
Abstract
Background:
There continues to be significant debate on how to manage traumatic rotator cuff tears in older patients.
Purpose:
To evaluate the clinical outcomes of patients ≥70 years who underwent arthroscopic repair of traumatic rotator cuff tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective review of prospectively collected data examined outcomes after arthroscopic rotator cuff repair in patients aged ≥70 years with traumatic full-thickness rotator cuff tears. The authors compared preoperative and postoperative outcomes, including American Shoulder and Elbow Surgeons (ASES) scores, Single Assessment Numeric Evaluation (SANE) scores, pain visual analog scale (pVAS) scores, and range of motion measures, as well as assessing postoperative complications.
Results:
A total of 31 patients met the inclusion criteria. The mean patient age at the time of surgery was 73.6 ± 3.3 years (range, 70-82 years), and the mean follow-up was 38.8 months (range, 24-99 months). The most common mechanism of injury was low-energy falls (87%), followed by motor vehicle collisions (13%). From preoperatively to postoperatively, ASES scores improved from 36.5 ± 15.5 to 95.2 ± 7.7, SANE scores improved from 41.13% ± 20.4% to 94% ± 10.26%, and pVAS scores improved from 7.74 ± 2.13 to 0.48 ± 1.03 (P < .0001 for all). A comparison of repairs performed at <6 months versus ≥6 months from injury yielded no statistically significant differences in ASES, SANE, or pVAS scores (P = .930, .445, and .806, respectively) or in forward flexion, external rotation, or internal rotation (P = .328, .063, and .811, respectively) at the final follow-up.
Conclusion:
Arthroscopic rotator cuff repair for traumatic full-thickness tears in patients aged ≥70 years demonstrated favorable clinical results. Surgery before or after 6 months of injury did not affect outcomes in this cohort. Surgical treatment should be strongly considered for traumatic rotator cuff tears in the elderly population.
Keywords
Rotator cuff tears are a common and frequent source of pain, impaired shoulder function, and reduced quality of life in the geriatric population, with incidences reported as high as 80% in patients >80 years of age. 12 An estimated 2.3% to 17.7% of older patients sustain traumatic rather than degenerative rotator cuff tears. 18,19,22 Most older individuals experience chronic degenerative tears characterized by insidious onset, repetitive use, and gradual deterioration.
There is significant debate on how to manage rotator cuff tears in an elderly population, with tears broadly occurring in either a degenerative or a traumatic fashion. In general, nonoperative treatments are commonly considered for first-line treatment of degenerative rotator cuff tears in the elderly. Nonoperative measures such as injections, anti-inflammatory medications, and physical therapy may yield short-term benefits, although an unrepaired rotator cuff tear, even if previously asymptomatic, continues to undergo potentially irreversible degeneration and fatty infiltration. 11,13,15,16 Surgical rotator cuff repair in elderly patients is accompanied by a number of concerns that portend poor outcomes: osteoporosis affecting anchor pull-out strength, preoperative corticosteroid injections, reduced cellular activity and healing response, higher rates of comorbidities, and most concerningly, high rates of rerupture after repair. 5,9,21,26 –28,30,35,37 However, patients with a history of trauma may be unique, as traumatic tears may theoretically have a better healing response. While studies show excellent outcomes and return to function after surgical repair as a first-line treatment of traumatic rotator cuff tears in younger patients, it is unclear if these results translate to an elderly population, given that the average age of patients with traumatic tears is typically younger and with a lower theoretical risk of repair failure. 23 –27
The purpose of this study was to evaluate the subjective and objective outcomes of patients aged ≥70 years who underwent arthroscopic repair of traumatic rotator cuff tears after a specific injury event. We hypothesized that arthroscopic rotator cuff repair in these patients would improve pain relief and functional outcomes while maintaining a low complication rate.
