
Abstract
Background:
Soft tissue interposition between a suspensory cortical button and the lateral femoral condyle is the most common cause of postoperative suspensory cortical button migration in patients undergoing anterior cruciate ligament reconstruction (ACLR).
Purpose:
To investigate the effects of soft tissue interposition and suspensory cortical button migration after ACLR on functional outcomes and graft ligamentization.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 249 patients who underwent single-bundle ACLR with hamstring tendon autografts. To measure soft tissue imposition, the patients were divided into 2 groups: those in whom the suspensory cortical button was in contact with (group 1) or at least 1 mm away from (group 2) the lateral femoral condyle on 1-day postoperative radiographs. To measure suspensory cortical button migration, the patients in group 2 were further divided into 2 subgroups: those with button migration (group M) and those without migration (group non-M) as observed on 12-month postoperative radiographs. Ligamentization was evaluated according to Howell classification (grades 1-4) on 12-month follow-up magnetic resonance imaging scans. Also recorded were preoperative and 24-month postoperative Lysholm and Tegner scores and 24-month postoperative arthrometer measurements for anterior knee laxity.
Results:
There was no significant difference between groups 1 and 2 or between groups M and non-M in terms of demographic characteristics or additional intra-articular pathologies detected intraoperatively. Normal anterior laxity (<3 mm) was detected in 83.7% of the patients postoperatively, and all patients showed statistically significant pre- to postoperative improvement on the Tegner (from 4.1 to 4.3) and Lysholm (from 44.0 to 89.2) scores (P < .05 for both). No significant difference in postoperative functional results or graft ligamentization was found between either the soft tissue interposition groups (groups 1 and 2) or the suspensory cortical button migration groups (groups M and non-M).
Conclusion:
Differences between patients in soft tissue interposition and suspensory cortical button migration did not significantly affect postoperative clinical or functional outcomes or graft ligamentization after single-bundle ACLR.
Anterior cruciate ligament (ACL) rupture is one of the most common sports injuries, occurring in 43.5 out of 100,000 people each year. 13 It has been reported that 92% of orthopaedic surgeons specializing in sports medicine believe there is a limited role for nonoperative treatment of ACL rupture in high-level athletes, and it has been reported that more than half of these surgeons use hamstring tendon autografts in primary ACL reconstruction (ACLR). 17 While there are many options for femoral fixation of the graft during ACLR, the current global trend shows that 50% of surgeons prefer a suspensory cortical button for femoral fixation. 17,22 Two different types of suspensory cortical buttons, adjustable-loop and fixed-loop, are available for use in ACLR; however, a fixed-loop suspensory cortical button has been associated with less postoperative graft slippage compared with an adjustable suspensory cortical button. 9
Suspensory cortical buttons, which are used frequently for femoral fixation during ACLR, can cause perioperative and postoperative complications such as graft failure and local soft tissue irritation, in addition to suspensory cortical button misplacement, which is the most common complication. 22 While the coronal and sagittal misplacement of a suspensory cortical button has been investigated in many studies, no significant relationship has been found between the location of the suspensory cortical button on the sagittal plane and postoperative clinical and functional results. 7 The cause of the misplacement is reported as “soft tissue interposition,” in which the suspensory cortical button has no flush contact with the lateral condyle of the femur in the coronal plane. 8,15,21,22
Early necrosis of interposed tissue may cause loss of graft tension and continuing graft-tunnel motion can negatively affect the healing process. 19 Although soft tissue interposition has been reported as the most common cause of postoperative suspensory cortical button migration, it has also been shown that suspensory cortical button migration and soft tissue interposition ≤2 mm have no effect on postoperative clinical and functional outcomes. 8,12 Upon review, we could not find any study investigating the effects of soft tissue interposition and/or suspensory cortical button migration on postoperative graft ligamentization.
The study aims were to investigate the effects of soft tissue interposition and of suspensory cortical button migration on functional outcomes and graft ligamentization after ACLR. We hypothesized that soft tissue interposition and consequent suspensory cortical button migration would not have a significant effect on the postoperative clinical and functional outcomes or on graft ligamentization.
