
Abstract
Background:
The postoperative failure rate of acromioclavicular (AC) joint fixation using the coracoclavicular (CC) stabilization technique is high. Studies have reported that compared with normal intraoperative anatomic reduction, intraoperative overreduction of the AC joint is more successful in achieving a satisfactory anatomic radiographic outcome at 1- to 2-year follow-up.
Purpose:
To evaluate the functional and radiographic outcomes and complications in patients with acute AC joint injury who underwent combined CC stabilization and AC capsular repair in which the CC distance was intraoperatively decreased to 50% of the unaffected side.
Study Design:
Case series; Level of evidence, 4.
Methods:
In this retrospective study, we collected and analyzed the data of patients with an acute AC joint injury (Rockwood type 5) who underwent combined CC stabilization and AC capsular repair during which the CC distance was decreased 50% compared with the unaffected side. At 2-year follow-up, we evaluated functional outcomes (American Shoulder and Elbow Surgeons [ASES] score), radiographic outcomes (alignment of the AC joint in the vertical and horizontal planes, tunnel widening), and complications (infection, clavicular fracture).
Results:
The study included 20 patients with a mean ± SD age of 42.20 ± 10.10 years. The mean follow-up period was 33.75 ± 11.50 months. At the 2-year follow-up, the mean ASES score was 95.13 ± 5.61. The overreduction alignment, anatomic alignment, and loss reduction alignment rates were 0% (0/20 patients), 95% (19/20 patients), and 5% (1/ 20 patients), respectively. No statistically significant difference was found in the mean CC distance between the affected and unaffected sides on radiographic evaluation. The mean medial clavicular tunnel width and lateral clavicular tunnel width were 5.03 ± 0.68 mm and 4.47 ± 0.67 mm, respectively. None of the patients experienced fractures or infections.
Conclusion:
Excellent functional and radiographic outcomes and no complications were seen at 2-year follow-up in patients with acute AC joint injury who underwent combined CC stabilization and AC capsular repair with the CC distance intraoperatively decreased to 50% of the unaffected side.
Keywords
Acromioclavicular (AC) joint injury is one of the most common shoulder injuries. AC joint injuries are usually classified based on the Rockwood classification. 3 In Rockwood type 5 AC joint injuries, the principle of treatment is to maintain the AC joint by healing the coracoclavicular (CC) ligament and the AC joint capsule. There are several approaches to AC joint fixation, such as CC stabilization and AC joint capsular repair, plate and screw fixation, hook plate fixation, and tension-band wiring. A combined CC stabilization and AC joint capsular repair is one of the most popular surgical options. 2,12 However, although the surgeon can achieve stability of the AC joint through fixation, this method entails some problems. Several studies have reported postoperative loss of reduction alignment of the AC joint and clavicular tunnel widening. 7,16,19,28,31,34 These complications can occur in both acute and chronic AC joint injury.
In AC joint injury, 2 factors can affect postoperative reduction alignment. First, the anteroposterior and superior instability of the AC joint can increase the strain on sutures after CC stabilization. If the sutures fail before complete ligament healing, there will be some loss of reduction alignment. Second, the quality of ligament healing has been reported to be inferior compared with the healthy ligament. 13,14 Other studies examining this problem have reported a 21% to 50% loss of reduction alignment in acute AC joint injury using CC stabilization. 4,7,27,30 In recent years, various methods to counteract this loss have been proposed. Maziak et al, 21 for example, studied factors that could predict the outcome of arthroscopic-assisted CC stabilization and reported that overreduction of the AC joint led to more favorable radiological outcomes than anatomic reduction or underreduction. Clavert et al 7 compared the CC distance between the affected and unaffected sides in the same procedure at 1-year follow-up and found that the incidence of radiographic failure was 41.3%, with the average CC distance of the operatively treated side 50% greater than the unaffected side. Because of the high incidence of radiographic failure and the good radiographic outcomes noted in patients with overreduction, some surgeons began to experiment with intraoperative overreduction of the AC joint in patients with Rockwood type 5 AC joint injury. To address the problem of radiographic failure in our own practice, we decided to review a series of overreduction cases to assess whether this method was better.
