
Abstract
Background:
Little is known about the association between physical fitness and the risk of injury or illness in ice hockey. The least-fit players may be more prone to injury and illness.
Purpose:
To examine the association between preseason fitness level and injury or illness risk among elite ice hockey players during the regular season.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 133 male ice hockey players in the GET League (the premier professional league in Norway) completed 8 different exercises (40-m sprint, countermovement jump, 3000-m run, squat, bench press, chin-ups, brutal bench, and box jump) at the annual 1-day preseason testing combine. During the 2017-2018 competitive season, the players reported all health problems (acute injuries, overuse injuries, and illnesses) weekly (31 weeks) using the Oslo Sports Trauma Research Center Questionnaire on Health Problems.
Results:
Overall, the players reported 191 acute injuries, 82 overuse injuries, and 132 illnesses. The least-fit tercile of players did not report more health problems (mean, 3.0; 95% CI, 2.2-3.8) compared with the most-fit (mean, 3.4; 95% CI, 2.6-4.2) or the medium-fit (mean, 2.7; 95% CI, 1.9-3.5) players. The most-fit players reported more substantial health problems (mean, 2.0; 95% CI, 1.6-2.5) compared with the medium-fit (mean, 1.3; 95% CI, 0.8 -1.8) and least-fit (mean, 1.8; 95% CI, 1.3-2.3) (P = .02) players. There was no association between low physical fitness and number of health problems when comparing the least-fit tercile of the players with the rest of the cohort (P > .05); however, there was an association between low physical fitness and greater severity of all health problems when comparing the least-fit tercile of players to the rest of the cohort after adjusting for time on ice per game, playing position, and age (P = .02).
Conclusion:
Low physical fitness was not associated with increased rate of injury or illness but was associated with greater severity of all health problems after adjusting for time on ice per game, playing position, and age.
Keywords
Ice hockey is an intermittent sport where periods of high-intensity play are interspersed with passive recovery periods. This high-speed sport combines technical skills with explosive ability and high aerobic and anaerobic work capacity. The divide between what is required to maintain and improve athletic skills versus minimize injury and illness risk is not fully understood. Previous studies on elite adult athletes have suggested that rapid increases in training load might lead to injuries, 37,38 and high training loads and well-developed physical qualities are thought to be associated with a lower risk of injury; thus, less fit players may be more prone to injury. 16 However, previous research 8,22 –25 on the association between training load and injury has been criticized recently because of methodological limitations.
Whether it is possible to use screening tests to identify who is at risk for a sports injury has been questioned. 2,28 Several studies 3,9,27,36,47 have found limited evidence using functional movement screening tests to assess injury risk in different sports. In football, preseason physical tests to screen for risk factors for injury are commonly used, and better preseason aerobic fitness has been associated with lower injury risk. 10,46 Still, several studies 1,34,39 have not found any correlation between the results of preseason physical performance tests and the risk of injury the following season. However, in rugby and Australian football, studies 17,18,35 have observed an inverse relationship between physical fitness and injury risk.
Little is known about the association between physical fitness and injuries and illnesses in general in elite ice hockey, although low levels of off-season sport-specific training and previous injury have been suggested to represent risk factors for groin injury. 11 Also, low hip adduction-to-abduction strength ratio during the preseason has been associated with adductor muscle strains, 44 and strengthening the adductor muscle group appears to be effective in preventing adductor strains among professional ice hockey players. 43 However, Grant et al 19 suggested that aerobic fitness and maximum strength outcomes were not associated with on-ice injury risk in male collegiate hockey players, after controlling for player position and body composition.
In this study, we aimed to determine whether the least-fit players in the Norwegian men’s premier professional league (GET League) were at greater risk of injury and illness. The least-fit players may be more prone to injury and illness when exposed to high training loads and congested match schedules. We used a battery of physical fitness tests to identify the least-fit tercile of players preseason and investigated whether these players were more prone to injury and illness than were more-fit players during the subsequent ice hockey season.
Methods
Study Design and Participants
This was a prospective cohort study of male ice hockey players in the GET League during the 2017-2018 season. A total of 225 players (mean age, 24 years; range, 17-41 years) registered all health problems once a week using a smartphone application. Details on the prevalence and burden of all health problems were reported in a separate paper. 32 Of the 225 players, 164 attended the annual 1-day, preseason testing combine.