Methods
Approval of the ethics committee of our university was obtained for this retrospective study, as it was a retrospective study no informed consent was needed from participants. A total of 425 patients were operated on by a single senior surgeon (R.A.) for ACL rupture between January 2012 and June 2019 in our clinic. Included were patients who had undergone anatomic single-bundle ACLR and femoral fixation with a fixed suspensory cortical button. Excluded were patients with multiligament injuries; those who underwent revision reconstruction, double-bundle ACLR, or all-inside ACLR; those who were treated with adjustable suspensory cortical buttons; those who received quadriceps tendon grafts or allografts; those having had surgery on the opposite knee; and those without 12-month follow-up knee radiographs or 24-month follow-up data. Overall, 249 patients met the inclusion criteria (Figure 1).
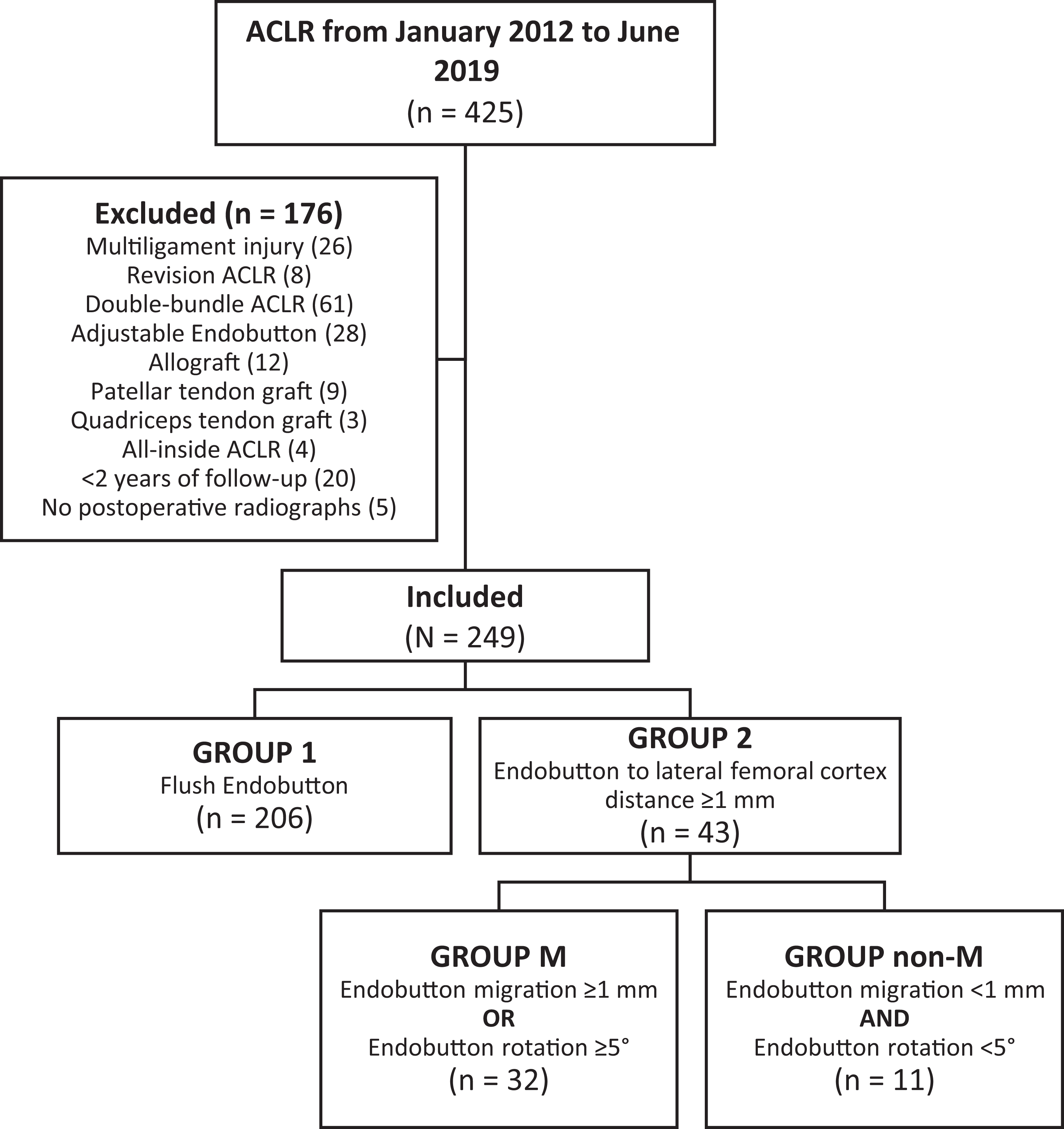
Flow diagram of patient inclusion. A total of 249 patients were included, with patient distribution among the study groups as shown. ACLR, anterior cruciate ligament reconstruction.