Some studies have reported that overreduction of AC joint fixation led to better radiographic outcomes than anatomic reduction or underreduction, 21 but to date no studies have conducted a statistical evaluation of the ratio of the CC distance on the affected side relative to the CC distance on the unaffected side. The aim of this study was to evaluate the functional outcomes, radiographic outcomes, and complications of combined CC stabilization and AC capsular repair that included intraoperatively decreasing the CC distance to 50% of that on the unaffected side. We hypothesized that good functional outcome and satisfactory anatomic alignment of the AC joint at 2-year follow-up could be achieved in patients with Rockwood type 5 AC joint injuries after this procedure.
Methods
This was a retrospective study of patients who had received a combined CC stabilization and AC joint capsular repair between January 2013 and April 2018. This study was approved by the ethics committee of our university. The study included the records of patients with an acute (<3 weeks) Rockwood type 3 and 5 AC joint injury who were aged between 18 and 65 years and had at least 2 years of postoperative follow-up. The exclusion criteria were a history of any type of fracture around the shoulder area, a history of shoulder surgery, or <2 years of follow-up recorded. A total of 22 patients were initially considered, of whom 2 patients were classified as Rockwood type 3 AC joint injury, leaving 20 patients in the final study population. A standard form was used to record demographic and clinical data (age, sex, side of operation, mechanism of injury, time to surgery, and follow-up period), medical comorbidities (diabetes mellitus, hypertension, dyslipidemia), functional outcomes (as assessed by the American Shoulder and Elbow Surgeons [ASES] score), radiographic outcomes (alignment of the AC joint in vertical and horizontal planes, tunnel widening, calcification of the CC ligaments and AC capsule, and AC joint osteolysis), and complications (superficial and/or deep infections, clavicular fracture). Radiographs conducted on postoperative day 2 were used to evaluate the original alignment of the reductions, and radiographs conducted at 2-year follow-up were assessed to determine the vertical and horizontal instability.
Surgical Technique and Postoperative Care
All surgeries were performed by a single experienced shoulder orthopaedic surgeon (P.K.). The combined CC stabilization and AC capsular repair began with the patient in the beach-chair position. A 5-cm saber incision was made from the distal clavicle, extending to the coracoid process. The incision was centered 2 cm medial to the AC joint. The deltoid muscle was identified and split to expose the coracoid process. The medial and lateral borders of the coracoid base were identified. An Ethibond No. 2 suture (Ethicon) was used to create a loop around the coracoid base and behind the coracoacromial ligament from the medial aspect to the lateral aspect of the coracoid base. In this step, the surgeon must be careful because of the neurovascular structures (subclavian artery, subclavian vein, and brachial plexus) located medially and close to the coracoid process. 6 The suture was then replaced with a shuttle loop using a shuttle relay technique.
For the operation on the clavicle, the full thickness of the deltoid trapezial fascia was excised in the longitudinal plane, and the fascia was peeled off the clavicle bone with a periosteum elevator. A double length of Ethibond No. 5 suture (Ethicon)was formed, and the loop end of the suture was passed underneath the coracoid base using a shuttle relay suture and then pulled upward and passed around the anterior of the clavicle. The other end of the double loop was passed around the posterior end of the clavicle (Figure 1A). The AC joint dislocation was then reduced by lifting up the patient’s arm, and the suture was tightened to maintain the reduction (Figure 1B). The alignment was checked using a fluoroscope. In the CC stabilization step, 2 clavicular tunnels were created using a 2.5-mm drill bit: a lateral clavicular tunnel 1.5 cm from the AC joint and a medial tunnel 2.5 cm from the joint (Figure 1C). The medial limb of the shuttle suture was passed through the medial clavicular tunnel, and the lateral limb of the shuttle suture was passed though the lateral clavicular tunnel. Next, 2 sutures of FiberWire No. 5 (Arthrex) were passed through the clavicular tunnel and looped underneath the coracoid base using a shuttle suture. The 4 ends of the 2 FiberWire sutures were passed though the holes in a small 5-hole plate and tightened (Figure 1, D and E).

