
Abstract
Background:
Mental health conditions, such as depression, anxiety, and learning disabilities, are associated with symptoms that can overlap with those seen in persons with concussion. While concussion screening tools such as the Sport Concussion Assessment Tool–5th Edition (SCAT5) quantify the number of symptoms and symptom severity, it is not known whether these outcomes differ among individuals with concurrent mental health conditions compared with those without them.
Purpose:
To determine whether, during initial concussion assessment, individuals with a self-reported mental health condition have a significantly different number of self-reported concussion symptoms or symptom severity compared with those without a self-reported mental health condition (controls).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective chart review was performed on consecutive patients aged ≥13 years who underwent post-concussion assessment at the Fowler Kennedy Sport Medicine Clinic between May 2018 and March 2020 (N = 765). Most participants did not self-report a mental health condition (n = 606; 79.2%). Participants with a self-reported mental health condition (n = 159) were classified as having a learning disability (n = 14; 8.8%), anxiety (n = 62; 39.0%), depression (n = 20; 12.6%), or multiple conditions (≥2 conditions: n = 63; 39.6%). Each participant with a mental health condition was matched with 2 control participants (overall pool, n = 318) based on age, sex, student status, and sport-related risk. Mann-Whitney U tests were used to determine the statistical significance of differences between each subgroup and their matched controls for the self-reported number of concussion symptoms and symptom severity as measured using the SCAT5.
Results:
The anxiety and multiple-conditions subgroups had a significantly greater number of reported symptoms than their corresponding control subgroups (median, 17 vs 15 [P = .004] and 18 vs 14.5 [P < .001], respectively). Additionally, the SCAT5 symptom severity score was significantly greater in the anxiety and multiple-conditions subgroups than their corresponding controls (median, 49 vs 34.5 [P = .018] and 62 vs 32 [P < .001], respectively).
Conclusion:
During initial concussion assessment, both the number of concussion-related symptoms and the symptom severity were greater in study participants with anxiety and multiple mental health conditions than participants without these conditions.
Mental health conditions, such as anxiety, depression, and learning disabilities, are common among the general population, 16,43,72,84,88,92 including athletes. 53 Importantly, concussion-related symptoms overlap with symptoms of these conditions, such as difficulty concentrating and remembering, feeling slowed down or “in a fog,” being nervous or anxious, and having low energy and sadness. 17,19,21,29 The Sport Concussion Assessment Tool–5th Edition (SCAT5) measures the occurrence of symptoms and symptom severity cross-sectionally rather than asking respondents to report any change in symptoms compared with their preinjury baseline. This makes it difficult to differentiate between concussion-related and preexisting health condition–related symptoms. This presents a challenge to those who interpret the SCAT5 results, especially for individuals with preexisting mental health conditions.
There is some evidence that youth athletes with preexisting mental health conditions are evaluated with an increased number of symptoms endorsed at baseline on the SCAT5. 17,18 For example, youth athletes with attention-deficit/hyperactivity disorder (ADHD) have been found to report a significantly greater number of symptoms and higher symptom severity during baseline SCAT assessments than those without ADHD. 17,19 Additionally, collegiate and high school athletes with depression have been found to report a significantly greater number of symptoms during baseline Immediate Post-concussion Assessment and Cognitive Testing (ImPACT) than those without depression. 21 Therefore, a concussed individual with a preexisting mental health condition may also report greater post-injury SCAT5 scores than individuals without preexisting mental health conditions. Accordingly, clinicians assessing concussed athletes may not be able to reliably distinguish between symptoms attributable to their preexisting medical conditions and those that have emerged as new since the injury. Furthermore, not all athletes will have completed baseline testing, and accordingly, it may not be possible for clinicians to compare SCAT5 scores collected for concussion assessment with a pre-injury baseline. In fact, the most recent version of the SCAT states that baseline testing is not required for concussion assessment. 28 Research has yet to evaluate the effect of adult athletes’ preexisting mental health conditions on SCAT5 scores after concussion.
Evaluating different domains of concussion-related symptoms may give insight into the effects of preexisting mental health conditions on symptomatology. 3,5,8,61 One study found that the symptom domain of mental health contributes to the variance of concussion-related symptomatology. 3 Another study determined that ADHD is associated with reporting 1 or more cognitive symptoms, whereas anxiety and depression are associated with reporting 1 or more emotional symptoms. 8 Additional research is required to investigate these symptom domains in concussed individuals with mental health conditions.
