
Abstract
Background:
Training and game loads are potential risk factors of injury in junior elite ice hockey, but the association of training and game loads to injuries is unknown.
Purpose:
To investigate the association of chronic training and game loads to injury risk in junior male elite ice hockey players.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
In this prospective cohort study, we monitored all health problems among 159 male junior ice hockey players (mean age, 16 years; range, 15-19 years) at sports-specific high schools during the 2018-2019 school year. Players reported their health problems every week using the Oslo Sports Trauma Research Center Overuse Questionnaire on Health Problems (OSTRC-H2). The number of training sessions and games was reported for 33 weeks. We calculated the previous 2-week difference in training/game loads as well as the cumulative training/game loads of the previous 2, 3, 4, and 6 weeks and explored potential associations between training/game loads and injury risk using mixed-effects logistic regression.
Results:
The players reported 133 acute injuries, 75 overuse injuries, and 162 illnesses in total, and an average of 8.8 (SD ±3.9) training sessions and 0.9 (SD ± 1.1) games per week. We found no association between the difference of the two previous weeks or the previous 2- 3- and 4-week cumulative, training or game load and acute injuries, nor the difference of the two previous weeks, or the previous 4- and 6-week cumulative, training or game load and overuse injuries (OR, ∼1.0; P > .05 in all models).
Conclusion:
In the current study of junior elite ice hockey players, there was no evidence of an association between cumulative exposure to training/game loads and injury risk.
Keywords
Ice hockey is a contact sport in which players frequently collide, with each other, boards, or goals, and get hit by sticks and pucks; injuries are prevalent. Injury risk is substantially higher during games (14.73 per 1000 athlete-exposures 45 ; 30.3-49.7 57 and 96.1 58 per 1000 player game hours) than during training sessions (2.52 per 1000 athlete-exposures 45 ; 3.9 per 1000 player practice hours 58 ). The risk of injury increases with age. 57,60 Nordstrøm et al 52 found an average weekly injury prevalence of 20% among junior elite players, split equally between acute and overuse injuries. Injuries have a significant impact on player and team performance. 37
Injury cause is multifactorial and involves both extrinsic and intrinsic risk factors, 47 and recent research has suggested that poor workload management may contribute to injuries and illnesses in sports. 26,28 Across different sports, training and game load have been suggested as risk factors for health problems, 1 and several studies have reported an association between training load and injury. 15,24,29,41,44,48 Studies in rugby, basketball, and Australian football have shown that the greatest incidence of illness and injury is observed when current training loads are greatest. 2,19,20,33 Several studies have found that a large percentage of injuries are associated with rapid changes or spikes in weekly loads 31,34,55 and that competition congestion leads to increased risk of injury. 10,27 Previous studies have also found a relationship between relative change in training load, measured by the acute/chronic workload ratio (ACWR), and injury risk. 34,13,35,36 However, this concept’s methodology has been criticized recently. 38 –40,43
In a small study regarding collegiate ice hockey, Mustapich and Koehle 50 found that players with greater training load experienced greater odds of injury compared with players with lower training loads. The association between training/game load and injury in junior elite ice hockey has not been studied.
The purpose of our study was to investigate the association between chronic training/game load and acute and overuse injuries in junior elite ice hockey players.
Methods
Study Design and Participants
This was a prospective cohort study on junior elite ice hockey players in 5 sports-specific high schools and 2 clubs during the 2018-2019 school year. The data collection methods used are the same as those recently applied in 2 studies in Norwegian ice hockey. 52,53 The prevalence and burden of all health problems are reported in a separate paper. 52
The protocol for this study received ethics committee approval, and all players provided written informed consent to participate in the study. For those younger than 18 years, written consent was signed by their parents. All participants approved access to their data for their school staff and physician.
Recruitment and Inclusion Criteria
We included 6 private specialized sports academy high schools that offer elite sports programs to students who want to combine sports on a high level with a college-entry academic program. The principal investigator (A.N.) contacted the schools, their management, and their coaches by email and telephone in January 2018 and held meetings with all schools providing information about the study during the winter-spring of 2018. The schools had limited medical support: one of the schools had a physician, while the rest had dedicated school staff who contacted medical personnel when needed. We informed the players about the study during a meeting at their school at the start of the school year. One school preferred that the study be conducted through their local affiliated club. We enrolled 2 teams (under 18 years and under 21 years) in the study. In the 5 schools and 1 club included, 3 players declined the invitation to participate in the study, 2 players did not respond in the system after they agreed to participate, and 4 players stopped reporting after 18 weeks. A total of 23 players dropped out throughout the year because of change of school, change of team, or unknown reasons. A female player was excluded from the analyses. A total of 47 players reported trainings and games <50% of all possible weeks and were excluded from the study. The final study sample consisted of 159 players.