Surgical Technique and Postoperative Rehabilitation
The surgery for all patients was performed by the same senior surgeon with patients under spinal-epidural anesthesia. After the standard arthroscopic anterolateral and anteromedial portals of the knee were opened, diagnostic arthroscopy was performed to evaluate the cartilage tissues on the joint surfaces, medial and lateral menisci, and the ACL. Diagnostic arthroscopy was performed to evaluate for associated pathology. Autologous gracilis and semitendinosus tendons obtained from a 4-cm oblique skin incision made 2 cm medial to the tibial tubercle were used. Meniscal pathology was addressed accordingly, and patients were included regardless of repair versus meniscectomy. The cartilage lesions were graded according to Outerbridge classification and were treated with chitosan-based liquid scaffold, hyaluronan-based soft scaffold, or chondroplasty if needed. 2
After the remnants of the native ACL were debrided, the femoral tunnel entry site was determined as the far medial portal, the knee was flexed to 120°, and the femoral tunnel was created using a 4.5-mm femoral drill over the 2.5-mm guide wire via far medial portal. 3 An appropriately sized tibial tunnel was drilled through the anteromedial portal using a tibial aiming guide (Acufex; Smith & Nephew, Inc). Femoral fixation was performed using fixed-loop suspensory cortical buttons (Endobutton CL; Smith & Nephew, Inc) loaded with 6-fold autologous grafts, with a loop length of 20 mm when the femoral tunnel length was ≥40 mm or with a loop length of 15 mm when tunnel length was <40 mm. Tibial fixation was performed using bioabsorbable screws (Biosure; Smith & Nephew, Inc) 1 mm thicker than the graft thickness with the knee flexed at 15° and maximum tension applied to the graft. 3 In all patients, a 4.5-mm tibial postfixation screw (Smith & Nephew, Inc) was used for additional fixation. Intraoperative fluoroscopy was not used in any of the study patients.