Methods
This study was determined to be exempt from institutional review board approval. The reporting of study findings was performed according to the Strengthening the Reporting of Observational Studies in Epidemiology recommendations. Prospective data were retrospectively collected from consecutive rotator cuff repairs in patients aged ≥70 years. All patients were referred from the emergency department after a traumatic event and evaluated with symptomatic tears severe enough to limit shoulder function. Patients with existing symptoms before the index traumatic event were not eligible for inclusion in order to exclude incidents of acute-on-chronic rotator cuff pathology. Additionally, patients were required to have imaging-confirmed full-thickness rotator cuff tendon tears and modified Goutallier grade ≤2 fatty degeneration, which is normal in this age group without degenerative tears. 11,15 Fatty grading was based on parasagittal T1-weighted magnetic resonance imaging (MRI) sequences: grade 0, no fatty infiltration; grade 1, some fatty streaks; grade 2, less fat than muscle; grade 3, as much fat as muscle; grade 4, more fat than muscle. 11 Imaging also showed acute muscle edema and wavy-like tendon appearance without chronic-appearing greater tuberosity changes.
All patients had undergone surgery by the senior author (N.P.), a shoulder and elbow fellowship–trained surgeon, at a single institution between June 2012 and January 2019 and had ≥2 years of follow-up. Patients with the following criteria were excluded: degenerative rotator cuff tears, acute-on-chronic tears, cuff tear arthropathy, modified Goutallier grade ≥3 fatty degeneration in any of the rotator cuff muscles, revision of prior rotator cuff repair, and comorbidities precluding surgical management. All patients underwent medical clearance and preoperative optimization before surgical intervention.
Surgical Procedure
Arthroscopic rotator cuff repairs were performed in a standardized fashion. After the administration of general anesthesia and an interscalene block, an examination under anesthesia was performed on all patients. Passive shoulder range of motion (ROM) in forward flexion, external rotation at the side of the body, external rotation in 90° of abduction, and internal rotation in 90° of abduction was recorded in addition to anterior and posterior stability. Patients were positioned in a modified beach-chair position with a SPIDER hydraulic arm holder (Smith & Nephew). All surgical procedures were performed arthroscopically. Five standard portals (posterior, anterior, lateral, anterolateral, and posterolateral) were used for diagnostic arthroscopy and surgical repair. Rotator cuff tears were defined according to the number of tendons torn and the size of the tear. After subacromial bursectomy, standard arthroscopic surgical principles were used to complete the rotator cuff repair, including mobilization of the rotator cuff and preparation of the greater and/or lesser tuberosity. The repair was performed using a suture bridge, double-row technique using biocomposite double-loaded anchors (Healicoil Regenesorb 5.5-mm suture anchors; Smith & Nephew) for the medial row and VERSALOK anchors (Depuy Synthes Mitek) for the lateral row. The type of repair and number of suture anchors were documented for each patient. Patients with concomitant shoulder pathology consistent with preoperative clinical examination underwent arthroscopic treatment of these pathologies in addition to rotator cuff repair.
Postoperative Rehabilitation
All patients were immobilized in a SmartSling (Ossur) using a 15° abduction pillow and were discharged home on the day of surgery. Elbow, wrist, and finger active ROM exercises were initiated after resolution of the interscalene block. Patients remained in slings with no active or passive motion of the shoulder for the first 6 weeks after surgery. Active and passive ROM exercises and formal physical therapy were initiated after 6 weeks and strengthening exercises after 12 weeks postoperatively. Return to full work, activity, and sport was allowed 6 months after surgery. Standardized follow-up occurred at 5 days, 12 days, 6 weeks, 12 weeks, 6 months, and 1 year postoperatively.
Outcome Evaluation
Per institution standards, outcome measures are prospectively collected as part of the standard of care at all patient visits. Outcome measures were divided into categories of patient-reported outcomes, ROM measurements, and complications. Patient-reported outcomes included American Shoulder and Elbow Surgeons (ASES), Single Assessment Numeric Evaluation (SANE; recorded in percentages), and pain visual analog scale (pVAS) scores. The 10-cm self-reported pVAS scale was used, in which 0 indicates no pain at all and 10 indicates maximum pain. ROM was collected in forward flexion and external rotation with a goniometer and in internal rotation by determining the highest vertebral level reached by the extended thumb.
