
Abstract
Background:
In acute high-grade acromioclavicular (AC) joint injuries, the aim of treatment is robust reduction and stabilization of the joint. The anatomical landmarks method is most commonly used for stabilization, but loss of reduction often occurs because of the suture tunnels.
Purpose/Hypothesis:
The purpose was to evaluate and compare the stability of coracoclavicular (CC) stabilization using the anatomical landmarks and coracoid-based landmarks techniques in treating a high-grade AC joint injury. It was hypothesized that stabilization using coracoid-based landmarks would provide better stability.
Study Design:
Controlled laboratory study.
Methods:
Twenty fresh-frozen cadaveric shoulders (8 male and 2 female pairs) were randomized into 2 operative technique groups: 10 shoulders in the anatomical landmarks group and 10 shoulders in the coracoid-based landmarks group. The CC ligaments and AC capsule were cut at the midlevel, and CC stabilization and AC capsule repair were performed. For the anatomical landmarks technique, two 2.5-mm clavicular tunnels were created at 25 and 45 mm from the AC joint, while for the coracoid-based landmarks technique, two 2.5-mm clavicular tunnels were drilled using the medial and lateral borders of the coracoid base to choose the tunnel sites. Before injury creation and after stabilization, each shoulder underwent a loading force of 70 N in the superior and anteroposterior directions, and the displacement distance and stiffness were compared between the 2 techniques using the paired t test.
Results:
The mean difference in displacement before and after stabilization was higher in the anatomical landmarks technique than the coracoid-based landmarks technique (1.82 ± 3.52 vs –0.18 ± 4.78 mm in the superior direction and 7.47 ± 9.35 vs 1.76 ± 3.91 mm in the anteroposterior direction), but none of the differences in displacement or stiffness were statistically significant between the groups.
Conclusion:
No significant biomechanical differences in displacement or stiffness were seen between the anatomical landmarks technique and the coracoid-based landmarks technique.
Clinical Relevance:
Either stabilization technique can be utilized for repair of the CC ligaments in an acute AC injury setting.
Acromioclavicular (AC) joint injury is one of the most common shoulder injuries. 3,17 This injury can be divided into low-grade and high-grade AC joint injuries. The treatment of choice in acute high-grade AC joint injuries is surgery followed by coracoclavicular (CC) stabilization to provide extra support to the AC joint until complete ligament healing, while the method of treatment for the patient with a chronic injury is to reconstruct the native ligament using CC tunnels created based on various anatomical landmarks. There are several approaches to fix an acutely injured AC joint, such as CC stabilization and AC joint capsule repair, using either a distal clavicular locking plate or hook plate or tension band wiring with K-wires.
In the surgical technique of CC stabilization and AC capsule repair, 1,9 the double clavicular tunnel method has been found to have superior radiographic outcomes to the single clavicular tunnel method. 8,10 There are 2 preferred techniques in creating the double clavicular tunnels. In the first technique, the surgeon drills 2 clavicular tunnels using anatomical landmarks based on the natural conoid and trapezoid ligament insertions; this is called the anatomical landmarks technique. 19,22 In the second technique, the surgeon creates 2 clavicular tunnels perpendicular to the medial and lateral borders of the coracoid base, which is called the coracoid-based landmarks technique. The direction of the resulting sutures in these 2 techniques is different. The sutures in the anatomical landmarks technique are inserted in an oblique direction, which may result in less stability than the coracoid-based landmarks technique, in which the sutures are inserted in a vertical direction.
The purpose of this study was to evaluate and compare the efficacy of CC stabilization between the anatomical landmarks and coracoid-based landmarks techniques for treating high-grade AC joint injuries. We hypothesized that the coracoid-based landmarks technique would provide more stability than the anatomical landmarks technique, as the coracoid-based landmarks technique would result in less superior and anteroposterior displacement.
Methods
This was a biomechanical study using 10 matched pairs (20 specimens) of cadaveric shoulders that were obtained from Prince of Songkla university. There were 8 male and 2 female pairs (mean age at death, 66.5 ± 6.0 years), which were randomized into 2 groups: 10 shoulders in the anatomical landmarks group and 10 shoulders in the coracoid-based landmarks group.