A standard rehabilitation program was applied to all patients. For patients who underwent meniscal repair, knee flexion was restricted to 90° use for 3 weeks. Partial weightbearing was permitted with crutches; no braces were used for 3 weeks. The crutches were used for 3 weeks, and exercises were directed predominantly to full knee flexion. In postoperative weeks 6 to 12, walking exercises and mild running were added, and isotonic and strengthening exercises were increased. After 45 days, cycling was permitted. Sports-specific exercises such as jumping and changing direction while running were started after 3 months, but return to active sports was not permitted until 9 months. 3
Radiological Evaluation
Preoperatively, all patients underwent anteroposterior (AP) and lateral knee radiographs as well as long-leg radiographs for coronal mechanical axis evaluation. Postoperative AP and lateral knee radiographs were performed at 1-day, 6-week, 3-month, and 12-month follow-up, then annually thereafter. Femoral tunnel width, femoral tunnel angle, tibial tunnel width, and the distance between the suspensory cortical button and the lateral femoral condyle (LFC) were measured on the 1-day and 12-month postoperative AP radiographs (Figure 2). 8 The radiographic measurements were performed independently by 2 orthopaedic surgeons (E.A.O., M.O.K.) twice with an interval of 2 weeks. The intra- and interobserver reliability of the measurements showed substantial agreement (κ = 0.75 and 0.76, respectively). 11
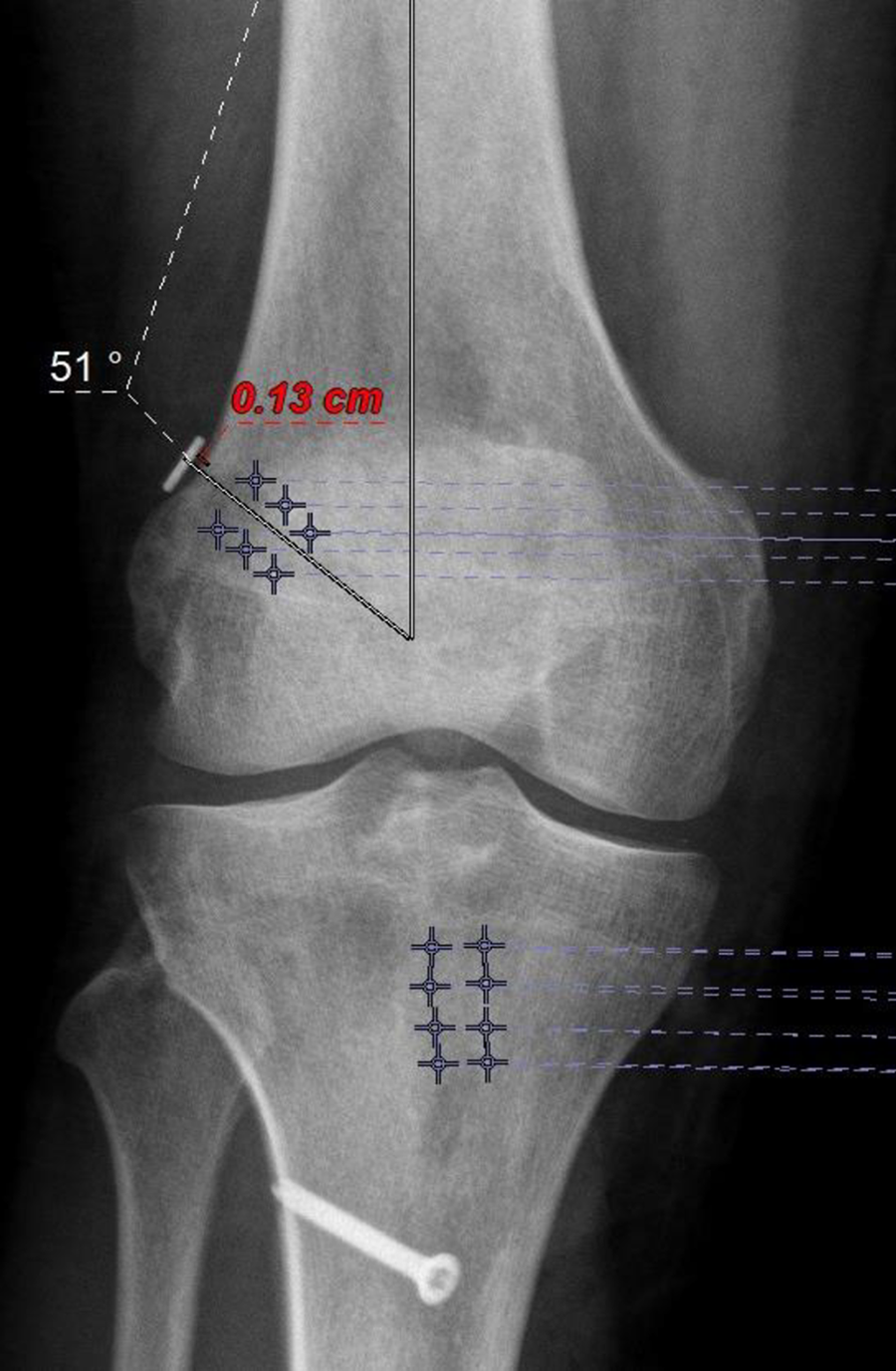
Anteroposterior radiograph of a knee taken on postoperative day 1. The femoral tunnel angle was measured as 51° and the distance between the suspensory cortical button and the lateral femoral condyle as .13 cm. Boundaries of the femoral and tibial tunnels are marked.