The study was approved by the Norwegian Data Inspectorate and the South-Eastern Norway Regional Committee for Research Ethics. All athletes provided written informed consent to participate.
Recruitment and Inclusion Criteria
The GET League consists of 10 teams, each consisting of 22 to 25 players. Most teams have medical support personnel, including a physician; physical therapist; and for some teams, other health professionals. The principal investigator contacted all teams, their management, and medical teams via email and telephone before the season with information about the study. We informed the players about the study during the combine, which all teams attended. We included 9 teams. 32 One team did not have a medical team and could not follow up on data collection during the season, and it was not included. In the 9 teams participating, 5 players declined to participate in the study, 6 did not download the necessary smartphone application, and 1 dropped out after reporting for 8 weeks.
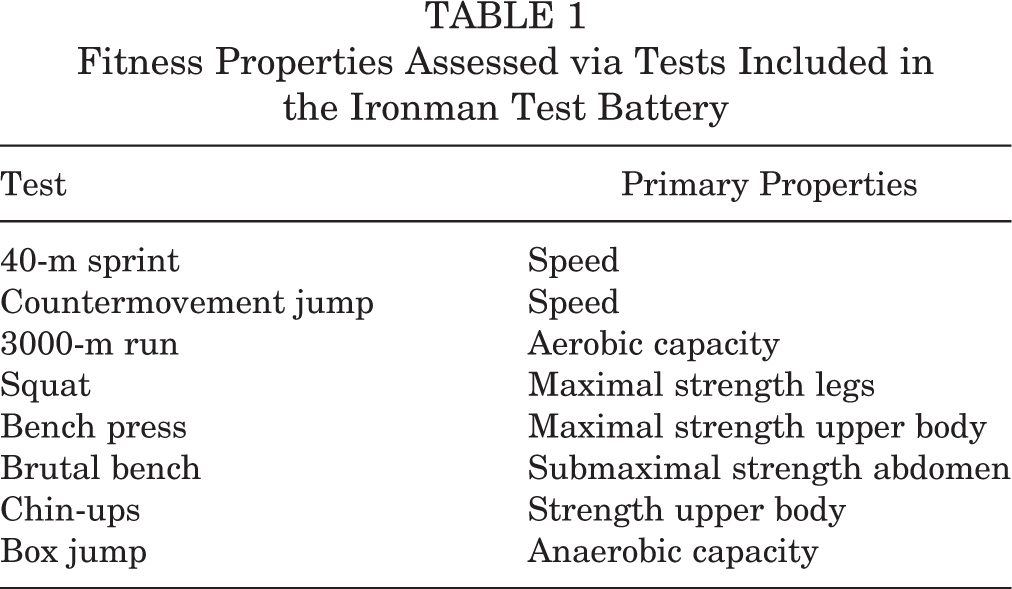
During the combine, players completed 8 different exercises (Table 1). A total of 133 players (mean age, 23 years; range, 17-33 years) completed ≥5 exercises during the testing and were included in the study. The sample included 76 forwards, 44 defenders, and 13 goalkeepers.
Fitness Properties Assessed via Tests Included in the Ironman Test Battery
Preseason Fitness Testing
Since 2002, the Norwegian World Cup alpine skiing team has used a set of standardized fitness tests (Ironman Test battery; Attacking Vikings, developed by Norwegian World Cup alpine skiing team, Version 5.0, August 14, 2014) to evaluate and promote the general physical fitness needed to compete at an elite level. Multiple other sports have since used the same tests to evaluate aerobic and anaerobic capacity, strength, agility/coordination, and speed. The Norwegian Ice Hockey Association has used a modification of these fitness tests to evaluate the general physical fitness level among ice hockey players in the GET League annually. Before the 2017-2018 season, players completed 8 different exercises, including a 40-m sprint (n = 127), countermovement jump (n = 131), 3000-m run (n = 114), squat (n = 116), bench press (n = 120), “brutal bench” (n = 123), chin-ups (n = 114), and box jump (n = 111). All players except those limited by injury performed all tests; players performed as many tests as possible. For each test, we ranked the players from most fit (1) to least fit (111-131, depending on the number of players tested) based on performance. By summing these ranks, we identified the tercile of the players with the greatest average total score (ie, the least-fit tercile of players) among players completing ≥5 tests. For each player, we calculated the average ranking score for speed (40-m sprint and countermovement jump), strength (squat, bench press, brutal bench, and chin-ups), endurance (3000-m run), and anaerobic capacity (repeated box jump). We then identified the tercile of the players with the greatest total score within each of these dimensions of physical performance.