The steps of coracoclavicular (CC) stabilization and acromioclavicular (AC) capsular repair used in the study. (A) A double length of Ethibond No. 5 suture is formed, and the loop end of the suture is passed underneath the coracoid base using a shuttle relay suture, pulled upward, and passed around the anterior of the clavicle. The other end of the double loop is passed around the posterior end of the clavicle. (B) The AC joint dislocation is then reduced and the suture tightened to maintain the reduction. (C) Two clavicular tunnels are created using a 2.5-mm drill bit: a lateral clavicular tunnel 1.5 cm from the AC joint and a medial tunnel 2.5 cm from the joint. The 4 ends of the 2 FiberWire sutures are (D) passed though the holes in a small 5-hole plate and (E) tightened. (F) The AC capsule is identified and reattached to the origin with Ethibond No. 2 sutures.
The alignment of the AC joint was overreduced by decreasing the CC distance to 50% of the unaffected side and checked under a fluoroscope with a scale radiopaque ruler in anteroposterior view. No formal attempt was made to repair or reconstruct the CC ligaments. Distal clavicle excision was not performed. The AC capsule was identified and reattached to the origin using Ethibond No. 2 sutures (Figure 1F), and the deltoid fiber was repaired with Vicryl No. 3-0. The skin was then closed layer by layer.
Each patient was advised to use an arm sling for 6 weeks after the surgery. Passive-assisted and active-assisted abduction and forward elevation were limited to 30° for 2 weeks, 45° for another 2 weeks (weeks 3-4), and 60° for a further 2 weeks (weeks 5-6). Active motion exercise of the shoulder was then started at 6 weeks postoperatively, and stretching exercises were begun at 8 weeks after surgery. The patient was allowed to return to full normal activities after 3 months.
Clinical Evaluation
All patients enrolled in the study were evaluated for a minimum of 2 years, at which time the ASES questionnaire was administered by a physician assistant who was blinded to the patient’s history and was not on the author team.
Radiological Evaluation
We evaluated the reductions using radiographs in both vertical and horizontal alignments. In the vertical alignment, we compared the anteroposterior view of both clavicles without load on postoperative day 2 (Figure 2) and with a 10-kg load at the 2-year follow-up (Figure 3). For the horizontal evaluation, we evaluated the radiographs of the affected shoulder without load in a transaxillary view. All measurements were made using radiographs from the hospital picture and archiving system. The accuracy of measurement was ±0.01 mm. The CC distance of both sides was defined as the shortest distance between the uppermost coracoid process and the inferior border of the clavicle in millimeters (Figures 2 and 3). The quality of the radiographs was somewhat inconsistent because of differences in the patient’s position, the distance between the patient and the x-ray beam, and the degree of beam tilting, which can influence the CC distance on the radiographic measurement. We tried to minimize the potential errors arising from this problem by comparing the CC distance on the affected side relative to the unaffected side (Figures 2 and 3).

A 2-day postoperative anteroposterior radiographic image of both clavicles showing the coracoclavicular distance between the uppermost section of the coracoid process and the inferior border of the affected (yellow line) and unaffected clavicles (white line). Analysis was based on the ratio of the coracoclavicular distance on the affected side (A, yellow line) relative to the coracoclavicular distance on the unaffected side (B, white line) = (A/B). In this example, the ratio is 0.42.

A 2-year postoperative anteroposterior radiographic image of both clavicles showing the coracoclavicular distance between the uppermost section of the coracoid process and the inferior border of the affected (yellow arrow) and unaffected clavicles (white arrow). Analysis was based on the ratio of the coracoclavicular distance on the affected side (A, yellow arrow) relative to the coracoclavicular distance on the unaffected side (B, white arrow) = (A/B). In this example, the ratio is 0.91.
Regarding vertical alignment, we classified the reductions as overreduction alignment, anatomic reduction alignment, and loss of reduction alignment based on the ratio of the CC distance on the affected side relative to the CC distance on the unaffected side. The alignment was classified as overreduction when the ratio was <0.9, as anatomic reduction when the ratio was between 0.9 and 1.1, and as loss of reduction when the ratio was >1.1. The percentage of patients included in each category at 2-year follow-up was calculated.
The horizontal alignment was evaluated according to the measurement method described by Rahm et al 27 (Figure 4). First, a line (L1) was drawn through the middle part of the distal clavicle. The most anterior part of the distal clavicle was identified, and then a second line (L2) was drawn passing this point and parallel to L1. A third line (L3) was drawn through the tip of the acromion process parallel to L1. Then, the shortest perpendicular distance from L2 to L3 was measured (in mm). In the horizontal plane, horizontal instability was defined as a difference of >7 mm between the most anterior part of the distal clavicle and the tip of the acromion process. The reference distance of 7 mm was based on the average distance in the study by Rahm et al.
