
Abstract
Background:
Femoral cortical button suspension fixation is a popular and reliable technique for posterior cruciate ligament reconstruction (PCLR). Button malposition during graft fixation can lead to postoperative graft loosening.
Purpose:
To determine the risk factors of femoral cortical button malposition in PCLR when neither direct visualization nor intraoperative fluoroscopy is used.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Of the 206 consecutive patients who underwent PCLR without direct visualization or intraoperative radiographs in 2019 at a single institution, 182 met the selection criteria and were included in the study. The distance from the suspension button to the femoral cortex was measured on postoperative computed tomography scans. The button was considered malpositioned if its distance to the femoral cortex was ≥2 mm. We evaluated patient-related and surgery-related variables, including age, sex, concomitant ligament reconstruction, button type, and surgeon experience. Multivariate logistic regression was conducted to evaluate the risk factors for button malposition.
Results:
The overall prevalence of button malposition was approximately 17.0% (31/182), and the mean distance from the button to the femoral cortex was 6.11 ± 5.82 mm in the malposition group. Male sex was the most significant risk factor for button malposition (odds ratio [OR], 13.86; 95% confidence interval [CI], 1.73-111.17; P = .013). Other independent risk factors were low surgical volume (completing ≤3 procedures; OR, 6.41; 95% CI, 1.89-21.72; P = .003), concomitant ligament reconstruction (OR, 5.56; 95% CI, 2.12-14.58; P < .001), and fixed-loop button (OR, 3.96; 95% CI, 1.11-14.18; P = .034).
Conclusion:
Male sex, low surgical volume, concomitant ligament reconstruction, and fixed-loop button were independent risk factors for femoral cortical button malposition during PCLR.
Keywords
Posterior cruciate ligament reconstruction (PCLR) has been continually evolving. As a result of advances in arthroscopic techniques and instruments, there are multiple options for femoral-side graft fixation in PCLR, one of which uses a femoral cortical button. The cortical button sits on the outer cortex of the femur, allowing the graft to be suspended through a retrograde-drilled tunnel. It is widely accepted because it has demonstrated satisfactory biomechanical properties both in anterior cruciate ligament reconstruction (ACLR) 6,12,14 and PCLR 3,13 surgeries. In addition, the use of suspensory devices can offer help on the length of the graft in PCLR.
However, some studies have reported several technical errors with this type of graft fixation, such as button malposition, flipping failure, jamming in the femoral guide pin hole, and being pulled to the outside of the skin or into the joint, 9,19 which would subsequently result in postoperative graft loosening and failure of reconstruction. In past clinical practice, we have noticed a phenomenon that the cortical button was not seated at the proper position on the femoral cortex, which was similar to that reported in ACLR called “button malposition.” The prevalence of button malposition in ACLR has been reported as approximately 15% to 25.2%, 7,17 but no studies have reported the prevalence of button malposition in PCLR. Because the basic graft fixation techniques of PCLR are the same as those of ACLR, similar technical errors can also occur in PCLR when inadequately recognized.
In this study, we retrospectively assessed cortex button positioning and its congruence with the femoral cortex using computed tomography (CT) scans in patients who underwent PCLR with femoral-sided cortical suspensory fixation devices. The purpose of the study was to identify the prevalence and risk factors of femoral cortical button malposition in PCLR. We hypothesized that the prevalence would not be lower than that reported in previous ACLR reports, and patient characteristics and surgeon experience would affect the prevalence of button malposition.
Methods
Study Design and Patient Selection
Appropriate institutional review board approval was obtained for the study protocol. We retrospectively evaluated consecutive patients who underwent unilateral single-bundle PCLR from January 1, 2019, to December 31, 2019, at our institution. Patient and surgical data were extracted from the electronic medical records and included age, sex, operation side, concomitant ligament reconstruction, cortical button type, and surgeon. The study inclusion criteria were as follows: primary single-bundle PCLR (isolated or multiligamentous procedure), femoral tunnel drilling using inside-out techniques, and graft fixation with a femoral cortical button. Exclusion criteria were as follows: revision PCLR, double-bundle PCLR, use of different types of femoral fixation from the cortical button, other femoral socket related technical errors occurring during operation (eg, the femoral cortical button remained within the bone tunnel), direct visualization or intraoperative radiographs were used during operation, and lack of appropriate postoperative CT scan to check the button position.