The purpose of this study was to determine whether, at the time of initial presentation for medical assessment of a concussion, individuals with a self-reported preexisting mental health condition—anxiety, depression, or learning disability—had a significantly different number of concussion symptoms or symptom severity compared with individuals without a preexisting mental health condition. It was hypothesized that individuals with a preexisting mental health condition who subsequently experienced a concussion would be evaluated with a significantly greater number of symptoms and an increased symptom severity compared with individuals without the same past medical history.
Methods
The protocol for this study was approved by our ethics committee. A retrospective chart review was performed for consecutive patients diagnosed with a concussion at the Fowler Kennedy Sport Medicine Clinic, London, Ontario, between May 2018 and March 2020. The concussion diagnosis was performed by a sport and exercise physician who is a member of the Canadian Academy of Sport and Exercise Medicine, is licensed as a family physician, and has received additional training on concussion management. The diagnosis was based on the mechanism of injury, clinical examination, and reporting of symptoms. Because of the differences between the Child– and Adult–SCAT5 assessments, participants aged <13 years were excluded from the study. Of 765 patients reviewed, 477 were included in the study (Figure 1).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram illustrating the grouping of participants.
During the initial evaluation for concussion assessment, participants self-reported mental health conditions on a questionnaire. Participants who self-reported specific preexisting mental health conditions (condition group; n = 159) were organized into subgroups based on the nature of their mental health condition; the remainder of the participants (n = 412) were placed in the control pool (Figure 1). Separate condition subgroups were defined for those with a learning disability (n = 14; 8.8%), anxiety (n = 62; 39.0%), depression (n = 20; 12.6%), and multiple conditions (≥2 conditions: n = 63; 39.6%). Each participant in these subgroups was matched with 2 control participants based on sex, age, student status, and sport-related risk (1:2 matching without replacement). This 1:2 matching was performed to improve test power and estimator precision compared with 1:1 matching. 74 Sport-related concussion risk was assessed by categorizing their self-reported sport participation as either high risk (such as rugby), medium risk (such as football and ice hockey), or low risk (such as running and volleyball). 96 Individuals participating in sports were clustered as either medium or high risk, or low risk, and were matched to control individuals within the same risk cluster.
All participants also completed the Adult–SCAT5 at their initial clinic visit for concussion assessment. This tool measures the presence and severity of 22 symptoms, each rated from 0 (none) to 6 (severe), and the scores are summed to generate a symptom severity score. The total number of symptoms present and the overall symptom severity score were compared between each condition subgroup and its respective control subgroup.
Statistical Analysis
Using SPSS 27.0 (IBM Corp) and t tests, we evaluated the differences in age between the mental health condition subgroups and their respective control subgroups. Additionally, Mann-Whitney U tests were used to assess between-group differences in number of symptoms, symptom severity scores, and time (in days) from injury to initial clinical assessment. Nonparametric statistics were used, as the Shapiro-Wilk test for normality indicated that the data were not normally distributed. Furthermore, a Mann-Whitney U test was used to calculate the corresponding Z scores for each P value. The differences were considered statistically significant if P < .05.
Nonparametric effect sizes with 95% CIs were calculated using the probability of superiority approach, 79,80 using an open-source spreadsheet, GENERALISEDMW.xls, available online. 81 This measure of effect size, also called the common language effect size, 35,66 indicates the proportion of instances that a random member of the distribution with the higher mean (eg, mental health condition group) will have a higher score than a random member of the other (eg, control group) distribution. Probability of superiority values of 0.56, 0.64, and 0.71 correspond to small, medium, and large effect sizes, respectively. 35,66 Box-and-whisker plots were used to identify the median, interquartile range, and outliers of the number of symptoms, symptom severity, and time from injury to initial clinical assessment. The whiskers were extended 1.5 times the length of the interquartile range beyond the box boundaries, defining the inner fence for identifying outliers. 47 Outliers were not removed from statistical analysis. Individuals who did not report an initial clinical assessment date were removed from the Mann-Whitney U analysis.