Injury and Illness Data Collection
The injury and illness registration and collection procedures have been reported previously. 52,53 Surveillance was conducted using an online platform designed to collect injury and illness data from athletes using the Oslo Sports Trauma Research Center Overuse Questionnaire on Health Problems (OSTRC-H2). 16 –18 The OSTRC-H2 was distributed to players automatically once a week (every Monday) from August 6, 2018, until June 10, 2019, (44 weeks) by SMS and/or email with a direct link to an online injury surveillance platform (AthleteMonitoring.com; FITSTATS Technologies). One school (n = 35) started registration on August 6, 1 school (n = 33) on August 13, 2 schools (n = 80) on September 3, and 2 schools (n = 58) on September 10. If players failed to complete the questionnaire, the system sent an automated reminder every day until a response was received. Additionally, the principal investigator sent SMS reminders to nonresponders after 3 and 5 days. The school physician and staff members could access their players’ health information on a web-based dashboard and encouraged players to respond. To encourage participation, the principal investigator visited 3 of the 6 participating schools during December 2018 and January 2019 and maintained regular contact with all players and responsible staff members throughout the registration period.
OSTRC-H2 Questionnaire
The OSTRC-H2 consists of 4 questions about the athlete’s participation in sports, modification in training or competition, performance, and symptoms of health problems during the past 7 days. 16 –18 If the athlete answered no on the first questions (full participation without problems), the questionnaire was complete for that week. If athletes reported a health problem, they were asked about modification in training or competition, performance, and symptoms and to define whether the health problem was an injury or an illness. In case of an injury, they were asked to classify it as either an acute injury (associated with a specific, clearly identifiable traumatic event) or an overuse injury (no specific identifiable event responsible for the occurrence) and register the affected anatomic area. The players could not specify if their injuries were a result of hockey participation. For all types of health problems, athletes were asked to register the number of days of complete time loss from training and competition (total inability to train or compete) and whether the health problem had been reported previously. They were asked to register all health problems, and in cases of multiple problems the same week, the questionnaire repeated itself.
Definition and Classification of Health Problems
We used an “all complaints” definition, recording all health problems, irrespective of the need for medical attention or the consequences for sports participation. 32,49,59 Our definitions of health problem, acute injury, overuse injury, and illness were consistent with the International Olympic Committee consensus statement. 7 The definition of acute injury was an injury caused by a single, clearly identifiable energy transfer (eg, a fall or collision). The definition of overuse injury was an injury caused by multiple accumulative bouts of energy transfer without a single, clearly identifiable event responsible for the injury. Health problems were defined as “substantial problems” if they caused moderate or severe modifications to training, moderate or severe reductions in performance, or a complete inability to participate in ice hockey. 16 –18
Load Data Collection
Additional questions about the number of training sessions and games played in the previous 7 days were added to the OSTRC-H2 questionnaire on October 29, 2018 (Table 1). The players recorded the number of training sessions in total, training sessions on ice, strength trainings, cardiovascular training, sessions with other type of activity, games, games at the elite level, and shifts on ice at the elite level.
Custom Questions Added to the OSTRC-H2 Questionnaire a

a OSTRC-H2, Oslo Sports Trauma Research Center Overuse Questionnaire on Health Problems.
Prevalence and Incidence Calculations
For each of the 33 weeks, we calculated the following prevalence measures using the methods described by Clarsen et al 17 : all health problems, substantial health problems, all injuries, substantial injuries, all illnesses, and substantial illnesses. We also calculated the average weekly prevalence with 95% confidence intervals. The incidence of each type of health problem was expressed as the number of cases per player per year (52 weeks). The average time loss was expressed as days per athlete per year (52 weeks).