Biomechanical Testing
Creating a Secure Base
All soft tissue was removed from each cadaveric scapula except for the CC ligaments and AC capsule, and the scapula was located centrally in a 10 × 10 × 10–cm aluminum box stabilized with 2 K-wires. Then the bottom half of the box was filled with epoxy resin to the level of the inferior half of the scapula. When the resin had cured, the scapula was removed from this box, and the proximal half of the clavicle was placed in the correct anatomical position in relation to the AC joint in a second, 5 × 5 × 5–cm aluminum box and fastened again with K-wires, and this box was again half filled with epoxy resin and allowed to cure.
Each base was securely fastened to a custom-made testing fixture with an array of M6 bolts (Figure 1A). The mold created to hold the scapular bone was fastened securely to the base of the testing fixture (Instron ElectroPuls E1000; Instron Corp), and the box created to hold the clavicle bone was fastened securely upside down to the upper level of the testing fixture.

The biomechanical testing setup showing the positions of the specimen-holding device in (A) frontal plane alignment and (B) transverse plane alignment. A, acromion process; C, clavicle; S, scapula.
Testing Setup
First, the scapular and clavicular bones were fastened in place in their respective boxes in the mechanical-testing instrument. Then 3 directions of displacement which consequently produced load—superior, anterior, and posterior, in that order—were applied to the upper testing box with the mechanical-testing instrument. Before testing each direction, a preload was applied to precondition the ligaments. We used a force of 70 N in both the vertical and horizontal directions to assess stability, based on previous studies. 7,13,15,24,25 A displacement rate of 1 mm/min was applied to the joint until the load cell force reached 70 N, and the displacement values and stiffness were recorded. Each joint underwent this process 3 times.
Because the force generated by the machine could be applied in only the superoinferior axis, for testing in the anteroposterior direction, the position of the testing device was changed from a frontal plane alignment (Figure 1A) to a transverse plane alignment (Figure 1B) by removing the clavicular bone from the testing fixture and rotating the base fixture through 90°. The clavicle was then again fastened securely to the testing fixture for testing with the anteroposterior load. A displacement rate of 1 mm/min was applied to the joint until the load cell force reached 70 N, and the displacement values and stiffnesses were recorded.
Study Groups
After randomization, a cadaveric shoulder was placed in the desired anatomical position in the mold in the stainless steel testing fixture and connected to the mechanical-testing instrument. Then, the AC capsule and CC ligaments were cut at the midlevel and the surgical CC stabilization and AC capsule repair were performed as described below.
For the anatomical landmarks technique, we first created two 2.5-mm clavicular tunnels at 25 and 45 mm from the AC joint (Figure 2A). 19,26 For the coracoid-based landmarks technique, we created two 2.5-mm clavicular tunnels centrally between the anterior and posterior edges of the clavicle using the medial and lateral borders of the coracoid base to identify the optimal placement of the tunnels (Figure 2B). In both techniques, CC stabilization was performed using 2 loops of ultra–high molecular weight polyethylene No. 5 suture (Arthrex), and the AC capsule was repaired with 3 cross-stitches using ultra-high molecular weight polyethylene No. 2 suture (Arthrex).

Coracoclavicular stabilization using the (A) anatomical landmarks and (B) coracoid-based landmarks techniques.
The final steps were the same for both techniques. The medial arm of the shuttle suture was passed through the medial clavicular tunnel, and the lateral arm of the shuttle suture was passed though the lateral clavicular tunnel. Two ultra–high molecular weight polyethylene No. 5 sutures were passed through the clavicular tunnel and looped underneath the coracoid base, again using a suture shuttle. The 4 ends of the 2 fiber wire sutures were then passed though the holes in a 4-hole small plate and tightened. The AC capsule was identified and reattached to the origin with 3 stitches using a ultra-high molecular weight polyethylene No. 2 suture.
After the CC stabilization and AC capsule repair, each shoulder was again tested with a loading force of 70 N (displacement rate of 1 mm/min) in the superior and anteroposterior directions as described earlier, and the displacement distances and stiffnesses were recorded.