Using SPSS 27.0 and chi-square analyses, we determined if the distributions of male and female participants, and students and nonstudents, within the condition subgroups were related to the condition itself (ie, learning disability, anxiety, depression, multiple conditions). 90 Cramer's V test was used to determine the effect size, interpreted using values of 0.06, 0.17, and 0.29 to correspond to small, medium and large effect sizes (df = 3), respectively. 54 Adjusted residuals were used to determine which cells were making the greatest contribution to the chi-square test, related to the presence of significant differences between observed and expected frequencies. Adjusted residuals >2.0 corresponded to a significantly greater difference in distribution than would be expected. Additionally, chi-square analyses were used to determine if there were significant differences in the proportion of individuals who reported a history of concussion in each condition subgroup. Cramer's V test was used to determine the effect sizes as described above (df = 1).
Factor weightings were extracted from studies that performed exploratory factor analysis on SCAT symptom scores 3,5 or reported symptom domain groupings. 8,61 These factor weightings were used to calculate factor scores for all participants, 44 following the 3-factor (Migraine Fatigue, Affective, Cognitive-Ocular), 5 4-factor (Physical/Somatic, Insomnia/Sleep, Emotional, Cognitive), 8,61 and 5-factor (Energy, Mental Health, Migrainous, Cognitive, Vestibulo-ocular) 3 schemes. Using SPSS 27.0, we ran 2-way analyses of variance for each factor, investigating whether the factor scores were significantly different between mental health conditions, and between the control and condition subgroups. Levene tests of equality of error variances were not performed, as they are not recommended for large sample sizes. 51,104
Results
All individuals reporting a mental health condition identified as having a learning disability, anxiety, depression, or multiple conditions. Three of the 4 subgroups had a greater proportion of female participants (anxiety, 58.1%; depression, 65.0%; multiple conditions, 68.3%); the learning disability subgroup had a smaller proportion of female participants (28.6%) (Table 1). This sex distribution varied significantly within the mental health condition groups (χ2 = 7.87; df = 3; P = .049), with a large effect size (Cramer's V = 0.35). Based on the adjusted residuals, the learning disability subgroup (adjusted residual magnitude, 2.55) was the only mental health condition subgroup with a significantly different sex distribution when compared with the other condition subgroups. There were no significant differences in age between the condition groups and their respective control groups.
Demographics and Concussion-Related Characteristics for Participants in Each of the Mental Health Condition Subgroups and Their Respective Control Groups

a The number of participants (n) was doubled in the respective control subgroups based on the 1:2 matching.
b The percentage of female participants was identical between the mental health condition subgroups and their respective control subgroups based on the matching.
c Statistically significant difference between condition and control subgroups (P < .01; χ2 test).
Between 80% and 100% of the participants in each condition and corresponding control group reported a sport-related cause for their concussion (Table 1). Additionally, approximately 40% to 65% of individuals in each condition and corresponding control group reported a history of concussion and had experienced ≥1 previous concussion (Table 1). The proportion of individuals reporting a history of concussion was significantly greater in the anxiety and multiple-conditions subgroups than their respective control subgroups (χ2 = 4.75, df = 1, P = .043, Cramer's V = 0.16; and χ2 = 8.30, df = 1, P = .005, Cramer's V = 0.21, respectively). However, history of concussion did not vary significantly between the depression and learning disability subgroups and their respective control subgroups (χ2 = 0.84, df = 1, P = .418, Cramer's V = 0.12; and χ2 = 0.44, df = 1, P = .530, Cramer's V = 0.10, respectively). Most individuals in the learning disability subgroup fell within the age range of 13 to 16 years, whereas more individuals in the depression, anxiety, and multiple-conditions subgroups fell in the 17- to 20-year age category (Table 2).
Percentage of Individuals in the Mental Health Condition Subgroups and Respective Control Subgroups Across 5 Age Categories a

a Data are reported as the percentage of the overall number of participants within each subgroup.
The proportion of individuals who self-reported a mental health condition did not differ by student status (χ2 = 2.55; df = 3; P = .466) (Table 1). All mental health condition groups tended to have greater average symptom severity scores, number of symptoms, and number of days between injury and initial clinical visit compared with their respective control groups (Tables 3 and 4). The anxiety and the multiple-conditions subgroups showed the largest differences in symptom severity score and number of symptoms compared with their corresponding control subgroups (Figure 2).
Comparison of SCAT5 Symptom Severity Score and Number of Symptoms at Initial Concussion Assessment Between the Condition Subgroups and Respective Control Subgroups a

a Boldface P values indicate a statistically significant difference between the condition subgroup and control subgroup (P < .05; Mann-Whitney U test). IQR, interquartile range; SCAT5, Sport Concussion Assessment Tool, 5th Edition.
b Medium effect size.
c Small effect size.