Statistical Methods
All data were compiled using Microsoft Excel software (Microsoft Office 365 ProPlus Version 2002). Data were analyzed using Stata (StataCorp). The mean number of training sessions and games per week were calculated along with their standard deviations. Regarding the training and game load data, 9% and 6%, respectively, were missing; we assumed these to be missing at random. 14 The data were imputed weekly with multiple imputations using linear regression with chained equations. 3 The variables used in the imputation model were age, player position, week, number of training sessions and games in the 2 weeks before imputation, and the latest number of training sessions and games (the variables imputed). After each round of imputation, we calculated the 2-week difference in training/game loads as well as the cumulative training/game loads of the previous 2, 3, 4, and 6 weeks.
We used multivariable logistic regression with random effects (mixed model) to investigate the association between load variables and outcome measures. 51 For acute injuries, we used data from the previous 2-week difference in training/game loads as well as the cumulative loads of the previous 2, 3, and 4 weeks. For overuse injuries, we used data from the previous 2-week difference in training/game loads as well as the cumulative loads of the previous 2, 4, and 6 weeks. The training and game load variables were modeled separately to avoid multicollinearity. A random intercept was included to account for within-player correlations. Age, player position, week, and training sessions and games in the current week were potential confounding factors adjusted for. Week was modeled with a second-degree polynomial term to account for potential nonlinearity. 4 In addition, to account for the exposure in the current week, 63 training sessions and games in the current week were adjusted for. Models were run on each of 100 imputed data sets, and results were pooled with Ruben’s rules. Statistical significance was defined as P <.05.
Results
Response Rate to the Weekly Questionnaires
We distributed 5223 questionnaires and received 4870 responses (average weekly response rate, 93%; range, 86%-99%) during the 33-week study period.
Number and Incidence of Health Problems
The players reported 133 acute injuries, 75 overuse injuries, and 162 illnesses in total. This translated to 1.4 new acute injuries, 0.8 new overuse injuries, and 1.7 new illnesses per athlete per year (Table 2). The average time loss was 34 days (95% CI, 33-35 days) per athlete per year, 17 days (95% CI, 16-19 days) for acute injuries, 8 days (95% CI, 7-10 days) for overuse injuries, and 9 days (95% CI, 7-10 days) for illnesses.
Number of Cases, Incidence, and Total Time Loss of Acute Injuries, Overuse Injuries, and Illnesses

a Incidence is shown with 95% CI.
Prevalence of Health Problems
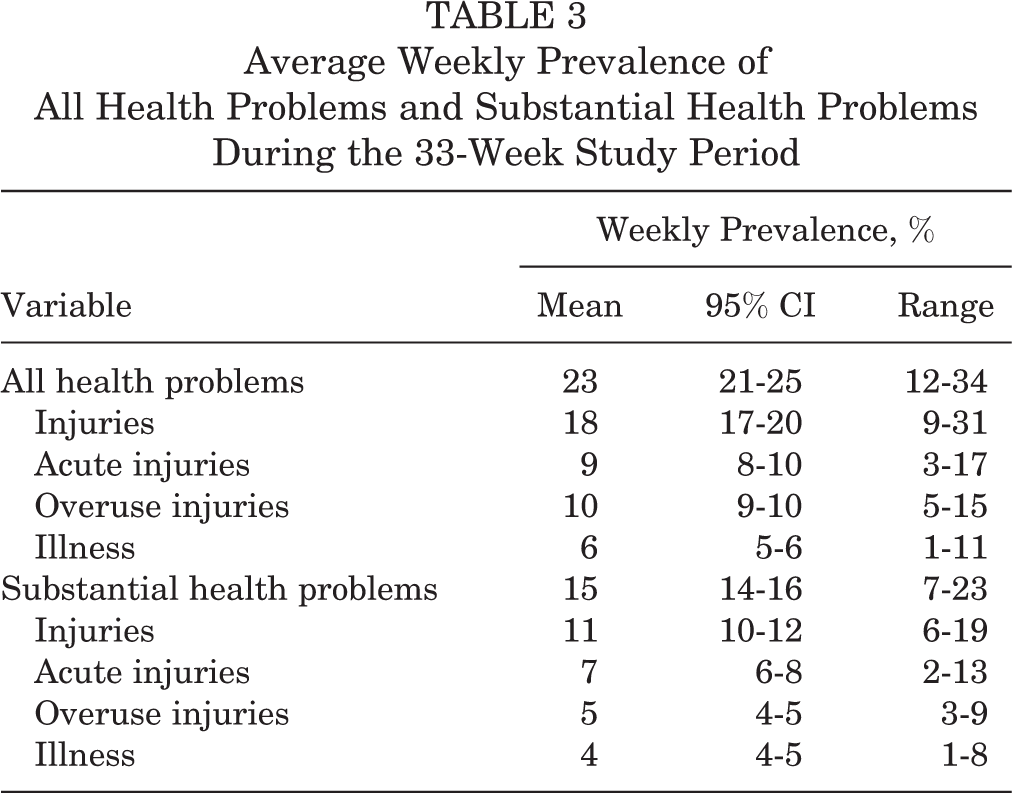
The average weekly prevalence of health problems, with 95% confidence intervals and ranges, is shown in Table 3.
