
Abstract
Background:
Few studies have compared the force distribution between the anterolateral, posterolateral, and medial structures of the knee.
Purpose:
To investigate the important structures in an intact knee contributing to force distribution in response to anterior tibial load.
Study Design:
Controlled laboratory study.
Methods:
Nine fresh-frozen cadaveric knee specimens underwent robotic testing. First, 100 N of anterior tibial load was applied to the intact knee at 0°, 15°, 30°, 60°, and 90° of knee flexion. The anterior cruciate ligament (ACL), anterolateral capsule, lateral collateral ligament, popliteal tendon, posterior root of the lateral meniscus, superficial medial collateral ligament, posterior root of the medial meniscus (MM), and posterior cruciate ligament were then completely transected in sequential order. After each transection, the authors reproduced the intact knee motion when a 100-N anterior tibial load was applied. By applying the principle of superposition, the resultant force of each structure was determined based on the 6 degrees of freedom force/torque data of each state.
Results:
At every measured knee flexion angle, the resultant force of the ACL was the largest of the tested structures. At knee flexion angles of 60° and 90°, the resultant force of the MM was larger than that of all other structures with the exception of the ACL.
Conclusion:
The MM was identified as playing an important role in response to anterior tibial load at 60° and 90° of flexion.
Clinical Relevance:
In clinical settings, the ACL of patients with a poorly functioning MM, such as tear of the MM posterior root, should be monitored considering the large resultant force in response to an anterior tibial load.
Keywords
There are numerous studies investigating the role of knee structures in response to anterior tibial load. Although the primary stabilizer for an anterior tibial load is the anterior cruciate ligament (ACL), 17 secondary stabilizers such as the medial meniscus (MM) and medial collateral ligament (MCL) may also be clinically and biomechanically important. 4,16,19,25,27 Injuries to knee structures, including the MM, MCL, or lateral structures, were identified as risk factors for graft failure after ACL reconstruction. 7,12,15,28,29,31 In cadaveric studies, in situ forces of the native ACL or ACL-reconstructed graft increased in the absence of the MM or other structures. 4,11,20,26
The MM plays an important role in ACL-deficient knees. 1,2,14,19,22,24,25 Several studies have reported the importance of the MCL 3,4,17,32 ; the anterolateral complex, including the anterolateral ligament and anterolateral capsule (ALC) 21,23 ; the lateral collateral ligament (LCL) 20 ; and other structures. However, there is insufficient research investigating the role of these structures in ACL-intact knees. One study revealed that the force of the MM posterior root (MMPR) in intact knees was approximately 10 to 30 N in response to a 200-N anterior tibial load. 24 Another study demonstrated that the in situ forces of MCL and posterolateral structures were approximately 10 to 20 N in ACL-intact knees in response to a 134-N anterior tibial load. 17 As described in previous studies, these various structures are important for anterior stability. However, there are insufficient comparisons of the force distribution between several knee structures, including anterolateral, posterolateral, and medial structures, when an anterior tibial load is applied to an intact knee.
The purpose of this cadaveric study was to investigate the force distribution of the anterolateral, posterolateral, and medial structures of the knee in response to an anterior tibial load. We hypothesized that, outside of the ACL, the MM plays an important role in force distribution in response to an anterior tibial load.
Methods
Specimen Preparation
The study protocol to obtain, use, and dispose of fresh-frozen human cadaveric knees was approved by the ethics committee of our institution. Nine fresh-frozen knee specimens from 6 male and 3 female cadavers were used (mean age at death, 82.9 years; range, 70-90 years). The bodies were donated by individuals who had provided informed consent before their deaths. Physical examinations were performed before the biomechanical test to confirm ligamentous stability and range of motion from full extension to 130° of knee flexion. Specimens with ligamentous instability or loss of range of motion were excluded.