Comparison of Time Between Injury and Initial Clinical Assessment for Concussion Between the Condition Subgroups and Respective Control Subgroups a

a Boldface P values indicate a statistically significant difference between the condition subgroup and control subgroup (P < .05; Mann-Whitney U test). IQR, interquartile range.
b Small effect size.
c Large effect size.
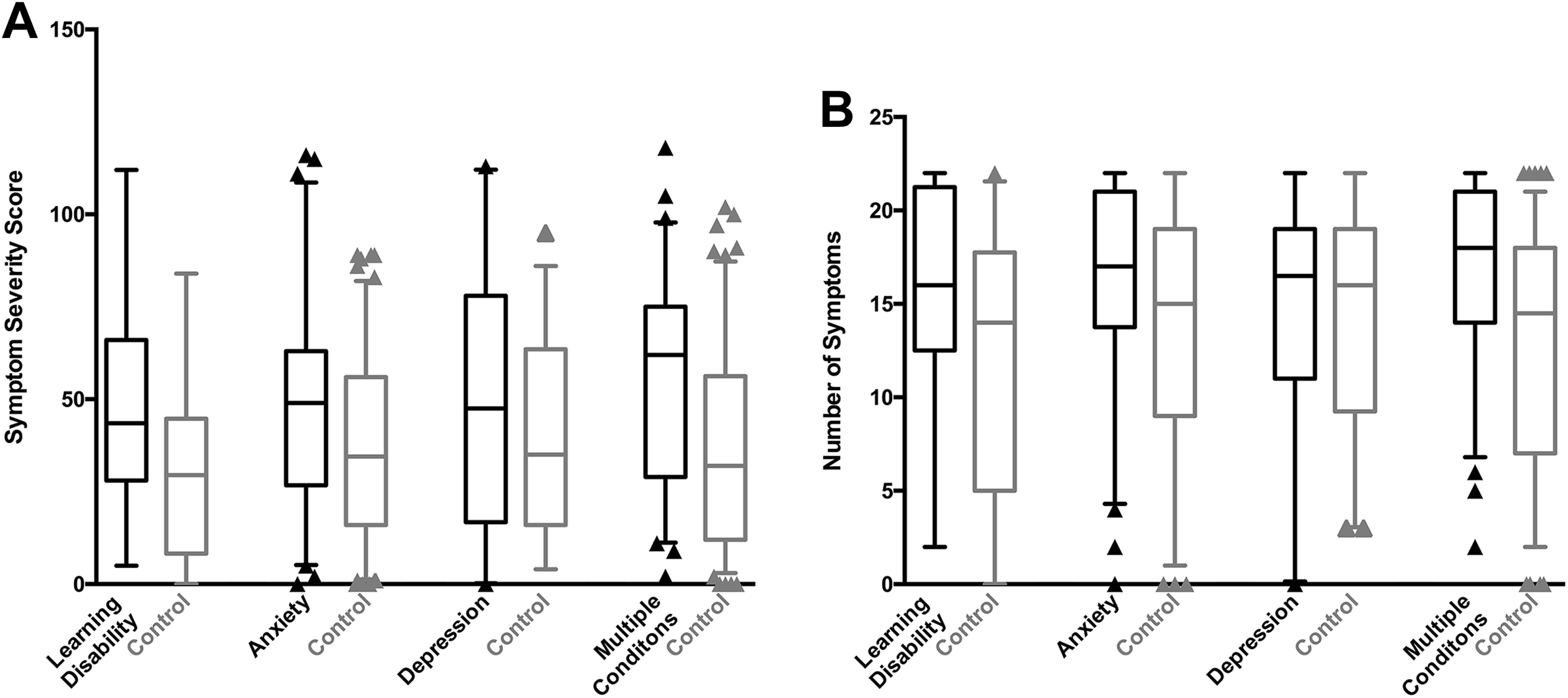
Box-and-whisker plots illustrating (A) Sport Concussion Assessment Tool–5th Edition (SCAT5) symptom severity scores and (B) number of SCAT5 symptoms for the mental health condition subgroups and their corresponding control subgroups. The bars illustrate the medians, the boxes illustrate the interquartile range (IQR), the whiskers extend 1.5 times the length of the IQR, and the triangles illustrate outliers.