Average Weekly Prevalence of All Health Problems and Substantial Health Problems During the 33-Week Study Period
Training and Game Load
The players reported an average of 8.8 (SD ±3.9) training sessions and 0.9 (SD ± 1.1) games per week (Table 4). The weekly average number of training sessions fell slightly throughout the registration period, and there were 2 periods with fewer training sessions: over a school holiday (registration weeks 9 and 10) and at the end of the hockey season (registration weeks 24-28). The weekly average number of games played was quite constant throughout the registration period but had 2 periods with fewer games: over a school holiday (registration weeks 8-10) and at the end of the hockey season (registration weeks 24-26). No games were played during weeks 27 to 33 of the registration. The number of training sessions and games by player position and age is shown in Table 4.
Training Sessions and Games by Player Position and Age a
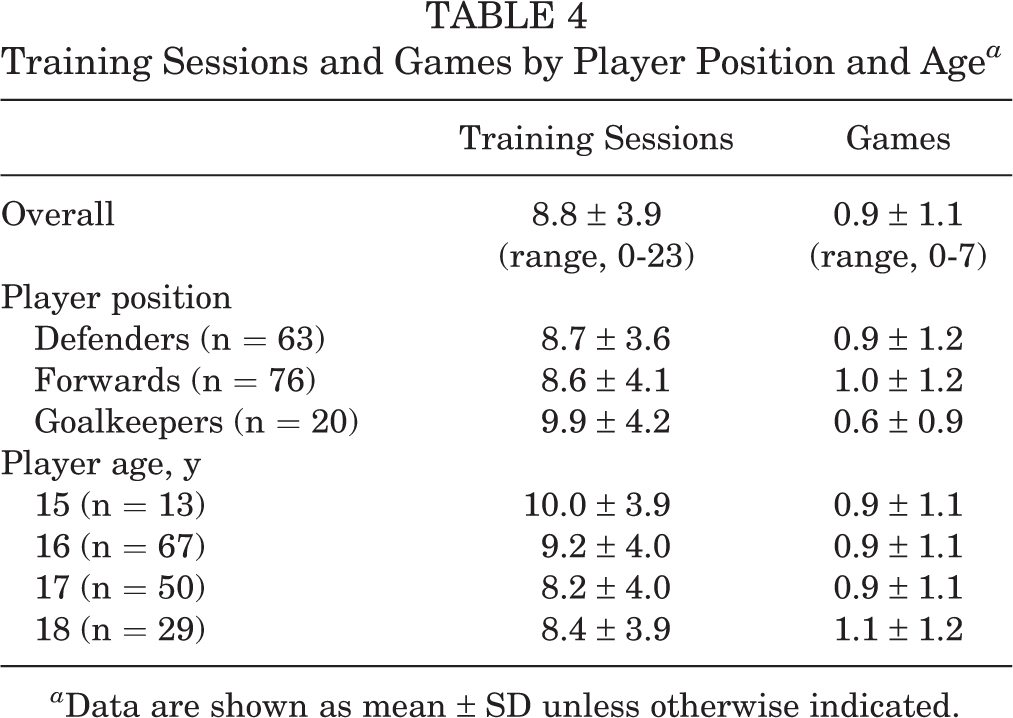
a Data are shown as mean ± SD unless otherwise indicated.