Statistical Analysis
Statistical significance was defined as P < .05. Paired t tests were used to compare preoperative and postoperative patient-reported outcomes and ROM measurements. Rates of complications were collected and pooled for analysis. In addition, we used paired t tests to compare outcomes between repairs performed <6 months after injury (early repair group) versus ≥6 months after injury. A post hoc power analysis was performed with an alpha of .05 to determine differences between the groupings with 2-tailed t tests. All power analyses were performed using G*power (Heinrich-Heine-Universität Dusseldorf).
Results
Of the 381 patients who underwent arthroscopic repair of full-thickness rotator cuff tears during the study period, 75 (20%) were ≥70 years of age. Of these, 42 were excluded because of repair of degenerative tears and 2 were lost to follow-up, with a cohort of 31 patients available for final analysis (Figure 1). Post hoc power analysis found the study power to be 1.00 (100%) with an alpha set at .05, demonstrating sufficient power to determine statistically significant differences between the prerepair and postrepair groups as well as the early repair versus delayed repair groups.

Flowchart of patient selection.
The mean patient age at time of surgery was 73.6 ± 3.3 years (range, 70-82 years) with a mean follow-up of 38.8 months (range, 24-99 months). Time from injury to surgery averaged 5.8 months (range, 1-12 months), with 58.1% of surgeries occurring within 6 months of injury. The most common mechanisms of injury included low-energy falls (87.1%) and motor vehicle collisions (12.9%). Most patients were men (67.7%) with the injury involving the dominant arm (61.3%). Intraoperative records demonstrated tears predominantly classified as either massive (32.3%) or large (48.4%) according to the Cofield classification. 6 Repaired tendons included the supraspinatus (100%), infraspinatus (64.5%), and subscapularis (35.5%), with an average of 3.9 ± 1.5 anchors (range, 2-7 anchors). The most common concomitant procedures included arthroscopic subacromial bursectomy (100%), biceps tenotomy (64.5%), and arthroscopic acromioclavicular joint resection arthroplasty (35.5%) (Table 1).
Patient, Injury, and Surgery Characteristics a

a Data are reported as mean ± SD [range] or % (n). AAJRA, arthroscopic acromioclavicular joint resection arthroplasty; ASAD, arthroscopic subacromial bursectomy; COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease; MVC, motor vehicle collision.
All patient-reported outcomes demonstrated significant improvements in function and pain at the final follow-up. ASES scores increased from 36.52 ± 15.48 preoperatively to 95.16 ± 7.72 postoperatively, SANE scores increased from 41.13% ± 20.4% preoperatively to 94% ± 10.26% postoperatively, and pain levels on pVAS decreased from 7.74 ± 2.13 preoperatively to 0.48 ± 1.03 postoperatively (P < .0001 for all) (Table 2). The mean forward flexion and internal rotation did not significantly change after surgery. While a statistically significant improvement in external rotation was noted (preoperative: 62.74° ± 9.47°; postoperative: 67.58° ± 4.63°; P < .007), the small amount of improvement rendered this change unlikely to be clinically significant (Table 2).
Functional Outcomes and Active ROM After Rotator Cuff Repair a

a Data are reported as mean ± SD. Boldface P values indicate a statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
In addition to significant pre- to postoperative improvement, the functional scores far surpassed the standard minimal clinically important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) for rotator cuff repairs. 7,36 For ASES scores, all patients (n = 31; 100%) exceeded the MCID and PASS and a majority (n = 27; 87.1%) exceeded the SCB. For SANE scores, all patients (n = 31; 100%) exceeded the MCID and 93.5% (n = 29) achieved SCB and 87.1% (n = 27) met the PASS. For pVAS scores, all patients (n = 31; 100%) exceeded the MCID (Table 3).