Individuals with self-reported anxiety had significantly higher average symptom severity scores and a significantly greater average number of symptoms (P = .018 and .004, respectively) compared with their control subgroup (Table 3 and Figure 2). Similarly, individuals who self-reported multiple mental health conditions had significantly higher average symptom severity scores and a significantly greater average number of symptoms compared with their control subgroup (P < .001 for both) (Table 3 and Figure 2). There were no significant differences in average symptom severity scores or the average number of symptoms for either the depression or the learning disability subgroups, although the effect sizes for these comparisons ranged from small to medium (Table 3 and Figure 2).
All condition groups had a greater number of average days between injury and initial clinical assessment than their respective control group (Table 4). There were significant differences in the number of days from injury to initial assessment between the control subgroup and the anxiety (P = .016), depression (P = .013), and multiple-conditions (P = .002) subgroups (Table 4); however, there was no significant difference in this outcome between the learning disability subgroup (P = .215) and its control subgroup. Effect sizes for number of days from injury to initial assessment ranged from small to large (Table 4). All condition and control groups contained outliers.
Considering the symptom scores in each of the factor domains, the interaction between mental health conditions and control/conditions was not statistically significant, and there were no statistically significant differences between the mental health condition subgroups for all symptom factor domains (all P > .05). However, the symptom factor scores were significantly higher in the mental health condition groups than the corresponding control groups for all symptom factor domains (all P < .05) (Table 5).
Comparison of Overall SCAT5 Symptom Scores Between the Condition and Control Groups Using 4-Factor Loading Sources and Their Respective Symptom Factor Categories a

a Data are reported as mean ± SD. Boldface P values indicate a statistically significant difference between the condition group and control group (P < .05; 2-way analysis of variance). The interactions between mental health conditions and control conditions were not statistically significant. There were no statistically significant differences between mental health conditions. SCAT5, Sport Concussion Assessment Tool–5th Edition.
Discussion
It was hypothesized that participants with a preexisting mental health condition—anxiety, depression, a learning disability, or multiple conditions—would report a greater number of symptoms and an increased symptom severity as assessed by the SCAT5 at the time of initial concussion assessment compared with control participants. This study determined that during initial concussion assessment, individuals who self-report preexisting anxiety or multiple mental health conditions had a significantly greater number of symptoms and higher symptom severity compared with individuals without a preexisting mental health condition. However, participants with a history of depression or a learning disability in isolation did not differ significantly from control participants without a preexisting mental health condition. Factor scores for each of the different factor schemes were not significantly different between the mental health conditions.
Concussion Assessment Tools
Concussion assessment tools are used for diagnosis and monitoring of recovery. 24,49,71 This study examined the symptom evaluation component of the SCAT5 tool in individuals undergoing a concussion assessment. 28 SCAT5 evaluates for common immediate and delayed symptoms related to concussion. 8,28,61 Interpretation of the SCAT5 scores does not require baseline data. 28 Although clinicians can diagnose concussions using normative data, 28 baseline measures are necessary for intraindividual comparisons with a nonconcussed state. 28 As we observed that individuals with anxiety or multiple mental health conditions have a significantly greater number of symptoms and severity of symptoms compared with matched control participants, data for individuals with these mental health conditions should not be compared with normative baseline values. Rather, baseline data should be collected for individuals with a mental health condition, as this enables the monitoring of intraindividual changes in symptomatology.
In addition to the symptom evaluation, the SCAT5 includes cognitive and neurological screening sections to evaluate memory, concentration, coordination, and balance. 28 Medical professionals rely on an individual’s self-reported symptoms as one criterion for diagnosing concussions; therefore, our study was limited to the symptom evaluation. 9,76 Although concussion assessment tools are available, medical professionals are not mandated to use them to diagnose concussion. 9,75 The Brief Symptom Inventory–18 (BSI-18) is similar to the SCAT5 as it also aims to assess and quantify individuals’ symptoms related to psychological distress and psychiatric disorders. 24 The ImPACT is another common tool composed of neurocognitive tests, vestibulo-ocular motor screening, and the Balance Error Scoring System. 71 As further evidence of the importance of symptom evaluations, research using concussion assessment tools often evaluates symptoms even when the tools themselves do not. 49,99
Concussion assessments can be used to monitor the recovery of signs and symptoms; however, they do not monitor the physiological recovery of the brain. 26,36,37,40,85 Neuroimaging has been employed to quantify the change in brain physiology due to concussion, expanding beyond the use of concussion assessment tools. 26,36,37,40,85 Brain physiology can be measured through modalities such as diffusion tensor imaging (DTI), 37 magnetic resonance spectroscopy (MRS), 36 and functional magnetic resonance imaging (fMRI). 40,65,85 Unlike computed tomography and MRI, DTI, MRS and fMRI can be used to detect physiological disturbance associated with concussion. 85 While providing insights, they require costly off-field equipment, 85 which limits their widespread adoption. In contrast, concussion assessment tools such as SCAT5, BSI-18, and ImPACT are more feasible.