Surgical Technique
After spinal anesthesia was performed, the patient was placed in a supine position, and the tourniquet was applied at the proximal thigh and inflated before the incision.
First, a standard arthroscopic examination was performed using standard anteromedial (AM) and anterolateral (AL) portals. Any associated pathology related to the meniscus or cartilage was treated. Remnants of the posterior cruciate ligament (PCL) were retained whenever possible. Grafts were harvested and prepared as a 4-stranded double-looped autograft with a minimum length of 90 mm. The femoral end was looped over an adjustable-loop (TightRope; Arthrex) or fixed-loop cortical button (EndoButton; Smith & Nephew Endoscopy) according to the surgeon’s preference.
The tibial tunnel was created under direct visualization with the arthroscopy in the posteromedial portal. The femoral tunnel was created using an inside-out technique through an accessory AL portal. The femoral side of the graft was deployed first. Then, the arthroscopy was transferred to the AM portal, and the prepared graft was passed through the accessory AL portal into the femoral tunnel from the proximal femora under arthroscopic visualization. Shuttling the implant into the tunnel and flipping the button were performed by a surgeon assistant. When a fixed-loop button was used, the marked length at the femoral end of the graft acted as a second check before the button was flipped. When an adjustable-loop button was used, once the button was engaged into the lateral cortex of the femur, the tensioning suture was pulled to advance the graft into the femoral tunnel. Thereafter, the tibial end of the graft was passed into the tibial tunnel with the aid of the tibial looped passing suture. With the graft under maximum tension and the patient’s knee in 90° of flexion, the graft was fixed on the tibial side with an interference screw that was oversized by 1 mm to the tibial tunnel diameter. Additional suspensory fixation might be used, depending on bone quality and the surgeon’s preference. Concomitant ligament reconstructions using conventional methods were subsequently performed as required.
CT Measurement
CT scans are performed routinely at our institution after PCL reconstruction. The scans are used to verify the position of the bone tunnels and the stability of the internal fixation, which helped to guide the progress of rehabilitation training. All CT examinations for the study patients were performed using a GE Discovery CT750 HD scanner (GE Medical Systems). The slice thickness was set at 5 mm. The senior authors (G.X., X.X., and W.J.) agreed on the measurement methods. The shortest distance from the inferior surface of the cortical button to the medial femoral cortex was measured on the axial sequences of CT (Figure 1). Two authors were trained to unify measurement methods and measure independently, and the average of the 2 measurements was used in the analysis (Z.Y. and M.Y.). In consensus with other studies, 1,17 the button was considered malpositioned if the distance from the inferior surface of the cortical button to the medial femoral cortex was longer than 2 mm (Figure 2). Data were recorded with an accuracy of 0.01 mm using specialized software (Centricity Enterprise Web Version 3.0; GE Medical Systems).