Ironman Test Battery
The tests were performed at Olympiatoppen (The Norwegian Olympic Training Center) in Oslo, Norway, on August 5, 2017. The specific tests were performed in a standardized order (Table 1) and monitored by technical staff at Olympiatoppen.
40-m Sprint
The players were requested to run 40 m as fast as possible. The test started when the rear leg passed a photocell located 50 cm in front of the starting line. Every player had 3 attempts. The fastest time in seconds was retained for analyses.
Countermovement Jump
The players were requested to perform 1 jump as high as possible. The players started from a standing position with extended knees and arms placed at their hips (Figure 1A). The test was performed as a fast bend in the knees until the angle was about 90° and then a jump straight upward. Every player had 3 attempts. The highest jump was noted.

(A) Countermovement jump. Fast bend in the knees until the angle was about 90° and then a jump straight upward; 1 jump as high as possible. (B) Brutal bench. Valid repetitions required elbows to be in contact with the knees at every lift and the buttocks to be in contact with the surface at all time. (C) Chin-ups. Pronated grip with the chin elevated above the rod in every lift and the arms fully extended between every repetition. (D) Box jump. Side-to-side jumps within 90 seconds. Every landing on the bench counted as a jump.
3000-m Run
The players ran 3000 m as fast as possible on an outdoor 400-m running track. Time was measured using a stopwatch.
Squat
The players were requested to perform 1 squat with maximum load. The players started from a standing position with extended knees. When performing the squat, the hip crease had to be lower than the highest point of the knee. Every player had 3 attempts. The maximum weight that the player could lift using correct technique was recorded.
Bench Press
Players were requested to perform 1 bench press with maximum load. The players were allowed a maximum of 81 cm between their little fingers while holding the barbell and started from a position with extended arms. Correct performance included slowly lowering the barbell to the chest and then lifting to extended arms as 1 movement. The buttocks had to be in contact with the surface at all time. Every player had 3 attempts. The maximum weight that the player could lift using correct technique was recorded.
Brutal Bench
The players started hanging upside down with knees flexed in a 90° position with hands held behind the head, holding a 5-cm ring made of rope (Figure 1B). All movements had to be slow and controlled. Elbows had to be in contact with the knees at every lift, and the buttocks had to be in contact with the surface at all times. There was no time limit, but the athlete received a warning if a pause between the repetitions extended 1 second. The next pause between repetitions stopped the test. The number of correctly performed crunches was noted.
Chin-ups
The players started with extended arms and pronated hands around the pole 10 cm wider than the width of their shoulders (Figure 1C). All movements had to be slow and controlled. The chin had to be above the pole, and the arms had to be fully extended between every lift. There was no time limit, but the maximum allowed pause between each chin-up was 2 seconds. The number of chin-ups performed correctly was recorded.
Box Jump
The players were requested to perform the maximum number of jumps possible within 90 seconds. The bench was 40 cm high, 51 cm wide, and minimum 60 cm long. The players started at the top of the bench, jumped laterally to one side of the bench with their feet together, then back up on the bench and laterally to the other side (Figure 1D). The test started when the player jumped down to one side. Every landing on the bench counted as a jump. The number of lateral jumps the player could perform in 90 seconds was recorded.