Assessment of Concussion Symptoms in Patients With Mental Health Conditions
Research has shown that individuals with mental health conditions reported a significantly higher number of symptoms and symptom severity during preconcussion baseline testing using assessment tools such as the Child–SCAT, ImPACT, and BSI-18. 17,19,99 Literature investigating baseline Child–SCAT scores also found that preexisting ADHD was associated with a greater number and severity of symptoms. 17,19 Additionally, literature investigating the Adult–SCAT as a baseline test has found that individuals with anxiety, depression, and multiple mental health conditions reported a significantly greater number and severity of symptoms compared with an extremely large independent control group (>29 times larger than any of the mental condition groups), which may have resulted in an overpowered study. 99 This is a concern since overpowered studies can produce outcomes that are statistically significant yet have little practical meaning. 101
To the best of our knowledge, this is the first study to show that individuals with preexisting anxiety or multiple mental health conditions have a significantly greater number of symptoms and symptom severity when undergoing initial screening with the SCAT5 after suspected concussion. This differs from the current baseline testing literature and might be explained by the inflated power in the study by Weber et al, 99 as they noted their results were likely affected by oversampling. Additionally, both Weber et al and Collings et al, 17 in their studies of baseline testing, did not case-match for each participant but rather compared condition groups with the entire pool of controls. In contrast, while Cook et al 19 did case-match participants, they did not evaluate any preexisting mental health conditions other than ADHD. Our experiment had a greater number of participants with learning disabilities in the multiple-conditions group than in the isolated learning disabilities group. Accordingly, a significant proportion of the participants in the Cook et al study may have had multiple conditions rather than an isolated learning disability. Additionally, Cook et al used the Child–SCAT, 23 requiring both the child and the parent to report the child’s symptoms. The parent’s perception of the child’s symptoms may differ from the child’s true experience; furthermore, children may possibly struggle to fully understand the extent of their symptoms or how to properly report them. 23,69
Factor Scores and Mental Health Conditions
We did not observe any statistically significant differences in factor scores between the mental health conditions for any of the factor schemes. 3,5,8,61 In contrast, Asken et al 8 found that individuals with psychiatric disorders (depression and anxiety) had higher scores in the Emotional domain. These differences may be because of the different study populations since Asken et al 8 studied nonconcussed individuals while the current study evaluated individuals who were being assessed for concussion. Additionally, we observed that the mental health condition groups had higher scores on all domains compared with their corresponding control groups. This is consistent with our findings of an increased total number of symptoms in mental health condition groups compared with their respective control groups. Therefore, the division of symptoms into factor domains did not reflect any information beyond the total symptom score measure.
