
Abstract
Background:
Shoulder instability attributed to glenoid labral tears is common among National Collegiate Athletic Association (NCAA) football players. Certain repetitive activities by player position may contribute to instability.
Purpose:
To compare the location of labral tears among player positions in NCAA Division I football.
Study Design:
Cross-sectional study.
Methods:
We conducted a review of football players who underwent shoulder labral repair between 2000 and 2020 at a single institution. Inclusion criteria were NCAA Division I level, diagnosis of shoulder instability, and labral tear requiring arthroscopic repair. Exclusion criteria were prior surgery on injured shoulder and incomplete medical records. Players were divided into 3 groups: line players (offensive and defensive linemen, defensive end), skill players (defensive back, wide receiver, running back, and quarterback), and hybrid players (linebacker and tight end). Labral tear location and size were recorded using the clockface method and categorized into 6 zones: superior, anterosuperior, anteroinferior, inferior, posteroinferior, and posterosuperior. Comparison of variables was performed using chi-square test or Fisher exact test (categorical) and 1-way analysis of variance or Kruskal-Wallis H test (continuous). The Spearman rank-order correlation was used to assess relationships between continuous data.
Results:
Of the 53 included players, 37 (70%) were offensive linemen, defensive linemen, and linebackers. There were 29 line players, 11 skill players, and 13 hybrid players. Line players represented 55% of included players and had the most total labral tears as compared with all groups. Hybrid players had a significantly higher percentage of posterosuperior tears than line players (92% vs 52%; P = .015) and skill players (92% vs 27%; P = .002). Skill players had a significantly higher percentage of anterior tears at 3:00-4:00 and 5:00-6:00 when compared with hybrid players (82% vs 15%, P = .003; 82% vs 31%, P = .012, respectively). There was a positive correlation between labral tear size and number of suture anchors (0; P = .010).
Conclusion:
In this study of NCAA Division I football players, skill players had a higher proportion of anteroinferior labral tears, and hybrid players had a higher proportion of posterosuperior labral tears.
Shoulder instability is a commonly diagnosed condition in young contact athletes. 16 A diagnosis of instability can be detrimental to a competitive athlete’s future, as it can negatively affect performance attributed to pain, weakness, and/or recurrent instability. 4 Among high school and college sports, football records the highest number of shoulder dislocations, with the most common mechanism of injury being tackling. 15 Shoulder instability is one of the most common injuries sustained by National Collegiate Athletic Association (NCAA) athletes, with football accounting for 29% to 71% of these injuries. 27,28 While some players may experience only 1 dislocation or subluxation event, many have symptoms of recurrent instability as their labrum sustains repetitive trauma during tackling, blocking, and overhead activities. 9 Athletes may eventually return to play and overcome performance limitations; however, it is nearly impossible to avoid time away from sport owing to rehabilitation and possible surgical intervention. 6,9,21,25 In the NCAA, athletes have been reported to miss around 8 to 10 days of play because of shoulder instability, which is a substantial portion of a 13-week football season. 6,22,27 The vicious cycle of trauma, rehabilitation, bracing, and surgical intervention often afflicts collegiate-level players with hopes of pursuing positions at the professional level. 21 Therefore, studies focusing on epidemiology and risk factors in football players are meaningful, as they can help shape current treatment protocols and possibly lead to injury prevention.
At a recent National Football League (NFL) Combine, shoulder instability accounted for 24% of injuries sustained by college football players. 14 Among NCAA Division I football players with shoulder instability, anterior instability is more common than posterior instability, with reported rates up to 68% and 19%, respectively. 19 Epidemiologic studies have identified that anterior instability is more common among linebackers and defensive backs, while posterior instability more commonly affects linemen. At the collegiate level, linebackers and linemen more often require surgical stabilization and go on to have decreased chances of playing in the NFL and shorter professional careers. 4,5,14,19
Many studies have looked to identify risk factors for shoulder instability and recurrence by investigating glenohumeral anatomy, glenoid retroversion, and strength. 9,18 After arthroscopic intervention, higher recurrence rates have been reported for anterior instability (17%-51%) than for posterior instability (3%-8%). 3,11,17,23,26 Therefore, labral tear location may influence postoperative outcomes and failure rates. Additionally, player position has been suggested to contribute to shoulder instability as the result of the nature of joint position during contact while performing high-speed tackling, blocking, and catching. 14,19 Despite this, there is a paucity of literature identifying or comparing exact labral tear locations among football player positions.