Association of Training Sessions and Games to Injuries
Table 5 shows the association between training/game loads and acute or overuse injuries, adjusted for player position, age, week, second-degree polynomial term of the week, and number of training sessions or games in the current week. The relationship between cumulative number of training/game loads and acute or overuse injuries had low effect sizes and was not significant (OR, ∼1.0; P > .05 in all models) (Table 5). The covariates of player position, age, week, second-degree polynomial term of week, and number of training sessions/games in the current week demonstrated consistent results throughout all the models, for both acute injuries and overuse injuries (Supplemental Table S1). None of the participant characteristics (player position, age) were significantly related to injury risk. Time was significant, as well as the nonlinear term for time (week). Training and game sessions for the current week had low odds ratios and significant P values. The random effects were significant in all models (P < .05) (Supplemental Table S1). Analyses of substantial acute and overuse injuries showed essentially the same results as analyses of all acute and overuse injuries (Table 5 and Supplemental Table S2).
Model Results From Number of Training Sessions/Games and All Injuries and Substantial Injuries a
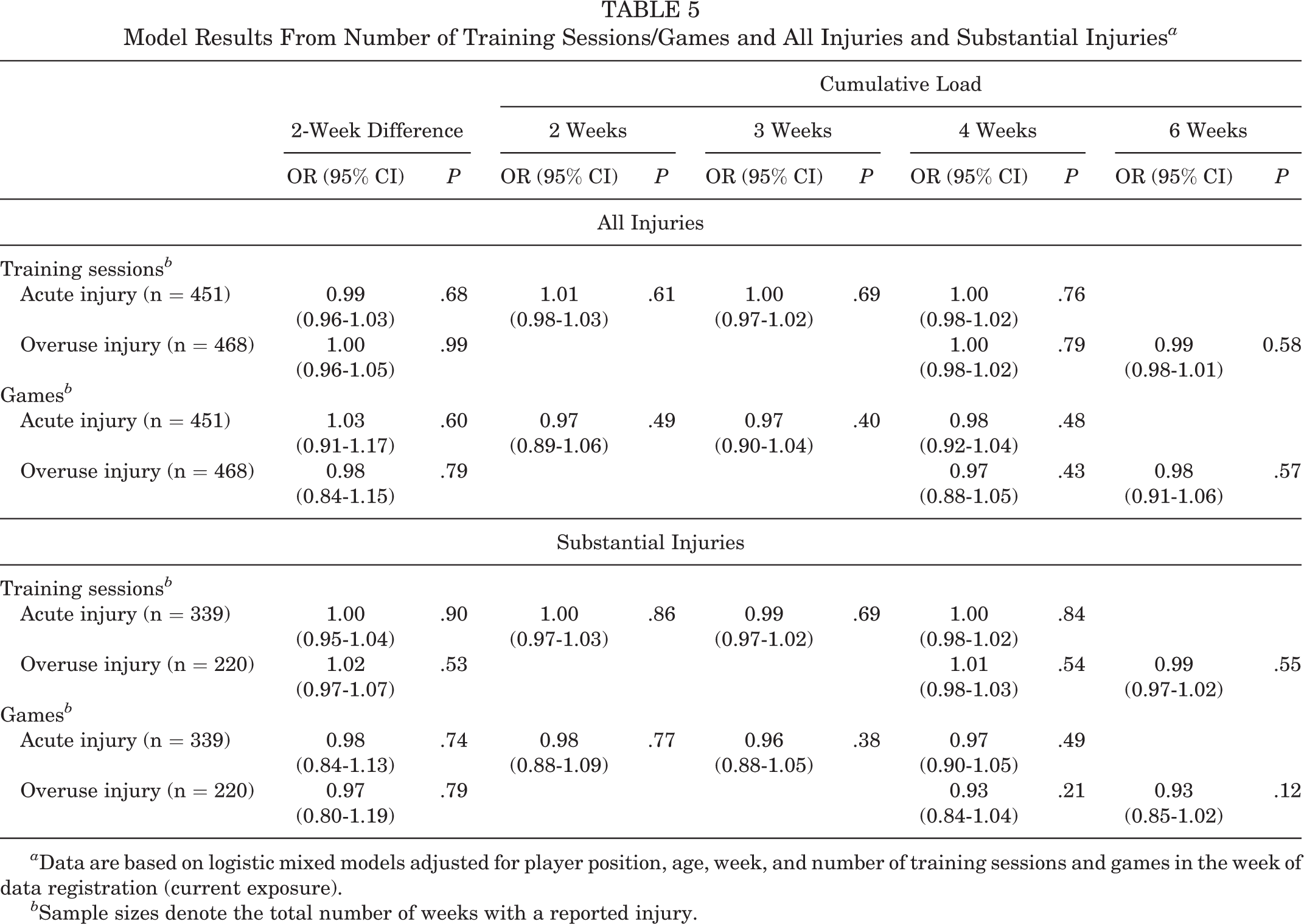
a Data are based on logistic mixed models adjusted for player position, age, week, and number of training sessions and games in the week of data registration (current exposure).