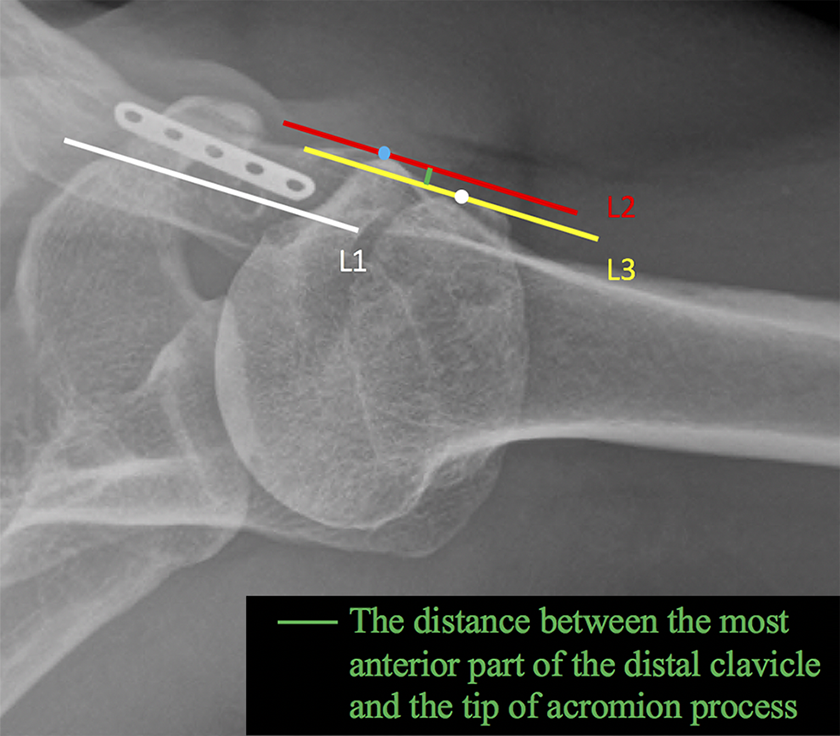
A 2-year postoperative transaxillary radiographic image of an affected shoulder. To evaluate horizontal instability, a line (white; L1) was drawn through the middle part of the distal clavicle. The most anterior part of the distal clavicle (blue dot) was identified, and then a second line (red; L2) was drawn passing this point (blue dot) and keeping parallel to L1. A third line (yellow; L3) was then drawn through the tip of the acromion process (white dot) parallel to L1, and the shortest distance from L2 to L3 (green line) was measured.
The widths of the clavicular tunnels were measured from an anteroposterior view of the affected shoulder on postoperative day 2 and at the 2-year follow-up at the midmedial and midlateral areas (in mm). Any calcification of the CC ligaments and AC capsule, AC joint osteolysis, or postoperative clavicular fractures were identified and recorded using radiographs of the affected shoulder taken at the 2-year follow-up (Figure 5).

A 2-year postoperative anteroposterior radiographic image of an affected shoulder showing the area of measurement at the midmedial (green arrow) and midlateral (white arrow) sections of the clavicular tunnel.
Statistical Analysis
To minimize measurement bias, all distances were measured 3 times by an experienced orthopaedist who was not on the author team, and the mean ± SD of these 3 measurements was used. Statistical analysis was performed with the R program and “epicalc” package (Version 3.4.3; R Foundation for Statistical Computing). The differences between the CC distance on the affected and unaffected sides were analyzed using unpaired t test. Statistical significance was set at P ≤ .05.
Results
Study Population
This study included 20 patients (12 men and 8 women) who had a mean age of 42.20 ± 10.10 years. The medical comorbidities were type 2 diabetes mellitus in 2 patients (10%), dyslipidemia in 2 patients (10%), and hypertension in 3 patients (15%). The duration of follow-up was 33.75 ± 11.50 months and ranged from 24 to 60 months. The side of operation was the left shoulder in 10 patients and the right shoulder in 10 patients. The mechanism of injury was traffic accident in 17 patients (85%) and sports injury in 3 patients (15%). The surgical reductions were performed at a mean of 7.60 ± 3.00 days after the injury. The mean ratios of the affected to the unaffected side were 0.52 ± 0.13 on postoperative day 2 and 1.05 ± 0.24 at 2-year follow-up. The mean functional ASES score was 95.13 ± 5.61 at the 2-year follow-up.