The purpose of this study was to determine the prevalence of labral tears based on location and to compare the location and size of labral injury by position among NCAA Division I college football players who received arthroscopic shoulder surgery. The hypothesis was that there is a difference in labral tear location and size among the player positions.
Methods
After receiving institutional review board approval, we conducted a review of all college football players who underwent arthroscopic shoulder labral repair between 2000 and 2020 at a single institution (University of Pittsburgh). Each surgical procedure was performed by 1 of 3 fellowship-trained sports medicine orthopaedic surgeons (A.L., V.M.). Inclusion criteria were as follows: a football player at the NCAA Division I level, a diagnosis of shoulder instability, and a labral tear requiring arthroscopic surgical repair. For the purposes of this study, players were diagnosed with shoulder instability after experiencing ≥1 subluxation event or shoulder dislocation. Subluxation events were defined instability episodes that did not result in a formal shoulder reduction. Dislocation events were defined as instability episodes that required a formal shoulder reduction by a provider. Exclusion criteria were prior surgery on injured shoulder, open surgical repair, and incomplete medical records. Data collection was completed in December 2020. The following data were extracted from patient medical records into a precompleted form: patient demographics, intraoperative arthroscopic findings, and details of surgical intervention performed.
Position Groups
Players were assigned to 1 of the following groups: line players, skill players, and hybrid players. 1 The line players (offensive lineman, defensive lineman, and defensive end) often begin in a 3-point stance on the line of scrimmage, predominantly blocking and tackling. The skill players (defensive back, wide receiver, running back, and quarterback) rely on their speed and agility, while frequently performing overhead activities. The hybrid players (linebacker and tight end) require speed and strength to compete against linemen and skill players. 1
Labral Tear Location
Published studies in the literature use the clockface method to describe the location of injury about the glenoid. 8,12,20 This is often used among radiologists for imaging review and orthopaedic surgeons when describing operative findings. Regardless of laterality, the following clockface times always represent these positions on the glenoid: 12:00 (superior), 3:00 (anterior), 6:00 (inferior), and 9:00 (posterior) (Figure 1A). To estimate the size of labral tears, the clockface is transformed to degrees, with the region in between hour mark of the clock representing 30° of the labrum. 13 For this study, the glenoid was also divided per the clockface method into the following 6 zones to describe labral tear location: superior (11:00-1:00), anterosuperior (1:00-3:00), anteroinferior (3:00-5:00), inferior (5:00-7:00), posteroinferior (7:00-9:00), and posterosuperior (9:00-11:00). 8,20 Each zone represents 60° of the labrum (Figure 1B). The location and size of each labral injury were determined from surgeon operative reports and reported using the clockface method, which was later categorized to the 6 zones for the purpose of data analysis.

Methods of dividing glenoid for labral tears. (A) Clockface method. For right and left shoulders, 3:00 faces anteriorly and 9:00 faces posteriorly. The angle between each hour represents 30° of the labrum. (B) Six zones. Each zone represents 60° of the labrum.
Statistical Analysis
Categorical data were reported using count and percentage, with analysis performed using the chi-square or Fisher exact test, as applicable. The Shapiro-Wilk test was used to evaluate distribution of continuous data, with normally distributed variables presented as mean and standard deviation and nonnormally distributed variables as median and range. One-way analysis of variance or Kruskal-Wallis H test was used for comparing continuous variables as appropriate, depending on normality. A post hoc analysis with Bonferroni or Tukey-Kramer correction was performed, if deemed necessary, to assess which study cohorts were responsible for any significant findings. The Spearman rank-order correlation was used to assess relationships between continuous data. The correlation value (r S) was interpreted as follows: very weak (0-0.19), weak (0.2-0.39), moderate (0.4-0.59), strong (0.6-0.79), or very strong (0.8 -1.0). 10 Statistical significance was set at P < .05. Statistical analysis was performed using SPSS Version 26.0 (IBM).