For analysis of soft tissue interposition, the patients were divided into 2 groups based on the 1-day postoperative radiographs: those in whom the suspensory cortical button was in contact with the LFC (group 1; n = 206) and those in whom the button was at least 1 mm from the LFC (group 2; n = 43). For both groups, the location (anterior/middle/posterior) and angle of the suspensory cortical button were measured on 1-day and 12-month postoperative lateral radiographs (Figure 3). 7,8

Lateral radiograph of a knee taken on postoperative day 1. In the sagittal plane, the distal femur is divided into 3 equal parts. The suspensory cortical button can be seen located posteriorly. The suspensory cortical button angle was measured as 37°.
To analyze suspensory cortical button migration, patients in group 2 were further divided into 2 subgroups: those in whom the suspensory cortical button had migrated (group M; n = 32) and those in whom it did not migrate (group non-M; n = 11). Button migration was defined as ≥1 mm movement on the femoral tunnel axis or ≥5° of button rotation on 12-month postoperative radiographs with respect to 1-day postoperative radiographs. 8,12,21 The amount of rotation of the suspensory cortical button was evaluated regardless of which direction it rotated.
Functional and Clinical Evaluation
The preoperative and 24-month postoperative records of all patients were evaluated retrospectively, including preoperative and postoperative pivot shift (grades 1-3), Lachman (grades 1-3), and Tegner and Lysholm scores. At 24-month follow-up, side-to-side differences in anterior knee laxity were recorded using a KT-1000 arthrometer with 134-N loads applied to both knees.
Graft Ligamentization
At our clinic, knee magnetic resonance imaging (MRI) scans are taken routinely for all patients after ACLR to evaluate ligamentization 12 months postoperatively. The Howell classification (grades 1-4) was used for the evaluation of ligamentization on the 12-month postoperative MRI scans of the patients. 3,10 The autograft was considered grade 1 if it showed the same homogeneity and hypointensity as the patellar tendon and the posterior cruciate ligament, grade 2 if >50% of the graft volume showed normal intensity, grade 3 if <50% of the graft volume was in normal ligament appearance, and grade 4 if there was diffuse increased intensity in the autograft and the graft strands did not appear normal (Figure 4). 3

T2-weighted sagittal magnetic resonance imaging scan taken at 12 months postoperatively demonstrating (A) Howell grade 2 ligamentization (>50% of the autograft volume with the same homogeneity and hypointensity as the patellar tendon and PCL) and (B) Howell grade 1 ligamentization (autograft with the same homogeneity and hypointensity as the patellar tendon and PCL). PCL, posterior cruciate ligament.
Statistical Analysis
The Stata/MP Release 13 software (StataCorp LLC) was used for descriptive and inferential analyses. The Shapiro-Wilk test was used to assess normality. The mean with standard deviation along with the maximum and minimum values were used to present the continuous data. The chi-square and Fisher exact tests were used for categorical variables. The t test was performed to analyze the parametric data between groups, and the Mann-Whitney U test was performed to analyze nonparametric data. The Wilcoxon sign-rank test was used to analyze the data between the dependent groups (pre- vs postcomparison). P < .05 was accepted as significant.
Using a receiver operating characteristic curve with Youden index calculation, we performed a cutoff analysis to determine the value of the distance from the cortical button to LFC after which the risk of migration was greater.
Results
The 249 study patients had a mean age of 34.3 ± 11.1 years. There were 210 male and 39 female patients, and the right side was affected in 53.4%. The mean time from ACL rupture to surgery was 13.8 ± 14.9 months. There were 82 patients (32.9%) with a preoperative pivot-shift grade of 3, and 78 patients (31.3%) had a preoperative Lachman grade of 3 (Table 1). When comparing these variables between the soft tissue interposition groups (groups 1 and 2) and between the cortical button migration groups (groups M and non-M), the only significant difference was that the mean age of the patients in group 1 was significantly older compared with group 2 (35.0 vs 31.3 years; P = .02) (Table 1).