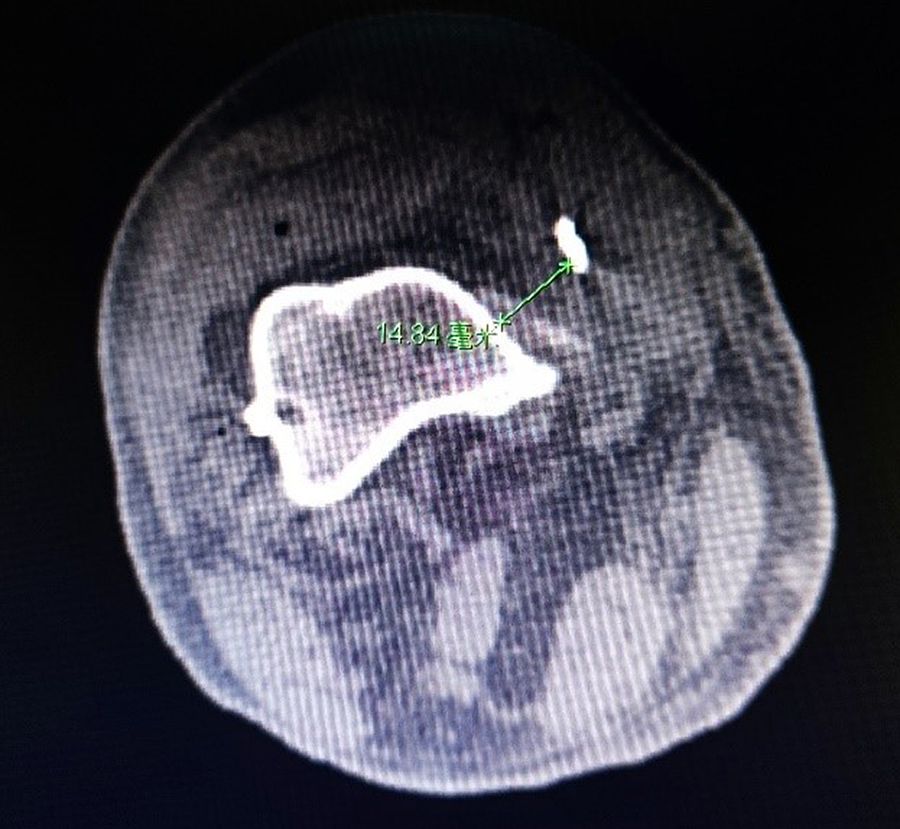
Measuring the shortest distance from the inferior surface of the cortical button to the medial femoral cortex (green line) on axial CT sequence. CT, computed tomography.
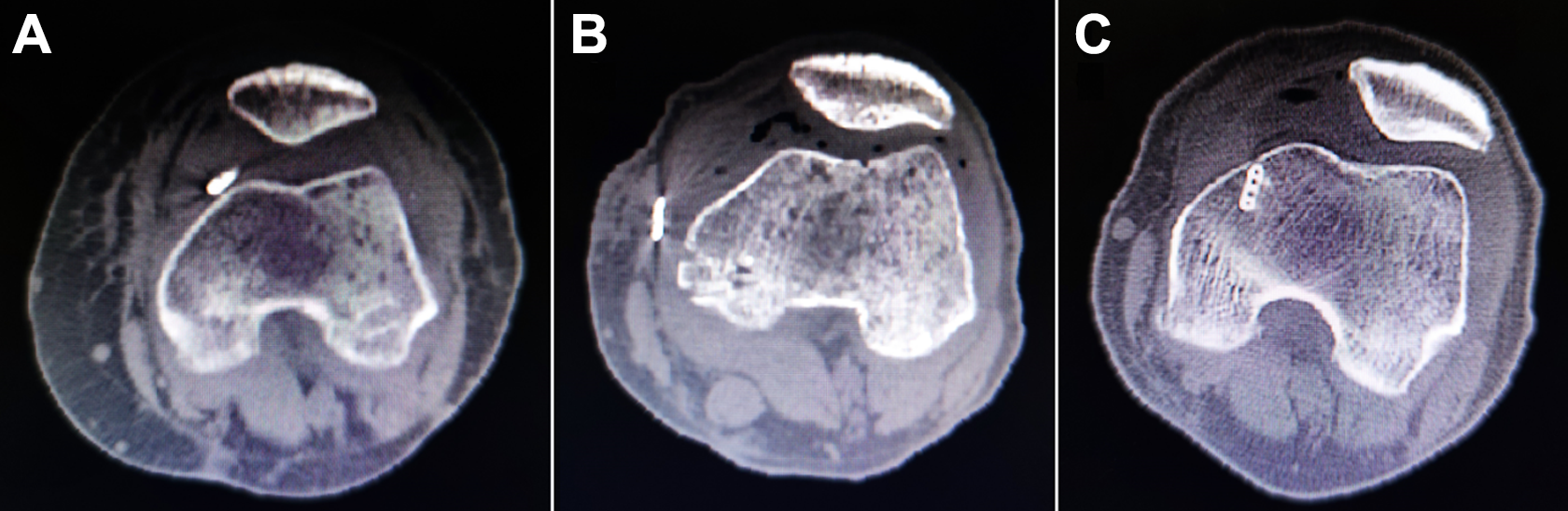
Femoral cortical button positions as shown on axial CT sequence. (A) A button was considered correctly positioned when the entirety of the button was completely in contact with the femoral cortex or the distance from the inferior surface of the cortical button to the medial femoral cortex was <2 mm. (B) A button was considered malpositioned if the distance from the inferior surface of the cortical button to the medial femoral cortex was ≥2 mm. (C) A button beneath the femoral cortex was excluded from the analysis. CT, computed tomography.