Percentage of Patients Meeting the MCID, SCB, and PASS for Functional Scores a
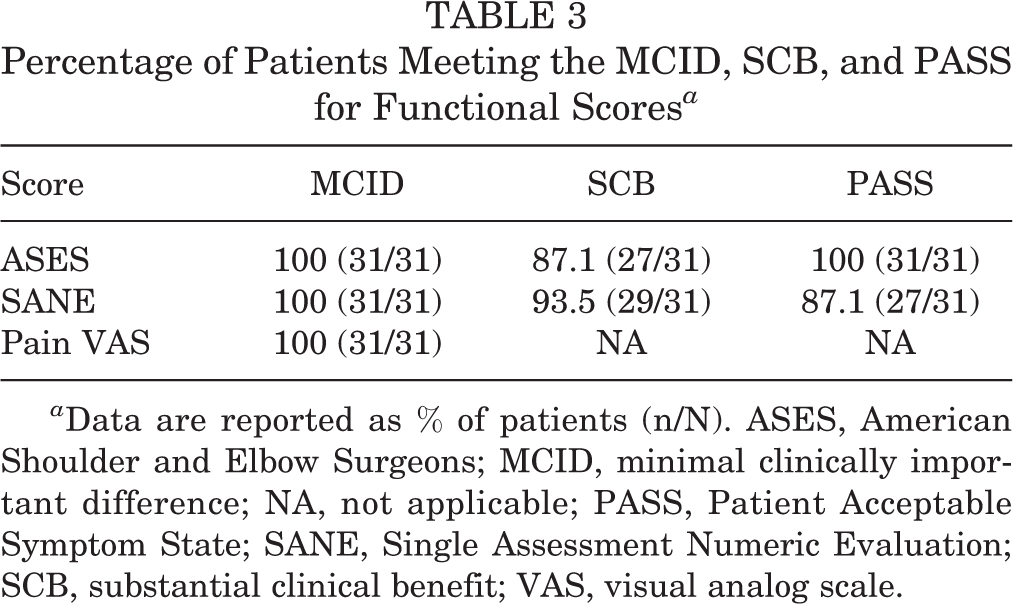
a Data are reported as % of patients (n/N). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; NA, not applicable; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
When comparing the early repair group with the delayed repair group, there was no statistically significant difference in patient-reported outcomes or ROM measures at the final follow-up (Table 4).
Functional Outcomes and Active ROM After Rotator Cuff Repair at Varying Time Points, Early (<6 months) or Delayed (≥6 months), From Injury to Surgery a

a ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Complications included 2 patients (6.5%) with a nonhealed rotator cuff tear visualized on MRI. Using the protocol of the senior author, MRI studies are ordered on patients with clinical concern for repair failure in the postoperative period. One patient was an 82-year-old who was evaluated with a massive tear at the time of surgery and underwent surgical treatment 3 months after a fall. At the end of the follow-up period (42 months), the patient had full passive ROM with 70° of active forward flexion. The patient had no pain and a SANE score of 50. The second patient was a 79-year-old who was similarly evaluated with a massive tear at the time of surgery and underwent surgical treatment 2.5 months after a fall. At the end of the follow-up (41 months), this patient had full passive ROM, 70° of active forward flexion, and weakness in abduction and external rotation. The patient remained pain-free with a SANE score of 80. Neither patient wished to pursue further surgery.
Discussion
Overall, our findings supported our hypothesis: arthroscopic rotator cuff repair of traumatic tears in patients ≥70 years of age yields substantial improvements in patient-reported outcomes measuring function and pain with a low rate of complications. These results challenge the belief that the risks associated with surgical repair of rotator cuff tears outweigh the benefits in elderly patients.
Most rotator cuff repairs in older patients address degenerative tears without a single traumatic event. 29,32 While some studies report good surgical outcomes in older patients with degenerative tears, 10,33 there is also evidence that demonstrates poor outcomes attributed to muscular atrophy and fatty infiltration. 14 Gwark et al 17 compared the structural and clinical outcomes after arthroscopic repair of degenerative rotator cuff tears in age- and sex-matched cohorts of patients older and younger than 70 years and found no significant difference in healing rates, retear rates, ROM, pain, muscle strength, and Constant scores, thereby demonstrating similar clinical outcomes between younger and older populations. They also found that the most significant factor associated with retear was preoperative tear size rather than age group. Similarly, Park et al 29 noted significant improvements in clinical outcomes after repair of degenerative rotator cuff tears in patients aged ≥75 years and determined that the size of the tear was the most important risk factor for retear. Specific to traumatic tears, a comparative study by Jeong et al 21 found that early repair of traumatic full-thickness rotator cuff tears results in statistically and clinically superior improvements in outcomes with a decreased incidence of retear compared with repair of degenerative rotator cuff tears. When considered alongside the results from the present study, these findings reinforce that arthroscopic rotator cuff repair should be considered a valuable treatment option for traumatic tears irrespective of patient age.