Time From Injury to Assessment
In our study, condition group individuals attended their initial clinical assessment on average more days post-injury than individuals in the respective control group. Individuals in the depression, anxiety, and multiple-conditions subgroups took significantly more days to attend a clinic than individuals in the control subgroups. This difference in duration suggests a delay in seeking treatment. This is consistent with literature stating that people with mental health conditions are more likely to engage in poor personal health behaviors, such as delaying evaluation when medical care is needed. 64,67,103 This is further seen through the factor analysis of SCAT5 symptoms, in which individuals with higher symptom scores related to the Mental Health domain are associated with a longer time between injury and assessment. 3 While 1 in 3 individuals will eventually seek treatment for their mental health condition, 95,98 the initial evaluation is often delayed from the initial onset of symptoms. On average, individuals with a mood disorder will delay treatment for 8 years, while those with an anxiety disorder will delay for 9 years. 95,97 This may be related to the internalized stigma of mental health conditions, which has been associated with longer delays in seeking treatment 25 and decreased treatment adherence. 70 Furthermore, the Lauver's theory of care-seeking behavior states that a series of psychosocial variables, including anxiety, play a significant role in determining when an individual will seek health care. 87 Individuals with mental health conditions are more likely to avoid seeking health care, even when they suspect they should. 103 Health care avoidance is a significant barrier to and has a negative effect on the well-being of individuals with mental health conditions. 103 Similarly, when immediate diagnosis and treatment for a concussion are not sought, the individual increases their risk of experiencing a delay in healing; an increase in symptom severity; an increase in time away from work, school, and/or sport; or second-hit syndrome. 6,7,10,12,30,45,48,100
However, the observed delay in seeking treatment is the opposite of what is expected, according to the diasthesis-stress model. 102 In this model, a concussion would be considered a significant stressor and therefore would likely result in the presentation of previously dormant psychological difficulties. 8 For individuals with mental health conditions, the sudden onset of new symptoms can lead to catastrophic thinking. 31,83 According to Ellis, 31 catastrophic thinking is the tendency to magnify a perceived threat and overestimate the seriousness of its potential consequences. Catastrophizing leads to avoidance and safety-seeking behaviors. 38 Individuals avoid situations that lead to perceived negative outcomes and react to these outcomes by partaking in safety-seeking behaviors. 38 Safety-seeking behaviors would likely urge individuals to seek treatment sooner than their noncatastrophizing counterparts. However, individuals with mental health conditions that lead to catastrophizing avoid seeking treatment, as it can lead to a diagnosis, solidifying their catastrophic thoughts. 38 Catastrophic thinking ultimately leads to a delay in seeking and attending treatment. 68,91
Self-Reporting Symptoms and Mental Health Conditions
Individuals with mental health conditions are known to ruminate, overanalyze, and catastrophize 31,33,94 ; however, research has yet to investigate how this may affect self-reported concussion symptoms. Self-reporting symptoms has been associated with the inaccurate portrayal of pre– and post–mild traumatic brain injury symptoms in children and adults. 56,62,63 Similarly, in individuals without mental health conditions, this can be due to poor effort during testing or the exaggeration of one’s symptoms. 59 These inaccuracies can lead to personal gain, such as financial gain for adults, 62,63 or getting out of tasks for children. 55 Exaggeration may be purposeful, such as “sandbagging,” 32 or unknowing. The phenomenon of unknowingly exaggerating one’s symptoms is referred to as the “good old days” bias. 42 This bias is the outcome of an individual’s viewing one’s past state of symptoms as “better” than one’s current state. 42,50,60 This can lead to the inaccurate portrayal of past symptoms and the misinterpretation of current post-injury symptoms as new. 42,50,60 Research has yet to investigate if there is a link between the good old days bias and increased symptom exaggeration in individuals with mental health conditions.
Studies have shown that concussed individuals without mental health conditions exhibit higher pain catastrophizing associated with having more post-concussion symptoms. 14,41 Multidimension symptom exaggeration has also been observed in individuals with depression. 78 This may correspond to these individuals’ exaggerating their concussion symptoms, resulting in increased self-reported symptom severity and perhaps an increased number of symptoms. Additionally, individuals with depression and anxiety show a similar symptomatology to post-concussion syndrome. 13,42 Accordingly, the increased number and severity of concussion symptoms observed in the current experiment may be related to a combination of exaggerated symptoms and genuine dysfunction. 78
Ratio of Male to Female Participants
In our study, a greater proportion of male participants self-reported learning disabilities than female participants, whereas a greater proportion of female participants self-reported anxiety, depression, and multiple mental health conditions. The latter difference is expected in part due to the larger number of female participants recruited to the study sample. Our study population is also in keeping with the existing literature, which has demonstrated that a greater proportion of female participants self-report anxiety and depression than male participants. 1,57,89 The larger proportion of male participants seen in the learning disability subgroup is consistent with the existing scientific literature reporting on the demographic data from athletes and adults with mental health conditions. ¶ Additionally, our study population is consistent with previous literature reporting that males are diagnosed with learning disabilities at a higher rate than females. 39,86,93 Interestingly, these subgroup proportions are likely related to sex-based differences in mental disorder diagnoses. 1,39,46,52,77 This is directly linked to referral bias and gender stereotypes in the Fifth edition of the Diagnostic and Statistical Manual of Mental Disorders. 4