Injury and Illness Data Collection
Details on the injury and illness registration and the data collection procedures have been reported previously. 32 Injury and illness data were collected using the Oslo Sports Trauma Research Centre Questionnaire on Health Problems (OSTRC-H). 6,7 All players were required to download a mobile application (SpartaNova), which distributed the OSTRC-H automatically once a week (every Sunday) between September 17, 2017 and April 15, 2018 (31 weeks). The OSTRC-H consists of 4 key questions about the athlete’s participation in sports, training volume, performance, and symptoms of health problems during the previous 7 days. 6,7 The response to each of the 4 questions was allocated a numeric value between 0 and 25. The value 0 represented no problems, and the value 25 represented the maximum level for each question. The numeric values were summed to calculate a weekly severity score from 0 to 100 for each health problem. If the athlete answered the minimum score for each of the 4 questions (full participation without problems, no reduction in training or performance, and no symptoms), the questionnaire was completed for that week. If athletes reported a health problem, they were asked to define whether it was an illness or an injury. In case of an injury, they were asked to classify whether it was an acute (associated with a specific, clearly identifiable traumatic event) or an overuse (no specific identifiable event responsible for the occurrence) injury and register the affected anatomical area. In case of an illness, they were asked to report their main symptoms (by choosing from multiple predefined symptoms). For all types of health problems, athletes were asked to register the number of days of complete time loss from training and competition (total inability to train or compete) and whether the health problem had been reported previously. They were asked to register all health problems, and, in cases of multiple problems the same week, the questionnaire repeated itself.
Definition and Classification of Health Problems
We used an “all complaints” definition, recording all health problems irrespective of the need for medical attention or the consequences on sports participation. 15,30,41 Health problems were classified as an injury if they affected the musculoskeletal system or were a concussion or as an illness if they affected an organ system or represented generalized symptoms. The definition of an acute injury was an injury or trauma with rapid onset associated with a clearly identifiable event. The definition of an overuse injury was an injury without a single, identifiable event. 15 Health problems were defined as substantial problems if they caused moderate or severe reductions in training volume, moderate or severe reductions in performance, or a complete inability to participate in ice hockey. 6,7
Match Exposure
Individual time on ice per game was calculated based on official match records from the Norwegian Ice Hockey Association database (https://www.hockey.no/). 33
Outcome Variables
The number of all and substantial health problems, acute and overuse injuries, and illnesses was calculated for every athlete. The cumulative severity score of injuries and illnesses was calculated by summing the score for every week a health problem was reported. 32
Statistical Methods
Data were analyzed using STATA (StataCorp 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). The number of all and substantial health problems, acute and overuse injuries, and illnesses was estimated as the mean with 95% CIs. Comparisons of means were based on the Kruskal-Wallis test. The cumulative severity scores for all and substantial health problems, acute and overuse injuries, and illnesses were reported as the median because of data skewness. We used linear or median regression models, both crude and adjusted, to investigate the differences in outcome measures between the least-fit tercile and the rest of the cohort based on the mean ranking score on fitness tests. Time on ice (per game), player position, and age (3 groups: 17-20 years [n = 44], 21-25 years [n = 48], and 26-33 years [n = 39]) were potential confounding factors and used as covariates in the adjusted models. Statistical significance was defined as a P value <.05.
Results
Ironman Test Results
Table 2 shows the results from the fitness testing, as well as the test results and ranking by player position. Goalkeepers were less fit overall than defenders and forwards. The test results did not differ significantly among defenders, forwards, and goalkeepers, except for the 40-m sprint and bench-press tests, where defenders and forwards performed significantly better than goalkeepers.
The mean overall fitness ranking did not differ significantly among age groups (17-20 years: mean, 74.2 [95% CI, 68.2-80.1]; 21-25 years: mean, 65.5 [95% CI, 58.4-72.5]; and 26-31 years: mean, 62.8 [95% CI, 56.4-69.1]; P = .052). However, older players (26-31 years) performed better in the 3000-m run (P = .03), brutal bench (P = .0495), and bench press (P = .01) tests than younger players (17-20 years).
Ironman Test Results and Overall Ranking by Player Position a

a Bolded P values indicate statistically significant difference among positions (P < .05, Kruskal-Wallis test).
Health Problems
The players reported 191 acute injuries, 82 overuse injuries, and 132 illnesses during the 31 weeks of registration. The average number of health problems per player and fitness group are shown in Table 3. The number of health problems did not differ among fitness level groups, except for all substantial health problems (P = .02).