Prior studies on the characteristics of traumatic rotator cuff tears found high proportions of massive and large tears as well as frequent involvement of the subscapularis tendon. 1,20 The present investigation mirrors those studies, with >80% of our patients evaluated with massive and large tears and more than one-third requiring subscapularis tendon repair. Given that arthroscopic repair of massive rotator cuff tears, particularly those with subscapularis involvement, is a challenging procedure, some surgeons may err on the side of nonoperative treatment or arthroplasty. However, unlike repair of degenerative rotator cuff tears, repair of traumatic tears demonstrates excellent patient satisfaction, pain scores, ROM measures, strength, and outcome measures. 4
There are conflicting data regarding the recommended time from injury to repair for surgical management of traumatic rotator cuff tears. Early surgical intervention in these patients is hypothesized to result in better clinical outcomes because tissues are stout and mobile, thereby optimizing repair and healing. 4,8,18,22 The 1983 article by Bassett and Cofield 2 as well as the 2006 Swedish national guidelines 34 advocate for repair as early as 3 weeks after trauma, despite little evidence-based support for this guideline. Based on results suggesting comparable outcomes in patients undergoing repair 3, 6, or 12 weeks after surgery, Björnsson et al 3 recommend surgical treatment within 3 months of injury. Similarly, later studies consider early repair as surgery within 6 months of the trauma. 8,21 In the present study, both early (<6 months) and delayed (≥6 months) repair groups demonstrated clinically and statistically significant improvements in outcomes after repair of traumatic rotator cuff tears. Likewise, at the final follow-up, there was no significant difference in outcomes between the 2 groups (Table 4). These results support the notion that arthroscopic repair in patients ≥70 years with traumatic rotator cuff tears leads to successful postsurgical outcomes, even if delayed >6 months.
The only complication found in the current study involved retears in 2 patients (6.5%). This is comparable with the retear rates of former studies specific to arthroscopic repair of traumatic tears in younger patient populations, suggesting that this rate of retear is not specific to an older population. 4,8,31 Additionally, both patients who experienced retears were at the extreme end of the age group included in the study at 79 and 82 years. Despite how both patients exhibited weakness and significant active motion arc deficits, neither chose to undergo further surgeries, most likely because of the improvements in their pain.
Limitations
The limitations of the present study center around the bias expected of a retrospective review, including the lack of a blinded control group and the scoring of outcome data by members of the treatment team. Additionally, there is no comparison with other treatment options, specifically nonoperative management or alternative surgical treatments such as reverse total shoulder arthroplasty or shoulder spacer arthroplasty. These results are specific to a single, fellowship-trained surgeon and subsequently may have limited external validity in the context of varying surgical techniques, patient selection criteria, and/or rehabilitation protocols. Standardized advanced imaging was not universally obtained during follow-up. Without preinjury and postinjury imaging to confirm the diagnosis, it is difficult to distinguish an acute traumatic tear from a degenerative one with new-onset, acute symptoms after known trauma.
Conclusion
Arthroscopic rotator cuff repair for traumatic full-thickness tears in patients ≥70 years of age demonstrates favorable clinical results. Surgery before or after 6 months of injury did not affect outcomes in this cohort. Therefore, surgical treatment should be strongly considered for traumatic rotator cuff tears in the elderly population.
Footnotes
Final revision submitted July 11, 2022; accepted August 12, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.D. has received hospitality payments from Stryker. N.P. has received consulting fees from Mitek. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Carson-Carthage (ref. No. 2021-5).