Clinical Relevance
In the anxiety and multiple-conditions subgroups, the number of symptoms and symptom severity were significantly greater than in their respective control subgroups; however, they had a small and medium effect size, respectively. In contrast, although not statistically significant, there were medium effect sizes associated with greater number of symptoms and symptom severity for the learning disability subgroup compared with its respective control subgroup and small effect sizes associated with greater number of symptoms and symptom severity for the depression subgroup compared with its respective control subgroup. Accordingly, these differences are practically important. 73 Clinicians will often need to interpret the SCAT5 results with no baseline assessment data available for comparison. Not only does the latest version of the SCAT5 not require the completion of a baseline assessment, 22 but also baseline assessments are not practical outside of athletes participating in certain organized sports. Normative data are readily available for athletes with a valid baseline and acute SCAT5 evaluations, 11,15,27,58 excluding individuals with neurological and balance disorders, 27 concomitant illness or injury, 58 and multiple evaluations for suspected concussion or multiple prospective diagnosed concussions. 11 However, these normative values may not be applicable to all individuals post-concussion given that the current study has provided evidence to suggest that some preexisting mental health conditions—such as anxiety, depression, and learning disabilities in adults and athletes 16,43,53,72,84,88,92 —may be associated with differences in symptom number and severity post-injury. Additionally, the normative values for symptom number and severity developed using the entire population may be inappropriately inflated for individuals without concurrent mental health conditions. In order for clinicians to properly interpret SCAT5 scores and develop appropriate management plans, they must understand the effects of preexisting mental health conditions on symptom number and severity and must have access to a complete past medical history for each athlete undergoing assessment. This study indicates that clinicians should consider the effects of preexisting anxiety or multiple mental health conditions on an individual’s concussion-related symptomatology at the time of initial evaluation. Future research should assess the effect of additional mental health conditions—such as posttraumatic stress disorder (PTSD), substance abuse, and psychosis—and investigate whether individuals with mental health conditions have altered concussion recovery compared with individuals without mental health conditions.
Limitations
A primary limitation of this study was the sample used. All participants were concussed, and accordingly, we were unable to make comparisons between concussed and nonconcussed individuals with mental health conditions. Additionally, the sample only contains individuals who actively sought health care for their concussion at a single clinic. Furthermore, the clinical questionnaires in use in this clinic did not prompt patients to report an exhaustive list of mental health conditions; specifically, patients were not prompted to report a history of PTSD, psychosis, or substance abuse. This limits the generalizability of our findings to a specific context and population, in addition to the single-site sample population. Furthermore, most individuals in this sample sustained a sport-related concussion, which also limits the generalizability of the findings. An additional limitation is that we were unaware of what prompted participants to attend the clinic (eg, a change in daily symptoms or advice from a peer). Therefore, it is not known if those with mental health conditions attended the clinic because of a noticeable difference in their usual daily symptoms as an outcome of a concussion. Furthermore, it is possible that some individuals did not attend the clinic, as mild concussion-related symptoms may not have been sufficiently different from their daily symptoms thus not prompting the need to seek health care. Future studies would benefit from recruiting participants with sport- and non–sport related concussion origins as well as collecting data on a wider range of preexisting mental health conditions. Additionally, studying individuals with physician-diagnosed mental health conditions rather than basing analysis on participant self-report would be advantageous. Individuals may self-report a mental health condition yet have limited or subtle symptoms, whereas physician-diagnosed conditions are derived from a clinically informed decision and evidence-based diagnostic criteria. Furthermore, individuals may choose to not self-report a mental health condition because of the social pressure or related stigma, regardless of a formal diagnosis. 20,34,57,82,89
Conclusion
Understanding how preexisting mental health conditions can affect the number and severity of concussion symptoms is important and can aid clinicians in the interpretation of SCAT5 symptom evaluation scores at the time of initial presentation for concussion assessment. Given that individuals with preexisting anxiety or multiple mental health conditions report an increased number of symptoms and symptom severity on the SCAT5 after concussion, clinicians should choose to take a complete past medical history before interpreting their patients’ scores. Furthermore, normative data should be used with caution for individuals with mental health conditions. More research is needed to determine how other mental health conditions may affect SCAT5 symptom and severity scores.
Footnotes
Acknowledgment
The authors thank the patients and staff at the Fowler Kennedy Sport Medicine Clinic for participating in and assisting with this study.