Number of All and Substantial Health Problems, Total and by Fitness Ranking Group a

a Data are shown as mean (95% CI). Bolded P value indicates statistically significant difference among fitness levels (P < .05, Kruskal-Wallis test).
Table 4 shows the number of all health problems and substantial health problems by player position. Goalkeepers reported fewer acute injuries than did defenders and forwards (P = .002) and fewer substantial acute injures than did forwards (P = .01). Players aged 21 to 25 and 26 to 33 years reported more substantial acute injuries than did players aged 17 to 20 years (P = .014).
Number of All and Substantial Health Problems by Player Position a

a Data are shown as mean (95% CI). Bolded P values indicate statistically significant difference among fitness levels (P < .05, Kruskal-Wallis test).
The number of health problems did not differ significantly among groups for each of the main fitness properties (strength, speed, or aerobic and anaerobic capacity) (Appendix Table A1).
The median cumulative severity score for all and substantial health problems did not differ among fitness level groups or age groups or by player position, except for goalkeepers reporting a greater cumulative severity score compared with defenders and forwards (P = .04). The median cumulative severity score did not differ significantly among groups for any of the main fitness properties (strength, speed, or aerobic and anaerobic capacity).
Association Between Physical Fitness Level and Health Problems
Table 5 shows the number and burden of health problems comparing the least-fit athletes with the rest of the cohort, adjusting for time on ice, player position, and age. There was no difference in the mean number of health problems between the least-fit players and the rest of the cohort. The least-fit players reported greater median cumulative severity score for all health problems (P = .02) when adjusting for time on ice (per game), player position, and age.
Association Between Injury or Illness (Number and Cumulative Severity Score of Health Problems) Comparing the Least-fit Athletes (Greatest Tercile According to Composite Score) with the Rest of the Cohort a

a Data are based on univariate and multiple linear regression analyses and univariate and multiple median regression analyses, adjusted for time on ice, player position, and age. Bolded P value indicates statistical significance (P < .05).
Discussion
This is the first study to evaluate the association between preseason fitness level and health problems during the subsequent season in ice hockey. We used a set of standardized fitness tests related to strength, speed, and aerobic and anaerobic capacity to identify the least-fit tercile of players in the cohort. Overall, the least-fit tercile of players did not have a greater risk of injury or illness compared with the rest of the cohort, although they reported a greater total burden of health problems when adjusting for time on ice per game, player position, and age.
We found that forwards reported a significantly greater number of acute injuries and substantial acute injuries than did goalkeepers. Our cohort included only 13 goalkeepers, which limited statistical power; nevertheless, several previous studies have demonstrated similar results. 13,19,26,42
In ice hockey, previous studies on the association between preseason fitness and injury and illness are few and limited. In a cohort study of 79 male collegiate players over 8 consecutive seasons, aerobic fitness and maximum strength were not strongly predictive of on-ice injury. 19 The findings of that study are comparable with ours, but dissimilarities in level of play, fitness tests, and statistical analyses prevent a direct comparison of results. In soccer, some studies have demonstrated results in line with ours. A prospective cohort study of male soccer players (n = 320) from the 2 highest divisions in Iceland did not demonstrate any relationship between physical fitness qualities and injury. 1 In 2 prospective cohort studies in Sweden, the results of preseason fitness testing were not associated with risk of injury among female senior (n = 123) or male elite soccer players (n = 63). 34,39 Two studies of youth (n = 67) and adolescent (21 teams) soccer players found no association between preseason functional tests and injuries. 12,14 Moseid et al 29 found no association between low physical fitness and the number or severity of injury and illness in a mixed-sports sample of youth elite athletes (n = 166) from Sports Academy High Schools. A prospective study on male elite junior Australian rules football players (n = 382) found an association between physical fitness tests and risk of injury, 5 but these findings were not reproduced. 4
However, some studies have demonstrated results conflicting with ours. In soccer, preseason aerobic fitness has been associated with lower risk of injury among collegiate male and female (n = 43) and professional (n = 31) players, 10,46 and lower risk of injury and illness among adolescent female players (n = 54). 45 In rugby, aerobic and anaerobic performance, the number of push-ups (n = 258), and slower 10- and 40-m sprint speed (n = 153) have been found to be risk factors for injury among male players. 17,35 A prospective cohort study of elite Australian rules football players (n = 69) over 4 seasons found that lower aerobic-running fitness was associated with increased risk of injury. 18 In youth alpine skiing, poor core and reactive leg strength have been associated with injury risk and injury severity. 31