Statistical Analysis
All statistical analyses were performed with Microsoft Excel Version 2016 (Microsoft) and SPSS Version 25.0 software (IBM). Variables include age and the distance from the button to the femoral cortex, expressed as mean ± SD according to their distribution. Surgeon experience was analyzed as a categorical variable according to number of PCLR procedures completed during the study period: low surgical volume (≤3 PCLR procedures; approximately 40% of surgeons), medium volume (4 to <10 procedures; 40% of surgeons), and high volume (≥10 procedures; 20% of surgeons) (Table 1).
Surgeon Experience According to Number of PCLR Procedures Undertaken in 2019 a

a PCLR, posterior cruciate ligament reconstruction.
The relationships of button malposition with the continuous covariates of age and distance from the button to the femoral cortex were analyzed using t tests. Pearson chi-square tests were conducted to examine the relationship of button malposition with the categorical covariates of the male sex, right side, concomitant ligament reconstruction, fixed-loop button, and surgeon groups. Fisher exact tests were conducted when cell frequencies were <5. A multivariable binomial logistic regression analysis was then performed to examine the independent effect. Odds ratio (ORs), 95% confidence interval (CIs), and P values were calculated for all variables. P < .05 was considered statistically significant for all statistical tests.
Results
A total of 206 consecutive patients who underwent PCLR without direct visualization or intraoperative radiographs were included for review. Of these, 18 patients had missing CT scans, and 6 additional patients failed to meet the inclusion criteria (2 patients had undergone revision PCLR, a suspension device for femoral-side graft fixation was not used in 1 patient, the button type could not be determined in 1 patient, and the femoral buttons remained within the bone tunnel and were beneath the femoral cortex in 2 patients). Overall, 182 patients (135 men and 47 women; 84 right knees and 98 left knees) with a mean age of 33.8 ± 14.3 years met the selection criteria and were included in the analysis.
The patient and surgery characteristics are listed in Table 2. Of the 182 patients, 133 (73.1%) received an isolated PCLR, and 49 (26.9%) had concomitant ligament reconstructions (Table 3). The prevalence of button malposition was approximately 17.0% (n = 31), and the mean distance from the button to the femoral cortex was 6.11 ± 5.82 mm in the malposition group, compared with 0.11 ± 0.34 mm in the correct position group (n = 151).