Baseline Patient Characteristics Overall and Compared Between Study Groups a
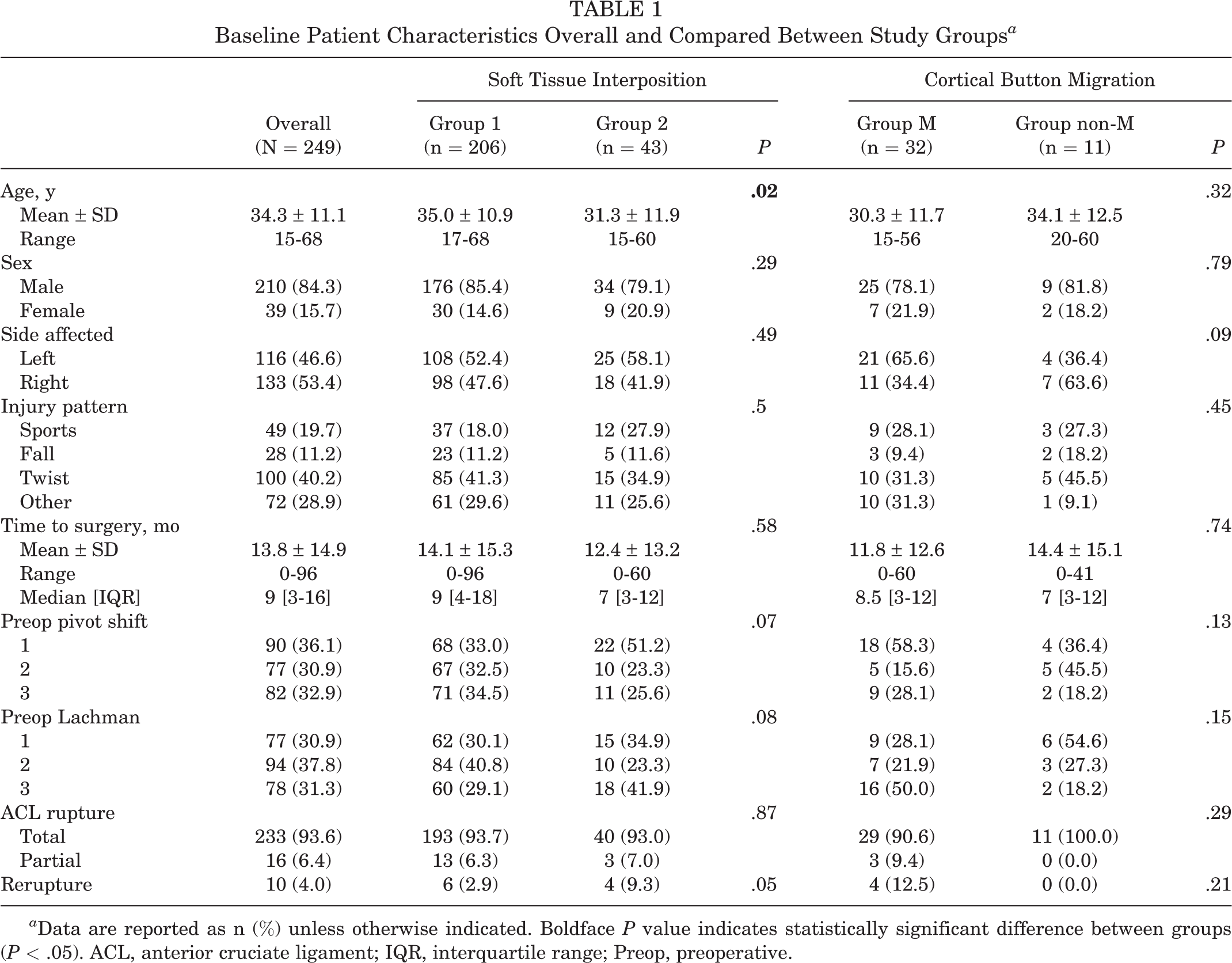
a Data are reported as n (%) unless otherwise indicated. Boldface P value indicates statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; IQR, interquartile range; Preop, preoperative.