Some of the studies mentioned have findings comparable with ours, but different participant profiles, fitness tests, and statistical analyses prevent a direct comparison between studies. The lack of an association between fitness test results and injury or illness in our study could have different explanations. The most obvious is that preseason fitness level does not represent a risk factor for injury or illness. Another could be the test battery we used. The tests were performed off ice, and the fitness tests included in the battery might not be sufficiently specific to detect relevant risk factors for injury or illness. Ice hockey is an intermittent high-speed sport that combines technical skills with key physical components: explosive ability and high aerobic and anaerobic work capacity. While the test battery used may represent valid indicators of on-ice performance, the relevance of the current tests in relation to injury risk may be questioned. Moreover, players in a specific playing position typically share a certain set of anthropometric and physical performance characteristics. Thus, if the relationship between fitness and injury is to be studied further, fitness tests specific to the demands of playing on ice and certain positions may need to be developed. Aerobic capacity measured via a continuous 3000-m run lasting >10 minutes may not be a relevant test for ice hockey players, who during games have 40-second to 60-second shifts on ice with several minutes of rest in between, while the 90-second box jump test has obvious validity for performance. Another limitation is that players were only tested once in the preseason, and their fitness may have changed during the season, for better or worse.
Preseason physical testing is conducted by coaches and designed primarily to measure physical standards necessary for elite ice hockey performance. To use such tests as injury predictors, researchers should design a test battery to evaluate more specific and relevant physical tests aimed at the most common injuries in ice hockey.
Methodological Considerations
Several preseason physical fitness tests to screen for risk factors for injury exist, but there is limited and conflicting evidence regarding their measurement properties. 20,21,40 The Norwegian Ice Hockey Association has used a modification of the standardized fitness tests of the Norwegian World Cup alpine team to evaluate the general physical fitness level among ice hockey players in the GET League on their annual 1-day, preseason testing combine. We chose to use these tests in our study, as all teams participate. Using different tests may have changed our results.
Tests procedures were standardized before testing. Testing was monitored by personnel from Olympiatoppen. Nevertheless, the test-retest reliability is unknown. Since we wanted to evaluate general physical fitness, we ranked players based on performance on each test and used a composite score based on the sum of each player’s ranking. A limitation to this approach is that all tests are equally weighted. However, their relevance may differ related to performance and injury risk.
We adjusted only for time on ice per game, player position, and age and not multiple comparisons in our analyses. Other factors, like comorbidity profile and environmental/social risk factors, might play a role in the athletes’ risk of illness, and we have not adjusted for them. Interpretations of statistical results should be made with full knowledge of spurious findings. Our study included only male senior elite players, and the findings may not be generalizable to other populations.
Conclusion
We used a set of standardized fitness tests related to strength, speed, and aerobic and anaerobic capacity to identify the least-fit tercile senior elite ice hockey players. Low physical fitness was not associated with increased rate of injury or illness but was associated with greater severity of all health problems after adjusting for time on ice per game, playing position, and age.
Footnotes
Acknowledgment
The authors thank all the athletes for their participation, as well as the clubs and medical teams involved. They also thank the Norwegian Hockey Federation for access to the results from the annual 1-day, preseason testing combine, Inge Dehli Andersen for excellent help with data management, and Morten Wang Fagerland for excellent help with statistical analyses. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Health Authority, the International Olympic Committee, the Norwegian Olympic and Paralympic Committee and Confederation of Sports, and Norsk Tipping.
Final revision submitted October 4, 2021; accepted November 12, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support was received from the Sykehuset Innlandet Hospital Trust and Stiftelsen fondet til fremme av idrettsmedisin og idrettsfysioterapi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the South-Eastern Norway Regional Committee for Research Ethics (2017/1298).