Characteristics of the Study Patients (N = 182) a
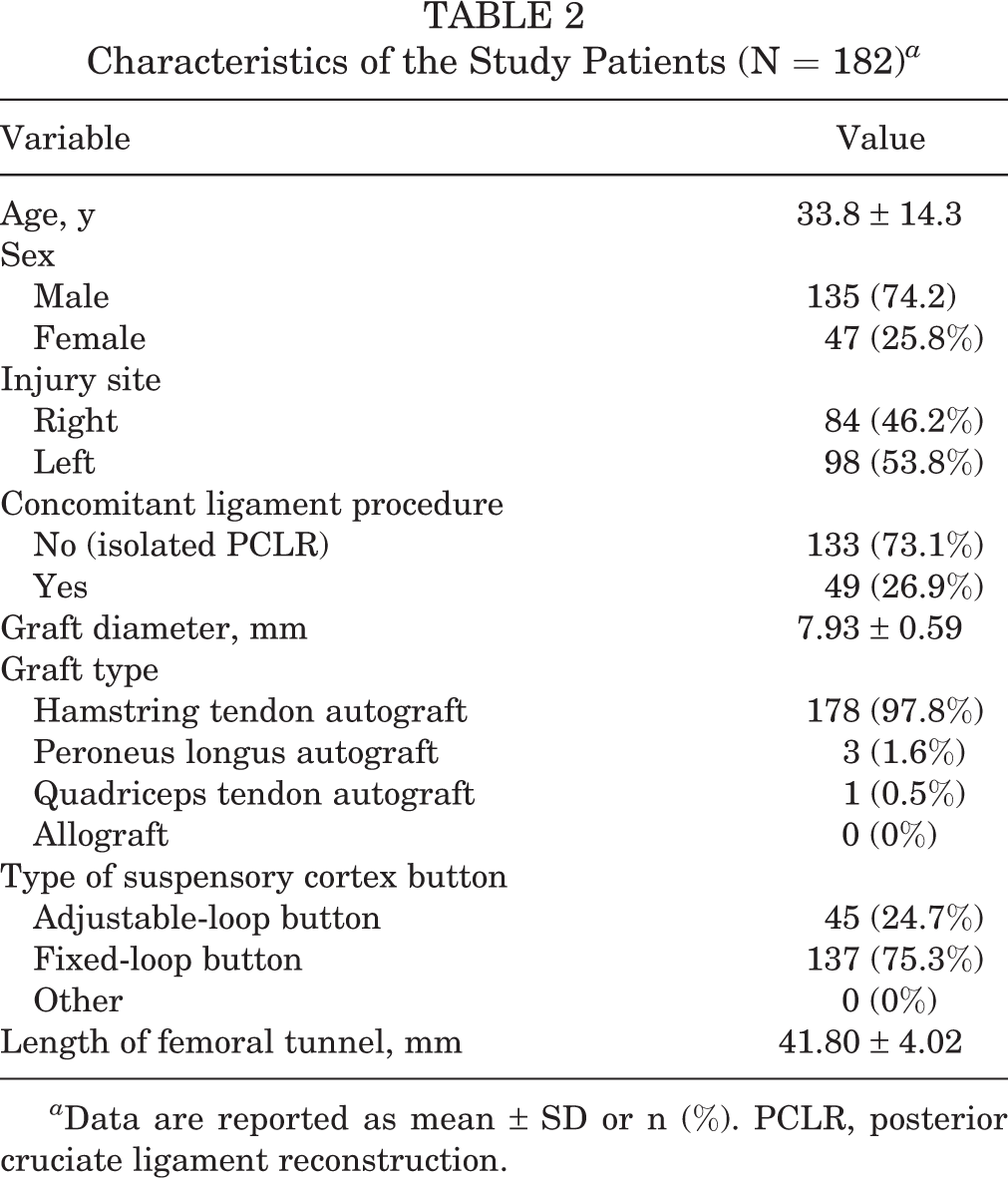
a Data are reported as mean ± SD or n (%). PCLR, posterior cruciate ligament reconstruction.
Concomitant Ligament Reconstructions Performed at the Time of PCLR a

a ACL, anterior cruciate ligament; MCL, medial collateral ligament; MPFL, medial patella-femoral ligament; PCLR, posterior cruciate ligament reconstruction; PLC, posterior lateral corner.