Statistical Analysis
Evaluation between the study groups of the 2 continuous dependent variables (displacement distance and stiffness) before injury and after stabilization, as well as comparison of the changes in displacement and stiffness, was performed using the paired t test. A P value <.05 was considered significant. Statistical analyses were performed using the R program and the epicalc package (Version 3.4.3; R Foundation for Statistical Computing).
Results
There were no significant differences between the anatomical landmarks technique and the coracoid-based landmarks technique in mean displacement, in either the superior or the anteroposterior direction (P > .05 for both). Stiffness values were also similar between the 2 techniques (Table 1). There were also no statistically significant differences between the techniques in the changes to displacement or stiffness from before injury to after stabilization (P > .05 for both) (Table 2).
Comparison of Displacement and Stiffness Before Injury and After Stabilization Between Techniques a

a Data are reported as mean ± SD.
Comparison of the Changes in Displacement and Stiffness Before Injury and After Stabilization Between Techniques a
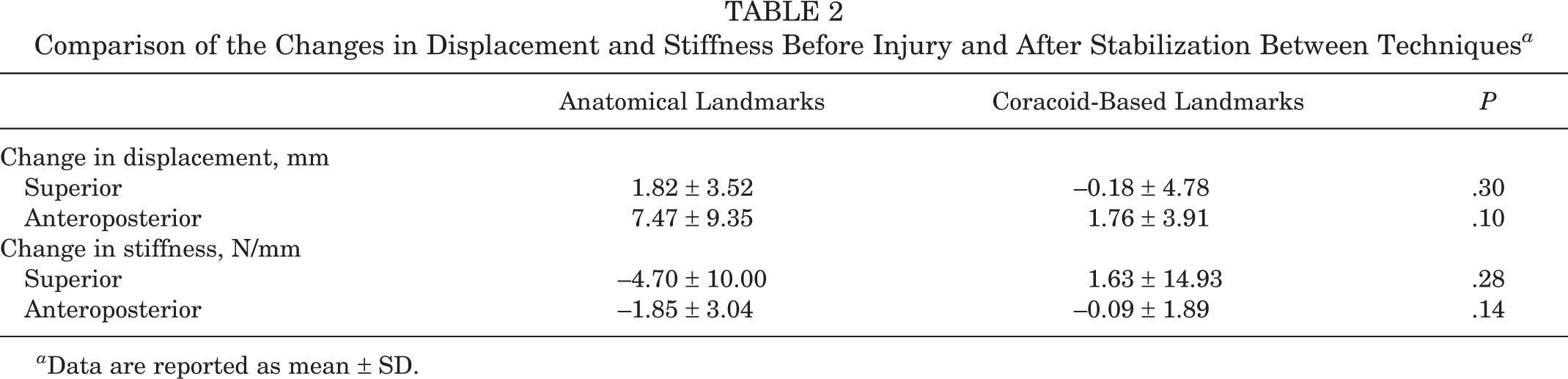
a Data are reported as mean ± SD.
Discussion
In this study, we found no significant differences in displacement or stiffness in either the superior or anteroposterior direction between the anatomical landmarks technique and the coracoid-based landmarks technique.
High-grade AC joint injuries are usually treated with CC stabilization and AC capsule repair or hook plate fixation. In CC stabilization and AC capsule repair, a number of studies have reported high incidences of superior displacement or loss of reduction after surgery of 5% to 50%. 4,5,12,18,23 The direction of the sutures is one of the important factors that affects postoperative reduction alignment. Seo et al 21 studied the outcomes of single-tunnel CC fixation and reported that an oblique suture direction was related to loss of reduction after surgery.