Each distance in this study was measured 3 times by a single experienced orthopaedist. The intraobserver reliability of the measurements was >0.9.
Radiologic Outcomes
At 2-year follow-up, the mean CC distances in the affected and unaffected shoulders were 9.00 ± 1.83 and 8.75 ± 1.84 mm, respectively, a difference that was not statistically significant (P = .38). The mean distance between L2 and L3 was 1.11 ± 0.97 mm. One patient had both vertical and horizontal instability. The percentage of patients with overreduction alignment, anatomic alignment, and loss of reduction alignment in the vertical plane was 0% (0/20 patients), 95% (19/20 patients), and 5% (1/20 patients), respectively. In the horizontal plane, 1 patient (5%) had posterior instability. The mean medial clavicular tunnel width and lateral clavicular tunnel width were 5.03 ± 0.68 mm and 4.47 ± 0.67 mm, respectively, at the 2-year follow-up. There were 2 patients with AC osteolysis.
Complications
No patients had experienced wound infection or postoperative clavicular fracture at the 2-year follow-up.
Discussion
Overreduction of the AC joint by intraoperatively decreasing the CC distance to 50% of the unaffected side resulted in good functional and radiographic outcomes at 2-year follow-up in this study.
Loss of reduction alignment after AC joint fixation with CC stabilization is one of the most common complications of this procedure, 20,29 but it may not be correlated with worse outcomes, as defined by many studies. 1,7,18,24,25 One study reported a 21% to 50% incidence of loss of reduction alignment with this procedure. The authors of that study hypothesized that the problem resulted from slippage of the suspension sutures and/or the postoperative clavicular tunnel angle leading to tunnel widening. 28
There are 2 common techniques used in CC stabilization: the single clavicular tunnel technique and the double clavicular tunnel technique. The double-tunnel technique has fewer complications than the single-tunnel technique and has a higher success rate in terms of clinical and radiographic outcomes. The traditional mode of dealing with an AC joint reduction has been the basic anatomic reduction. Tunnel position is another factor that has been related to failure in CC stabilization. The surgeon should avoid medializing the clavicular tunnel. 8,10 Cook et al 8 reported that no failures occurred if the conoid tunnel was <25% of the clavicular length from the lateral edge of the clavicle. In the current study, we created the trapezoid and conoid clavicular bone tunnels at 1.5 mm and 2.5 mm from the lateral edge of the clavicle, respectively. We placed the conoid tunnel <25% of the clavicular length from the lateral edge of the clavicle because the mean clavicular length of the Thai population is 152.3 ± 8.4 mm. 5
However, overall, this procedure has an unacceptably high rate of reduction failure. In recent years a new “overreduction” method has emerged, in which the normal loosening of the sutures after a normal reduction, causing loss of alignment, is countered by increasing the strain on the sutures, thus intentionally causing an overalignment during the procedure, which will then slowly return to the correct place as the sutures loosen. Stein et al 31 examined anatomic reduction of the AC joint and found that the incidence of postoperative loss of reduction alignment was 26.55%. Maziak et al 21 studied radiographic outcomes in acute high-grade AC joint injuries using arthroscopic-assisted CC stabilization and found that although 4% of the overreduced joints (CC distance of the affected side less than that of the unaffected side) remained overreduced, 69% of the overreduced joints had migrated to the correct anatomic position (CC difference = 0) or nearly correct anatomic position (CC difference = 1-2 mm). In patients with standard anatomic reduction of the AC joint, the alignment stayed in the correct position in only 41% of the cases. Clavert et al 7 studied the displacement of CC distance in patients with fixation failure and found that the average CC distance in these cases was 50% higher than the unaffected side, which would be attributable to loosening of the sutures by increased strain on them after CC stabilization.