Factors associated with button malposition are summarized in Table 4. The prevalence of button malposition in the fixed-loop button group was not significantly higher than that in the adjustable-loop button group (19.7% vs 8.9%; P = .112). However, we still analyzed the fixed-loop button in our logistic regression because of the high rate of malposition (19.7%). Overall, 4 potential risk factors were identified: patient sex, distance from button to femoral cortex, concomitant ligament surgery, and surgeon experience.
Patient- and Surgery-related Factors Compared Between the Correct Position and Malposition Groups a

a Bold P values indicate a statistically significant difference between the correct position and malposition groups (P < .05). PCLR, posterior cruciate ligament reconstruction.
bt test.
c Fisher exact test.
d Pearson chi-square test.
e Low volume, ≤3 PCLR procedures/year; medium volume, 4 to <10 procedures/year; high volume, ≥10 procedures/year.
Multivariate logistic regression was conducted to evaluate the risk factors for button malposition. Male sex was the most significant risk factor for button malposition (OR, 13.86; 95% CI, 1.73-111.17; P = .013). Other independent risk factors were concomitant ligament reconstruction (OR, 5.56; 95% CI, 2.12-14.58; P < .001), fixed-loop button (OR, 3.96; 95% CI, 1.11-14.18; P = .034), and low-volume surgeon (OR, 6.41; 95% CI, 1.89-21.72; P = .003) (Table 5).
Risk Factors for Button Malposition in PCLR a
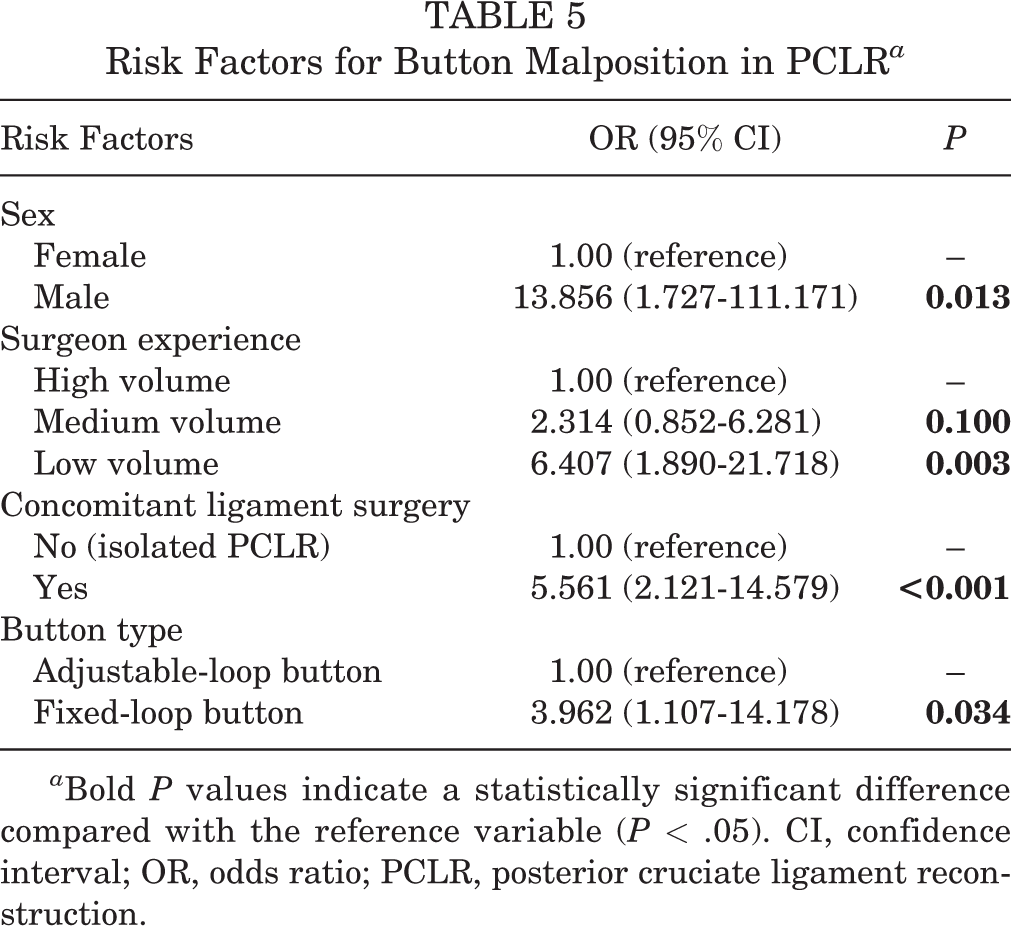
a Bold P values indicate a statistically significant difference compared with the reference variable (P < .05). CI, confidence interval; OR, odds ratio; PCLR, posterior cruciate ligament reconstruction.