Overall, 55% of patients had medial and 8.8% lateral meniscal pathologies. Ramp lesions were detected in 2% of the patients and posterior root rupture of the lateral meniscus in 2%. There were no significant differences in the distribution of these findings among the groups. Regarding the lateral meniscus, there were significant differences between groups 1 and 2 in the distribution of repaired menisci (6.3% vs 6.9%; P = .02) and meniscectomies (0.4% vs 0%; P = .02). Cartilage pathologies were detected in the medial tibiofemoral compartment in 7.2% of the patients and in the lateral tibiofemoral compartment in 1.6%, with no difference in distribution among the groups. For the treatment methods, hyaluronan- or chitosan-based scaffolds were used in group 1 but not in group 2 (Table 2).
Intraoperative Findings and Treatments a

a Data are reported as n (%). Boldface P values indicate statistically significant between-group differences (P < .05).
Overall, the mean autograft diameter was 8.4 ± 0.8 mm, and femoral fixation was achieved with 15-mm loop length cortical buttons in 219 patients (87.9%). The location of the suspensory cortical button in the sagittal plane was posterior in 79.1% of patients, and the femoral tunnel angle in the coronal plane was 39.6° ± 6.2° on postoperative day 1. At 12-month follow-up, the mean femoral tunnel widening was 2.6 ± 2.0 mm, while the mean tibial tunnel widening was 3.1 ± 2.3 mm. Aside from the significant difference in distance from the cortical button to the LFC between groups 1 and 2 (P < .01) and between groups M and non-M (P = .03), there were no significant differences between the soft tissue interposition groups or the cortical button migration groups (Table 3).
Graft Diameter, Cortical Button Location, and Radiographic Measurements a

a Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant between-group differences (P < .05). LFC, lateral femoral condyle; postop, postoperative.
In group 2, the mean distance between the suspensory cortical button and the LFC (ie, the soft tissue interposition) was 2.4 ± 3.3 mm on postoperative day 1 radiographs (Table 3). A comparison of the 1-day versus 12-month postoperative radiographs in group M revealed that the suspensory cortical button had migrated 4.1 ± 1.7 mm in the coronal plane and had rotated 3.1° ± 23.6° in the sagittal plane. The results of our cutoff analysis indicated that if this distance was >1.8 mm at 12 months postoperatively, then it was considered as a risk factor for greater suspensory cortical button migration (sensitivity = 56.25%; specificity = 81.82%; area under the receiver operating characteristic curve = 0.7102 (95% CI, 0.53995-0.88051).
Postoperatively, ACL rerupture was detected in 10 (4.0%) of the patients included in our study. These patients were not included in the comparison of outcomes among the groups. For all patients, there was a statistically significant improvement in the pre- to postoperative Tegner (from 4.1 to 4.3; P = .044) and Lysholm (from 44.0 to 89.2; P = .012) scores, with no statistically significant difference in improvement between groups 1 and 2 or between groups M and non-M. The postoperative laxity evaluation demonstrated that 83.7% of the patients had normal anterior knee laxity (<3 mm), and no statistically significant difference in laxity was found between groups 1 and 2 or between groups M and non-M. When evaluating the 12-month postoperative MRI scans, Howell grade 1 ligamentization was observed in 54.0%, and grade 2 ligamentization was observed in 45.6% of the patients. There was no significant difference between groups 1 and 2 or between groups M and non-M in terms of ligamentization (Table 4).
Patient-Reported and Clinical Outcomes and Autograft Ligamentization a

a Data are reported as mean ± SD or n (%). Dashes indicate percentages. Preop, preoperative; Postop, postoperative.
b Excluding 10 patients with reruptures.
Discussion
The current study demonstrated that, in patients undergoing single-bundle ACLR with hamstring autograft, there were no differences in clinical outcomes or 12-month postoperative ligamentization in either the soft tissue interposition groups (groups 1 and 2) or the suspensory cortical button migration groups (groups M and non-M). These findings are in parallel with the hypothesis of our study. Upon review, we could not find any study in the literature investigating the effects of soft tissue interposition and suspensory cortical button migration on postoperative graft ligamentization assessed on MRI scans.