Results
Player Characteristics
The initial chart review identified 62 NCAA Division I football players who underwent arthroscopic labral repair; however, 9 players were excluded after exclusion criteria screening. Five players were excluded for a history of shoulder surgery and 4 more players for operative reports without clockface description of labral tear location. The remaining 53 players (100% male) were included in data analysis, accounting for 9 positions: 21 (40%) offensive linemen, 9 (17%) linebackers, 7 (13%) defensive linemen, 5 (9%) defensive backs, 4 (8%) tight ends, 3 (6%) wide receivers, 2 (4%) running backs, 1 (2%) defensive end, and 1 (2%) quarterback. After players were assigned to position-based groups, there were 29 line players, 11 skill players, and 13 hybrid players (Table 1).
Player Cohorts Based on Position a
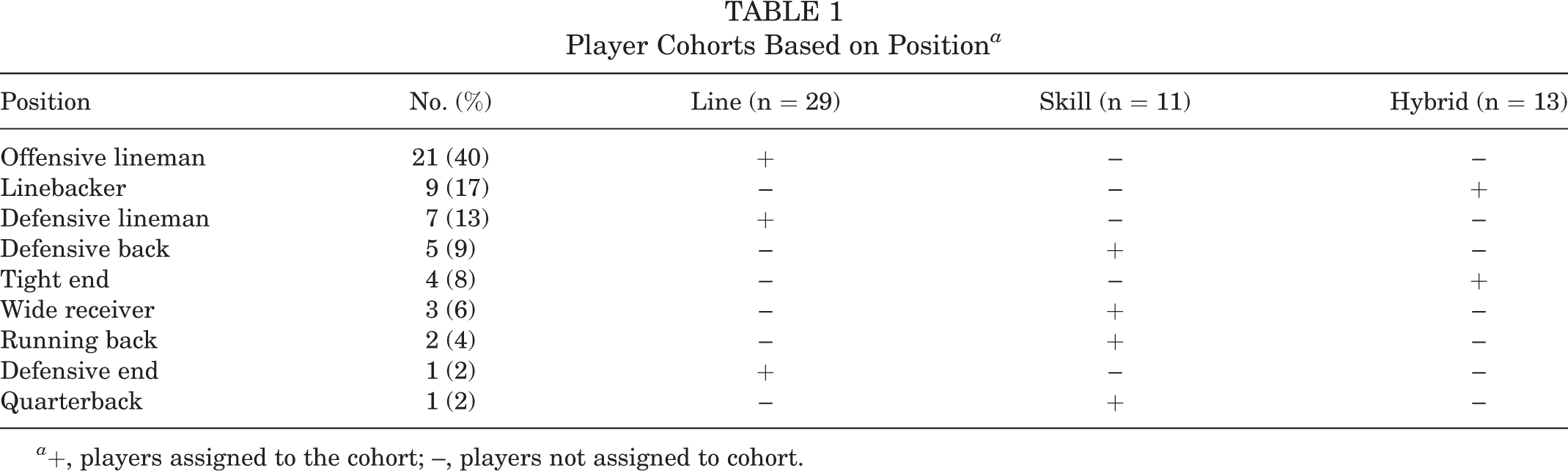
a +, players assigned to the cohort; –, players not assigned to cohort.
The mean age at the time of surgery was 20.1 ± 1.4 years with no statistically significant difference among groups (P = .570). The mean body mass index (BMI) was 32.1 ± 4.4 kg/m2, which was significantly different among the position cohorts: line players had a higher BMI than hybrid players and skill players (P < .001), and hybrid players had a higher BMI than skill players (P = .001) (Table 2). Overall, 39 players (74%) experienced subluxation events based on documented history and physical examination. Only 14 players (26%) sustained documented shoulder dislocations before surgical intervention. Of these 14 players, 8 experienced just 1 dislocation event, 3 sustained 2 dislocations, and 3 had ≥3 dislocations. Skill players sustained significantly more dislocations than hybrid players (P = .044). Regarding timing of surgery, 34 players (64%) underwent surgery during the offseason, with the remaining having surging during the regular season (P = .641).
Characteristics of the Football Players by Position Group

a-d Shared superscripts indicate significant differences between position groups after post hoc analysis (P < .05).
Labral Tear Location
Among line players, 66% of labral tears were noted in the posteroinferior zone. For skill players, 82% of labral tears were identified in the anteroinferior and inferior zones. Hybrid players had 92% of labral tears in the posteroinferior and posterosuperior zones (Figure 2). In the posterosuperior zone, there was a significant difference in percentages of labral tears among all position groups after pairwise comparison (P = .004). Further post hoc analysis revealed that hybrid players had a significantly higher percentage of posterosuperior tears than line (P = .015) and skill (P = .002) players. Although no other significant differences were noted among the remaining 5 zones, the anteroinferior zone had tear percentages of 39%, 48%, and 82% in hybrid, line, and skill players, respectively (P = .081) (Table 3).

Proportion of labral tears by location for position groups. Percentage of labral tears within each zone correspond to the legend. Dark green represents 0% and red 100%.
Location and Extent of Labral Tears by Position Group

a,b Shared superscripts indicate significant differences between groups after post hoc analysis (P < .05).
The clockface method allowed for further breakdown when analyzing tear locations. When all position groups were compared, significant differences in the proportions of labral tear based on location were reported at 3:00 to 4:00 (P = .005), 5:00 to 6:00 (P = .036), 7:00 to 8:00 (P = .046), and 9:00 to 10:00 (P = .015). The percentage of skill players with tears at 3:00 to 4:00 and 5:00 to 6:00 was significantly higher than hybrid players (82% vs 15%, P = .003; 82% vs 31%, P = .012, respectively). At the 9:00-10:00 position, hybrid players had a significantly higher percentage of tears than skill players (85% vs 27%; P = .005) (Table 3). After post hoc analysis with pairwise comparisons and Bonferroni correction, no significant difference was detected in the proportion of labral tears at 7:00 to 8:00.
Labral Tear Size
In all 53 players, labral tears spanned a median 150° with a range of 30° to 360°. Two line players and 1 skill player had full 360° circumferential tears. The mean number of suture anchors utilized for labral repair was 5.4 ± 2.0. There were no significant differences among position groups in regard to labral tear size (P = .735) and numbers of suture anchors used (P = .465) (Table 3). No significant correlation was found between number of dislocations and tear extension (P = .782) or number of suture anchors (P = .985). There was a strong significant positive correlation between labral tear extension and number of suture anchors (r S = 0.729; P = .010).
Discussion
In this 20-year study of NCAA Division I college football players who underwent arthroscopic shoulder surgery, hybrid players had the highest proportion of labral tears in the posterosuperior zone, which was significantly increased when compared with skill and line players (92% vs 27%, P = .002; 92% vs 52%, P = .015, respectively). Specifically, the clockface method revealed a significantly higher proportion of 9:00-10:00 tears among hybrid players as compared with skill players (85% vs 27%; P = .005). When compared with hybrid players, skill players had a higher proportion of tears in the anteroinferior zone, and further breakdown revealed significant differences at 3:00 to 4:00 and 5:00 to 6:00 (82% vs 15%, P = .003; 82% vs 31%, P = .012, respectively). Although line players had similar percentages among 5 of the 6 zones, the highest percentage of tears was noted in the posteroinferior (66%), inferior (59%), and posterosuperior zones (52%), respectively. The data findings support the hypothesis that labral tear location differs among player positions.