Discussion
Arthroscopic PCLR is a more technically demanding technique than is ACLR. Technical errors during reconstruction, such as inadequate fixation or improper graft tension, can lead to persistent posterior laxity, which is the most common complication following PCLR. 20 Currently, no studies have reported the prevalence of femoral cortical button malposition in PCLR. In this study, we conducted a retrospective review of postoperative knee CT scans of 182 patients. The prevalence of button malposition in the present study was approximately 17.0%. This result is consistent with our hypothesis and similar to that in ACLR surgeries, which have been reported as approximately 15% to 25.2%. 7,17
A cortical button that is not sitting in a congruent manner on the femoral cortex indicates that there is interposition of soft tissue between the femur and button. Technique notes reported that the button could be pulled out through the skin laterally or it might flip within the substance of the vastus medialis. In this study, the button was fixed more than 2 mm from the femoral cortex in 31 (17.0%) patients. Furthermore, in 4 patients, the buttons had deviated more than 10 mm from the femoral cortex.
Another technical error is that the button might be stuck in the lateral opening of the guide pin hole, giving the false impression that it has flipped and engaged on the lateral femoral cortex. These misplacements are often not noted until postoperative radiographs are performed. There were 2 patients in this study in whom the buttons were jammed in the femoral guide pin hole in the region of the cortical bone bridge. As the focus of this study was to investigate the risk factors for a femoral button far away from the bone surface, the 2 patients failed to meet the inclusion criteria of this study and were excluded from the analysis.
Furthermore, the study revealed that male sex was an independent risk factor for femoral cortex button malposition in PCLR. The risk of button malposition in the male group was 13.86 times higher than that in the female group (P = .013). A rational explanation for this is that a larger vastus medialis muscle volume may lead to more soft tissue interposed between the femoral cortex and the button. It has been reported that maximal muscle power in jumping and sprinting are positively correlated with lower limb muscle volume, especially the vastus medialis muscle. 2 In general, muscle thickness in the distal medial femoris is larger in men than in women. 5
There was significant difference in the rate of button malposition according to the surgeon experience group (40.9% for low-volume vs 18.1% for medium-volume vs 10.2% for high-volume surgeons; P = .003). On multivariate logistic regression analysis, the risk of button malposition in the low-volume group was 6.41 times higher than that in the high-volume group (P = .003). The finding suggests that a steep learning curve also exists for proper button deployment in PCLR. It has been reported that an experienced surgeon requires at least 10 ACLR cases to attain an improved tunnel placement when converting from a single-bundle to a double-bundle technique with relative accuracy. 15 We found similar results for PCLR. The risk of button malposition in PCLR may be higher for novice surgeons, especially at the beginning of their learning curve. We recommend the use of intraoperative radiographs or arthroscopic direct visualization during the learning phase for effective button deployment to perform accurate and reproducible PCLR.