Specimens were thawed at room temperature for ≥24 hours before the test. Each specimen was wet during the test to avoid tissue deterioration. The femur and tibia were cut to ≥15 cm above and below the joint line, and the fibula was cut 5 cm below the proximal tibiofibular joint. The soft tissues, including the quadriceps and hamstrings, as well as the patella, were removed. The ligaments related to the knee joint, joint capsule, and meniscus were left intact.
Testing Apparatus
Both ends of the tibia and femur were fixed in a cylindrical mold using acrylic resin (Ostron II; GC). The fibula was fixed in its original position using the resin. Femoral and tibial cylinders were fixed with aluminum clamps and connected to the end-effector of a robotic testing system (FRS-2010; Technology Service) (Figure 1). 6 The robotic testing system was fitted with a custom-made 6 degrees of freedom (6 DOF) manipulator equipped with a universal force-torque sensor (DELTA IP65, SI-660-60; ATI Industrial Automation). The robotic system could simulate physiological knee joint motion with respect to the in vitro joint coordinate system developed by Grood and Suntay. 13 This system was controlled in real time by an original LabVIEW-based program (LabVIEW Version 12.0.1; National Instruments) for displacement and applying the force/torque to each axis.
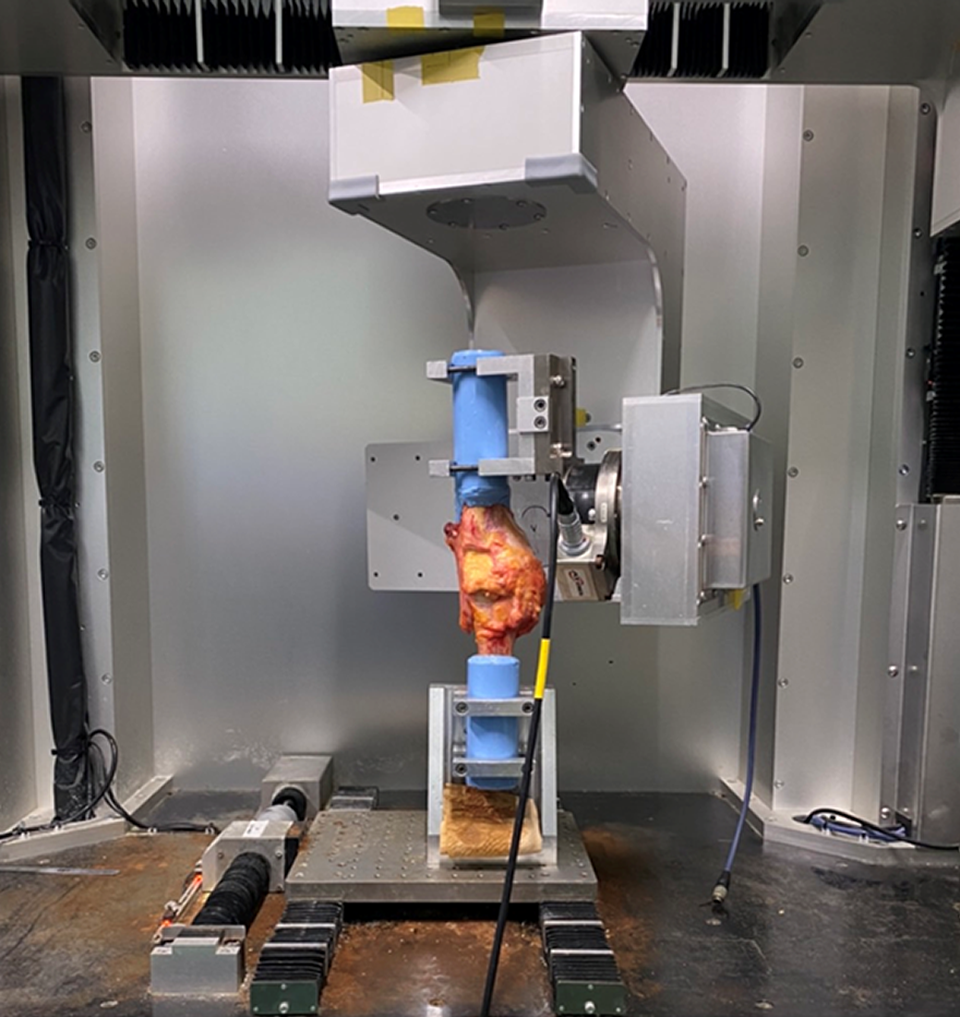
Robotic testing system with a right knee specimen. The manipulator, which works with a universal force-torque sensor, was placed on the end-effector. The tibia was fixed to the end-effector, and the femur was fixed to the lower part of the device using metal clamps.