b Sample sizes denote the total number of weeks with a reported injury.
Discussion
This study is the first to investigate the association between number of training sessions/games and injuries in junior elite ice hockey players. We found no association between the cumulative long-term or 2-week difference in the number of training sessions or games and the risk of acute or overuse injuries.
Developing youth athletes are at increased risk of injury when introduced to new loads, changes in loads, or congested competition calendars. 11,15,25,30 The most talented athletes might be more prone to injury, 6 and load volume 54,61 and impact load 54,62 are believed to represent important risk factors for injury. To our knowledge, there is no previous study in junior ice hockey reporting on training and game load. The players reported an average of 8.8 training sessions and 0.9 games per week, reflecting their status as elite junior players. This training volume is similar to that of elite youth handball. 12 Other studies have reported on the training load in football, 15,22 but differences in quantifying workload make direct comparisons to our findings difficult.
The ACWR has recently been criticized because of methodological issues, and the validity of the model has been questioned. 38 –40 Methodological choice affects the potential association between ACWR and health problems 21 ; however, the causal relation to injury has not been established. 40 The proposed relationship between ACWR and health problems is based on descriptive studies reporting associations between various alterations of ACWR and health problems. Several studies have examined the relationship between training load and health problems in junior sports. 5,15,22,23,42,48,56 Most of these have used the ACWR, but none have used the same calculation of ACWR, analytical approach, or statistical methods. Despite these limitations, studies in football 15,23 and other sports 42,48 have found that variations in the ACWR were associated with the risk of health problems. In contrast, 1 study based on the ACWR found that internal load markers were not associated with noncontact injuries in young football players. 56 The only randomized trial performed (482 elite youth soccer players of both sexes) using the ACWR to manage player load within what was believed to represent the “safe zone” found no between-group difference in health problem prevalence, suggesting that the specific load management intervention was not successful in preventing health problems. 22
Because of the recent criticism of the ACWR concept, we chose not to use ACWR for our analyses. A priori, we decided to use measures likely to be most valid and clinically relevant. It is not known how many weeks back in time training and game load can have an impact on injury, and this may differ between sports. Our data only included the total number of training sessions and games; we do not have information about their intensity or duration. It was not possible to investigate current exposure without bias as we only recorded load once a week and did not register exactly when during the week an injury occurred. However, this is not the case for previous cumulative exposure. Direct comparison of studies using ACWR as load measures to our findings is therefore difficult.
In a small study in collegiate ice hockey (1 team, 26 players), Mustapich and Koehle 50 found that players with greater 2-day training load experienced greater odds of injury compared with athletes with lower loads. This study defined injury as that related to ice hockey play, resulting in time loss or modification of a training session or game, diagnosed by the team physician or physical therapist. The subjective training load for all on-ice sessions was recorded using the subjective rating of perceived exertion (modified Borg CR-10 RPE). Each athlete’s score was multiplied with the duration in training or game sessions in minutes, determining the session training load value in arbitrary units. They used cumulative training load (each day, 2 days, and 2 weeks) measured in arbitrary units. Cumulative training load over 2 weeks affected the odds of injury occurrence positively, but this finding was not significant. These findings are not in line with ours, although direct comparisons are difficult, as we separated training from game load, and acute from overuse injuries, and only recorded the number of training sessions and games.
We found no association between the number of training sessions/games and injuries. An explanation for this may be that the relationship between training load and health problems is complex, and several other factors might influence the occurrence of health problems: previous injury status, fitness, wellness, nonsporting load, biomechanics, poor technique, differences in reporting of injuries, differences in pain threshold and pain tolerance, or simply chance. 8 Meeuwisse 46 and Meeuwisse et al 47 have previously demonstrated how internal and external risk factors can influence injury risk. Later, Bahr and Holme 8 and Bahr and Krosshaug 9 expanded this conceptual model and considered how injury mechanisms—the inciting event—also may play a crucial role. Further, cumulative long-term exposure might have a small-to-moderate association to injury, and our sample size might not have been large enough to detect small-to-moderate associations. 8
Despite conflicting evidence, training load is considered to be an important risk factor for health problems. Previous research has suggested that the relationship between training load and injury risk should be assumed to be nonlinear. 4 However, future research on the methods that are most optimal to determine the relationship between training load and risk of injury is needed.
Methodological Considerations
One of the main strengths of the study is the high response rate and a relatively large sample size. We also used sensitive injury surveillance methods to capture all health problems and a multivariable statistical approach to investigate training and game load as potential risk factors for injury.
This study also has several limitations. The data were collected from the players, and the extent to which health problems and numbers of trainings sessions and games were underreported could not be measured. The weekly reports by the athletes are subjective, and the reporting threshold may differ between players. Recall bias and underreporting of health problems and training sessions and games could also affect the results; daily reports could reduce this bias but, on the other hand, challenge the compliance of the participants.
The players reported the number of training sessions in total, training sessions on ice, strength trainings, cardio trainings, sessions with other types of activity, games, and games and shifts on ice at the elite level. In our analyses, we only used the total number of training sessions and games; we did not ask for information about their intensity or duration. However, the duration of a training session was very consistent, since access to time on ice was limited; typically, 60 to 75 minutes was allotted to each team for each session. Strength sessions typically lasted 45 to 60 minutes. We would argue that the number of training sessions is an adequate marker for training load; adding duration in minutes would have minimal impact on the outcome.
Still, the intensity of training sessions and games may vary substantially, even between players in the same session. We therefore would have liked to have had data on both external (eg, GPS data) and internal (eg, session rating of perceived exertion) loads. This has been done in other sports, and we recommend this for future studies on training and game load in ice hockey.
While this study included 159 players monitored for 33 weeks, resulting in nearly 5000 observations, sample size is still a limitation and may not be sufficient to detect small-to-moderate associations between training/game load and injury. Nevertheless, across all models, the odds ratio is centered around 1, with narrow confidence intervals. This consistent finding indicates that the risk of a type 2 error is low and that adding more observations is unlikely to change our conclusions.
Health-related problems are expected in ice hockey. The wide definition used, based on all health complaints, leads to the registration of minor and transient problems (eg, muscle soreness or unspecific symptoms). 17 This is a source of systematic bias, overestimating the prevalence of sports-related health problems. The “substantial health problem” definition (problems leading to reduced performance and/or participation) might be a more appropriate estimate of the impact of injuries and illnesses in ice hockey.
Finally, our study only included male junior elite ice hockey players and may not be generalizable to other populations.
Conclusion
In the current study of junior elite ice hockey players, there was no evidence of an association between cumulative exposure to training or game loads and injury risk.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671221129646#supplementary-materials.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221129646 - Association of Training and Game Loads to Injury Risk in Junior Male Elite Ice Hockey Players: A Prospective Cohort Study
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221129646 for Association of Training and Game Loads to Injury Risk in Junior Male Elite Ice Hockey Players: A Prospective Cohort Study by Anine Nordstrøm, Roald Bahr, Lena K. Bache-Mathiesen, Ben Clarsen and Ove Talsnes in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank all the athletes for their participation, as well as the schools, clubs, and medical teams involved. They thank the Innlandet Hospital Trust and Stiftelsen fondet til fremme av idrettsmedisin og idrettsfysioterapi for financial support. They also thank Lien My Diep and Harald Weedon-Fekjær for excellent help with multiple imputation. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Health Authority, the International Olympic Committee, the Norwegian Olympic and Paralympic Committee and Confederation of Sports, Norsk Tipping, and Sparebankstiftelsen DnB.
Final revision submitted June 13, 2022; accepted July 24, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support was received from the Innlandet Hospital Trust (salary support for A.N.) and the Stiftelsen fondet til fremme av idrettsmedisin og idrettsfysioterapi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Norwegian Centre for Research Data (reference No. 59423 LH/LR) and the Norwegian Data Inspectorate (reference No. 17/00803-6/CGN).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.