In the present study, linemen, linebackers, and defensive backs made up >70% of the player population undergoing labral repair. This finding is consistent with the literature revealing a higher incidence of arthroscopic labral repair in linemen and defensive backs in NCAA Division I players. 19 One study investigating football players at the NFL Combine performed analysis by position. Its data suggested that anterior instability primarily affected linebackers and defensive backs and that posterior instability was more significantly identified in linemen. 14 While there are similar findings regarding linemen and defensive backs in the current study, linebackers sustained more posterior than anterior tears. These differences may be due to small sample size and grouping of players for statistical analysis.
Hybrid players sustained no prior dislocations and had 92% of tears in the posteroinferior and posterosuperior zones. Line and skill players made up the 14 players who sustained dislocations, and these position groups had more tears in the anterosuperior and anteroinferior zones. Similarly, a recent retrospective study examined the incidence of labral repair in NCAA football players who sustained a subluxation or dislocation event. In the subluxation group, 67% of players required posterior labral repair. Anterior labral repair was required in 50% and 86% of players in the subluxation and dislocation groups, respectively. 28 In the current study, there were no significant predictive correlative findings with number of dislocations. However, future studies examining the relationship between dislocations and labral tear location may be warranted.
The use of 6 glenoid zones and the clockface method provided important detail regarding the specific location of labral tears and the extent of injury in patients with shoulder instability. While there were no significant differences in labral tear extension among players, tear sizes ranged from 30° to 360°. All included college football players had substantially sized labral tears on diagnostic arthroscopy that warranted repair with suture anchors. Reporting data using these methods results in a better understanding of the magnitude of labral injury and raises the question whether player position is a predictive risk factor for labral tear location.
There is a need for a better understanding of why specific positions may be more prone to tears in certain locations. Some studies suggest that linemen sustain posterior labral injuries because of the nature of blocking with forward flexed arms that sustain repetitive posterior loading forces across the labrum. 2,4 Regarding anterior labral injury, the literature suggests that it may be related to positioning the arm in abduction and external rotation as seen during pass rushing. 4,29 Although superior labrum anterior-posterior are mostly seen in overhead throwing athletes, 1 study reported that they most often occur in offensive linemen. 7 There is uncertainty regarding the mechanism behind this injury, as linemen frequently perform blocking and tackling actions. Future research focusing on the biomechanics of shoulder function in each player position could allow for better understanding of its labral injuries. This study suggests that certain player positions are at risk for specific locations of labral tears. This information could lead to the development of position-specific shoulder injury-prevention programs for football players, similar to those developed for overhead throwing athletes. 24 Developing exercise protocols and rehabilitation for each position may lead to decreased risk of shoulder instability.
Limitations
The main limitation of this study was its small sample size, which entailed the use of position groups for data analysis. This made it difficult to compare among individual positions. It is challenging to compare findings from the present data set and the current literature, as most published studies report incidence rates based on individual positions. A larger sample size and the addition of more institutions could result in more significant findings and allow for better extrinsic validity. Another limitation is the retrospective nature and the potential for selection bias. This study does not include players with labral tears experiencing instability that underwent nonoperative management or players with labral tears that were asymptomatic. Follow-up studies focusing on rates of recurrent instability and failure after arthroscopic labral repair are of particular interest.
Conclusion
The location of labral tears varied among positions for NCAA Division I football players undergoing arthroscopic labral repair. Line players made up 55% of the study population, and this group had the highest prevalence of labral tears in each size zone. However, when percentages were compared, skill players had a higher percentage of anteroinferior tears, and hybrid players had a higher percentage of posterosuperior tears. Labral tear size ranged from 30° to 360°, with larger tears requiring an increased number of suture anchors for repair.
Footnotes
Final revision submitted May 4, 2022; accepted August 2, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H. has received grant support from Arthrex, education payments from Pylant Medical and Smith & Nephew, and hospitality payments from SI-BONE. A.L. has received education payments from Mid-Atlantic Surgical Systems, consulting fees from Tornier/Stryker and Arthrex, nonconsulting fees from Arthrex, and honoraria from Wright Medical. V.M. has received educational grants, consulting fees, and speaking fees from Smith & Nephew and educational grants from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh (STUDY19030196).