Testing Protocol for the Intact State
First, a 0° flexion-extension axis was defined as when a 0.5-N·m extension moment was applied. Next, passive flexion-extension was performed from a hyperextended position to 120° of knee flexion using a 5-N·m extension moment. This method was applied at a rate of 0.5 deg/s and repeated 3 times as preconditioning. Finally, the anterior tibial load test was performed. A 100-N anterior tibial load was applied to the knee at 0°, 15°, 30°, 60°, and 90° of knee flexion. 10,30 During the test, the intact 6 DOF knee motion and force/torque were recorded.
Structure Transection
The ACL, ALC, LCL, popliteal tendon, lateral meniscus posterior root (LMPR), superficial MCL, MMPR, and posterior cruciate ligament (PCL) were completely transected in the stated order. The ACL, LCL, superficial MCL, and PCL were transversely cut at the midsubstance of the ligament. The ALC was divided just above the lateral meniscus. No obvious anterolateral ligament was observed in the specimens used in the present study. The popliteal tendon was transected just distal from the femoral attachment. LMPR and MMPR were transected 5 mm from the posterior root. In pilot studies, we compared total meniscectomy with the transection of the posterior root to determine the contribution of the medial and lateral menisci to load distribution. As a result, the posterior root tear completely lost the resultant force of the MM and LM in response to anterior tibial load, which is similar to a previous study in response to axial loading. 2 Thus, considering specimen damage from the cutting sequences of this experimental protocol, we selected the posterior root tear as a representative status when the meniscal function was completely lost.
Testing Protocol for the Transected State
By applying the principle of superposition, 8,9 the resultant force of each structure was determined based on the 6 DOF force/torque data of each state. First, we applied a 100-N anterior tibial load to the intact knee and recorded motion and force. After each transection, we reproduced the recorded intact knee motion when a 100-N anterior tibial load was applied and measured the forces to determine the resultant force of each structure (Table 1).
Experimental Protocol to Determine the In Situ Forces of Each Structure a

a ACL, anterior cruciate ligament; ALC, anterolateral capsule; LCL, lateral collateral ligament; LMPR, posterior root of the lateral meniscus; MCL, medial collateral ligament; MMPR, posterior root of the medial meniscus; PCL, posterior cruciate ligament.
Statistical Analysis
The resultant forces for each structure were analyzed using the Kruskal-Wallis test and the Steel-Dwass test. All analyses were performed using SPSS Version 28.0 (IBM) or EZR Version 1.55 (Saitama Medical Center, Jichi Medical University), a graphical user interface for R (The R Foundation for Statistical Computing) modified from R commander and designed to add statistical functions frequently used in biostatistics. 18 P < .05 was considered statistically significant.
Results
The resultant forces of the structures in the intact knee in response to the anterior tibial load are shown in Figure 2. At each knee flexion angle, the resultant force of the ACL was greater than that of the other structures. At >60° of knee flexion, the resultant force of the MM was larger than that of all other structures excluding the ACL.