Soft tissue interposition between the suspensory cortical button and the LFC is a complication with a reported prevalence of 25.2% after ACLR. 12 Gürpınar et al 8 reported that >2 mm of soft tissue interposition may lead to poor postoperative functional results and is a risk factor for postoperative suspensory cortical button migration. 8 However, other studies have reported that this complication has no effect on postoperative clinical and functional outcomes. 12,19 Even though an average soft tissue interposition of 2.4 mm was observed in group 2 patients, satisfactory clinical, functional, and radiological results were obtained in our study.
Some researchers have suggested the use of intraoperative fluoroscopy to confirm the proper placement of the button in surgeries where femoral fixation is performed using a suspensory cortical button. 4,15 Gunaydin et al 7 reported that the placement of the suspensory cortical button in the sagittal plane had no effect on postoperative functional outcomes. Chung et al 6 reported that, in ACLRs performed with the transportal technique, the exit site of the femoral tunnel from the LFC tends to be located more distally, that is, with a higher femoral tunnel angle. Uchida et al 21 reported that posteriorly and distally placed suspensory cortical buttons have a higher risk of migration; however, this migration had no effect on postoperative functional outcomes. In our study, no significant difference was found between the soft tissue interposition groups or the cortical button migration groups in terms of the femoral tunnel angle or the location of the suspensory cortical button in the sagittal plane.
Meniscal and cartilage pathologies may accompany ACL ruptures. Ramp lesions and posterior root ruptures of the lateral meniscus, which can accompany ACL ruptures, increase rotatory laxity. 1,14 It has been reported that performing meniscal surgery together with ACLR does not have a significantly negative effect on postoperative clinical and functional outcomes. 5 It has also been reported that cartilage-related surgeries performed together with ACLR do not have a significant effect on postoperative clinical and functional outcomes, but a lesion size >2 cm2 may lead to unsatisfactory results. 18 In our study, there was no significant difference among the soft tissue interposition groups or the cortical button migration groups in terms of meniscal and cartilage pathologies. The methods used in the treatment of lateral meniscal and cartilage pathologies showed significant differences; however, the sample sizes of these groups were small. There were no further significant differences observed in treatment of other pathologies of all treated patients.
MRI is used as a noninvasive method that provides excellent information about the biological status of the graft using its signal intensity. 16 In the evaluation of graft ligamentization in our study, grafts demonstrated Howell grade 1 ligamentization (equal hypointensity with the posterior cruciate ligament and the patellar tendon) in 54.0% of the patients. Stöckle et al 20 reported that, after ACLR, revascularization could be completed at 18 months postoperatively, and after this period all grafts could exhibit hypointense characteristics. In our study, Howell grade 2 ligamentization was detected in only 45.6% of the patients at 12-month follow-up, which may be owing to MRI evaluation before the full ligamentization process.
Limitations
There were several limitations to this study. First, our study was retrospective. Second, our sample size was small. Third, the distances of the button from the lateral condyle were relatively small. The small sample of patients with interposition may result in our study’s being underpowered for some of our analyses. Fourth, even though the performance of all surgeries by a single surgeon provides homogeneous groups, having all the clinical and functional results belonging to a single surgeon may be considered a limitation. Another limitation was that the patient-reported outcomes and functional outcomes were recorded at a different time than the radiographic measurements. In the routine practice of our clinic, patients undergo MRI scans 1 year after ACLR. To be synchronous with the MRI findings and because the literature has reported that there is no significant suspensory cortical button migration before 12 months postoperatively, 8,12 we evaluated radiographs at the 12-month follow-up. Finally, in assessing ligamentization on the MRI scans, we used the Howell grading system instead of the frequently used signal-to-noise quotient, since patients had their postoperative MRI scans taken at different centers and the magnet strength of each MRI scan was different (1.5 T to 3.0 T). 16
Conclusion
In the current study, differences in soft tissue interposition and suspensory cortical button migration did not significantly affect postoperative clinical or functional outcomes or graft ligamentization after single-bundle ACLR.
Footnotes
Final revision submitted May 9, 2022; accepted June 14, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ankara University (ref No. I8-491-20).