In our study, we performed combined CC stabilization and AC capsular repair in patients with Rockwood type 5 AC joint injury by overreducing the AC joint (intraoperatively decreasing the CC distance to 50% of the unaffected side). With this method, we achieved the final correct anatomic position in both the vertical and the horizontal planes of the AC joint in 95% of our patients (19/20 patients) at the 2-year follow-up, and the functional outcomes (ASES score) were also good. Only 1 patient had loss of reduction alignment; in this patient, vertical displacement of the AC joint on the affected side compared with the unaffected side decreased only from 286% at the initial injury to 202% at the 2-year follow-up, but even so his functional outcomes were good (100/100 in the ASES score evaluation). Our study results thus give strong support to the hypothesis that intraoperatively decreasing the CC distance to 50% of the unaffected side provides good clinical and radiographic outcomes at 2-year follow-up.
Another technique for treating acute AC joint injury of Rockwood type 5 is an anatomic CC ligament reconstruction, for which several studies have reported good functional and radiographic outcomes. 23,24,26,32,33 This technique had better biomechanical testing results when compared with coracoacromial ligament transfer. 9,11,17,22 The surgeon can reconstruct the ligament using either autograft, allograft, or synthetic graft. Overreduction of the CC distance may not be necessary with this technique. The pitfall of this procedure is that it can lead to a clavicular fracture, which can be avoided by maintaining a distance of >20 mm between the 2 bone tunnels.
Postoperative clavicular tunnel widening has been reported in several studies. 16,19,28,34 Jensen et al 15 and Yoo et al 34 reported postoperative clavicular tunnel widening in patients with acute and chronic AC joint injury who had undergone single-tunnel CC stabilization. The investigators found that the clavicular tunnel widths were widened from 4.5 to 11.4 mm 34 and from 6 to 10 mm, 15 respectively. Additionally, Seo et al 28 reported that tunnel widening was related to the CC tunnel angle. In our study, we found the mean widths of the medial and lateral clavicular tunnels to be 5.03 ± 0.68 and 4.47 ± 0.67 mm, respectively, an increase of approximately 100% from the initial clavicular tunnels. Such tunnel widening is usually related to the direction of the sutures, which in our procedure was from the medial border of the coracoid base to the medial clavicular tunnel and from the lateral border of the coracoid base to the lateral clavicular tunnel. During suturing, a tensile load is exerted on the sutures at an angle to their longitudinal axis, with 2 major component forces that influence that tensile load and thus act on the sutures. In a 2-dimensional coordinate system, the primary component forces are parallel and perpendicular. The effect of an applied axial component force might be lower, but the normal component forces could increase stress on the surrounding bone, resulting in tunnel widening and superior displacement of the AC joint.
This study had some limitations. First, as noted earlier, we were unable to control the quality of the radiographic images, and there were possible incongruencies in the images due to variations in beam tilt and patient position; however, we took steps to neutralize this potential problem by using relative value assessments, and we believe our findings are accurate. Second, we evaluated the vertical and horizontal planes based on 2-dimensional anteroposterior view radiographs of both clavicles and a transaxillary view of the affected shoulder, which posed a possible limitation due to the chance of projection error, especially in the transaxillary view. If possible, future studies should be based on 3-dimensional or dynamic 2-dimensional analysis. Other weaknesses of this study were the small number of patients, lack of a control group, use of a single radiographic examiner, unavailability of preoperative ASES scores, and lack of patients with chronic injury. For future studies, we suggest that a larger number of patients be recruited by conducting multicenter trials, that randomized controlled trials be conducted comparing 50% overreduction cases with anatomic reduction cases, and that preoperative and postoperative functional scores be recorded. Finally, to confirm the findings of this study, future studies should be designed to compare an overreduction group with an anatomic reduction group.
Conclusion
In acute AC joint injury of Rockwood type 5, combined CC stabilization and AC capsular repair that intraoperatively decreased the CC distance to 50% of the unaffected side had good functional and radiographic outcomes without any complications.
Footnotes
Acknowledgment
The authors thank Boonsin Trangtrakulwanich and Nannapat Pruphetkaew of the Faculty of Medicine for providing statistical support; Konwarat Ninlachart for the illustrations; and David Patterson of the International Affairs Office of the Faculty for English proofreading.
Final revision submitted September 16, 2020; accepted October 21, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Prince of Songkla University (REC 63-174-11-1).