Resultant forces of knee structures in response to anterior tibial loading. Error bars indicate SDs. Brackets indicate significant differences within each knee flexion angle. *Significantly greater than all other structures at each knee flexion angle (excluding other * structures). ACL, anterior cruciate ligament; ALC, anterolateral capsule; LCL, lateral collateral ligament; LMPR, posterior root of the lateral meniscus; MCL, medial collateral ligament; MMPR, posterior root of the medial meniscus; PCL, posterior cruciate ligament.
Discussion
This cadaveric study compared the resultant force of various structures in response to anterior tibial load in an intact knee. The most important finding of the present study was that the MM plays an important role when flexion is ≥60°.
A study by Markolf et al 24 showed a resultant force of 10 to 30 N with a 200-N applied anterior tibial load, which differs from the resultant forces of the 100-N load in this study. In the previous study, the MMPR force was determined by directly measuring the tensile force on the MMPR attachment using a force gauge. By contrast, in the present study, the resultant forces were calculated by applying the principle of superposition using force data obtained from the robot before and after transection of the structure. The method used in the previous study only enabled the determination of the tensile force of the attachment, whereas the method used in the present study evaluated the sum of all force contributions of the MM against a prescribed anterior displacement. In summary, only the tensile force was mainly evaluated in the study of Markolf et al, whereas the tensile, compressive, and shear forces were comprehensively evaluated in the present study. 8,9 As a result, the present study found greater resultant forces than the previous study.
At flexion angles of 60° and 90°, the resultant force of the MM was larger than that of the other structures except for the ACL. Although the resultant force of the ACL mainly contains tensile force, the resultant force of the MM may include tensile, compressive, and shear forces. Thus, the result of the present study does not conflict with previous reports that note that the ACL is most important with respect to the increase of anterior laxity. 5
Limitations
The present study had several limitations. First, the only investigated meniscal injury pattern was a posterior root tear. In pilot studies, medial and lateral posterior root tears showed nearly complete loss of the resultant force of the medial and lateral meniscus. Thus, we selected the posterior root tear as the meniscal injury pattern for near-complete loss of the resultant force in response to anterior tibial load. This was chosen to evaluate a single status condition and to avoid excessive damage to the specimen. Second, to investigate the resultant force of the ACL, a secondary stabilizer was transected first to calculate the force of the ACL in the secondary stabilizer–deficient state. However, only the effect of 1 structure could be investigated for 1 specimen in this method, and several structures could not be compared in the same specimen. Third, because the experiments were performed using specimens from older donors, there may be cases of poor bone quality and degenerative tendons. Although no obvious degenerative change was observed for the specimens of the present study, this may have been a source of bias. Fourth, because the results were obtained by in vitro tests, muscle forces and the contribution of the soft tissues, such as the anterior capsule and extensor mechanism that had been excised during specimen preparation, were not considered. Fifth, these tests were performed using only limited flexion angles, and other flexion angles were not evaluated. Sixth, the present study only evaluated knee flexion-extension forces in response to anterior tibial load. Additional evaluation of rotational stability would give more relevant data associated with real life. Seventh, in the transection stage the sequential cutting order was not randomized, which may be a potential source of bias. However, this biomechanical study’s data on the force distribution of structures in the knee may aid in understanding the biomechanics of the human knee joint.
Conclusion
Considering the results of the present study, ACL reconstruction with poor functional MM, such as a tear of the MMPR, should be carefully considered in clinical settings because of the large resultant force in response to anterior tibial load. Concomitant ACL and MMPR injuries are rarely found during arthroscopic observation at ACL reconstruction. However, the present results indicate that compared with other structures, both the ACL and the MMPR have larger force distributions in response to anterior tibial load at flexion angles ≥60°, suggesting that injury of either the ACL or the MMPR may lead to injury of other structures because of the loss of force distribution. This hypothesis should be further investigated.
Footnotes
Final revision submitted July 8, 2022; accepted August 12, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was partially funded by a MEXT/JSPS KAKENHI grant (JP 20K18035). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sapporo Medical University (reference No. 1-2-68).