In CC stabilization, there are 2 features that the surgeon must consider. First is the coracoid process, in which the surgeon can create a tunnel or loop a suture under the coracoid base. Creating a tunnel is suitable for a large coracoid base, such as is generally found in Western populations, 14,19 but in East/Southeast Asian populations, this creates a risk of iatrogenic fracture due to the small size of the coracoid base. 6,11 For this reason, in East/Southeast Asian populations, most surgeons prefer to loop a suture under the coracoid base rather than creating a coracoid tunnel. The second feature is the clavicle, in which the surgeon can create 1 or 2 clavicular tunnels, with some studies reporting that the double clavicular tunnel method had better clinical and/or radiographic outcomes than the single tunnel method. 8,10 With the double clavicular tunnel method, most surgeons usually use the conoid and trapezoid ligaments as the anatomical landmarks for creating the 2 clavicular tunnels, although some surgeons create the 2 clavicular tunnels in relation to the medial and lateral borders of the coracoid base. In the anatomical landmarks technique, the sutures run in oblique directions, creating 2 major component forces that influence the tensile load and thus create a destabilizing force on the sutures. In the 2-dimensional coordinate system, the primary component forces are parallel and perpendicular and so do not create such a destabilizing force. The effect of the axial component force applied will normally be lower than that in the coracoid-based landmarks technique, resulting in less stability.
Our study compared the stability (the different displacements and stiffnesses) between creating clavicular tunnels related to the anatomical landmarks and creating clavicular tunnels related to the medial and lateral borders of the coracoid base, and we found no significant differences between the 2 techniques; however, in our clinical practice we prefer to create the clavicular tunnels based on the medial and lateral borders of the coracoid base because these landmarks are easy to identify while the anatomical landmarks of the CC ligaments have some variations in each patient.
The study findings suggest that the surgeon can successfully use the coracoid-based landmarks technique in the acute setting; however, caution should be exercised with chronic cases. There is a general consensus that either autograft or allograft should be used for CC ligaments and AC capsule reconstruction in chronic AC joint stabilization 20 because using only strong sutures has a chance of surgical failure. Carofino and Mazzocca 2 used the anatomical technique in treating chronic AC joint injury. They used a combined high-strength nonabsorbable suture and a semitendinosus allograft/autograft or anterior tibialis allograft to reconstruct the CC ligaments and superoanterior part of the AC capsule. In 2019, Muench and colleagues 16 reported the clinical and radiographic outcomes using the surgical technique of Carofino and Mazzocca in treating acute and chronic AC type 3 and 5 injuries and reported that both the clinical and the radiographic outcomes were improved compared with the preoperative clinical and radiograph situations, and 81% of the patients achieved substantial clinical benefit after surgical treatment with this technique. This result supports the suggestion that the surgeon should add either allograft or autograft to reconstruct the CC ligaments and AC capsule in treating chronic AC joint injury.
Limitations
There were some limitations to this study. First, the findings of a biomechanical study may not correspond to actual patients with high-grade AC joint injuries because the deltotrapezial fascia is usually repaired in actual cases, which we were unable to do in the cadaveric biomechanical study, and the strength of the fixation is usually weaker in actual cases because of this. Second, we could not assess the healing process after surgery, which affects postoperative stability. Third, in this study, we tested the superior, anterior, and posterior motions, which are the main motions of the AC joint; however, there are other motions we did not test, such as AC joint rotation. Fourth, we did not reconstruct the CC ligaments and AC capsule before testing the stability; thus, the results of this study cannot be applied to chronic AC joint injuries treated with CC ligaments and AC capsule reconstruction. Fifth, this study did not test cyclic loading or load to failure, which are also important considerations when deciding on tunnel placement.
Conclusion
No significant biomechanical differences were found in displacement or stiffness between the coracoid-based landmarks technique and anatomical landmarks technique for repair of the CC ligaments in an acute AC injury model. Either technique can be utilized in the acute setting with comparable outcomes.
Footnotes
Acknowledgments
The authors sincerely thank Boonsin Tangtrakulwanich of the Department of Orthopedics and Jirawan Jayuphan of the Epidemiology Unit, Faculty of Medicine, for providing statistical support; Bancha Chernchujit of the Department of Orthopedics, Faculty of Medicine of Thammasat University, for his suggestions in comparing these techniques; Chittipong Tipbunjong (head of the Department of Anatomy) and his assistants in the Department of Anatomy, Faculty of Science, for supplying the cadavers; Konwarat Ninlachart for assistance with the demonstration drawings; and Dave Patterson for his editing support.
Final revision submitted August 1, 2022; accepted August 10, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Prince of Songkla University (reference No. REC 62-258-11-1).