In general, concomitant ligament reconstructions could increase operative difficulty and split the focus of surgeons, which may lead to a high prevalence of technical errors. In this study, 49 (26.9%) patients had concomitant ligament reconstructions performed at the time of PCLR. A higher prevalence of button malposition was found in the concomitant ligament reconstruction group than that in the nonconcomitant ligament reconstruction group (30.6% vs 12.0%; P = .003). Medial collateral ligament rupture and patellar dislocation would disturb the normal structure of the medial distal femur. Local bleeding and scarring at the injury site could thicken the fascia of the medial distal femur. These factors could lead to more soft tissue interposed between the femoral cortex and the button.
It is easier to explain in theory why the fixed-loop button could result in a higher prevalence of button malposition than the adjustable-loop button, although no statistical significance was reached (19.7% vs 8.9%; P = .112). One of the explanations is that the adjustable-loop button is generally shorter than the fixed-loop button, making the adjustable-loop button less likely to compress the surrounding soft tissue. Another explanation is that the adjustable-loop button is a fixation device for suspensory fixation, which, instead of having a loop of fixed length, provides an adjustable loop along with passing sutures that can be retrieved through the skin. This adjustable configuration allows the graft to be tensioned to reach a strong femoral-side graft fixation. After femoral-side and tibial-side graft fixation, the surgeon can pull the sutures again to tighten the entire length of graft in the joint. If soft tissue is interposed, the distance between the cortical button and the medial femoral cortex may decrease during tensioning. Despite there being no significant difference when analyzed by the Pearson chi-square test, multivariate logistic regression analysis revealed that the risk of button malposition in the fixed-loop button group was 3.96 times higher than that in the adjustable-loop button group (P = .034).
Several techniques helping to ensure proper positioning during ACLR have been reported in the literature. Some surgeons recommend the use of intraoperative fluoroscopy to avoid button malposition and assess its relation to the femoral cortex. 1,18 Other surgeons propose the use of a guide pin to provide a controlled force for a more accurate passage of the button through the femoral guide pin hole 9 or the use of a femoral guide pin incision on the lateral aspect of the femur as an endoscopic portal for direct visualization of the cortical button. 10 Arthroscopic direct visualization of the button deployment is a more effective method. Several studies have reported that the proper position was achieved through an arthroscopic view of the lateral gutter of the knee or an iliotibial band portal 4,8,11,16 in ACLR. It was reported that the femoral button placed with direct visualization was more likely to have an optimal position directly on the femoral cortex compared with indirect methods (0% vs 8.8%; P = .046). 4
Prior to this study, we did not realize that the prevalence of button malposition was so high, which was 17.0% on average. So far, no other studies in the literature have reported this issue. Before this analysis, we did not routinely check the position of femoral cortical buttons during the operation, but after this retrospective study, we have begun to pay attention to and set out to solve this problem. Direct visualization and intraoperative radiographs are now routinely used during operation to check the proper position of the femoral cortical button. We have also begun to study the relationship between button malposition and the function of the knee joint.
Limitations
There are a few limitations to the present study. First, it was a retrospective study. Analysis was performed using only electronic medical records. There are no follow-up results and no control group. In addition, no postoperative laxity measurements or patient-reported outcomes are reported. Thus, no clinical significance to the malposition can be assessed. Second, the distance between the button and the femoral cortex was only measured on the axial sequences of CT scan; a 5-mm thickness of CT slices was used when the threshold for considering malposition was 2 mm. These may be subject to potential method bias. Third, the body mass index and thigh circumference were not included in the study, although they could be risk factors. Fourth, further study is warranted to determine the effect that cortical button malposition has on the laxity and strength of PCL graft fixation.
Conclusion
PCLR using a suspension device for femoral-side graft fixation may lead to a high risk of femoral cortical button malposition. Male sex, low-volume surgeons completing ≤3 procedures per year, concomitant ligament reconstructions, and a fixed-loop button are independent risk factors. We encourage authors to confirm button position intraoperatively with radiographs or direct arthroscopic visualization. Further high-quality prospective studies are required.
Footnotes
Final revision submitted February 8, 2022; accepted February 23, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Education Department of Hunan Province (No.20C1144). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital.