
Abstract
Background:
The New Zealand Rotator Cuff Registry represents the largest prospective cohort of rotator cuff repairs. Despite this, there are limited medium- to long-term data of rotator cuff repair outcomes.
Purpose:
To (1) analyze the pain and functional outcomes of a large cohort of primary rotator cuff repairs and (2) evaluate the effect of patient factors and tear characteristics on medium-term outcomes.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
This was a multicenter, multisurgeon prospective cohort study of rotator cuff repairs from March 2009 until December 2010. Surgical data were collected by the operating surgeon. Primary outcome measures were the Flexilevel Scale of Shoulder Function (FLEX-SF) and a pain score, collected at baseline, 6, 12, and 24 months, and 5 years. Univariate and multivariate analyses were carried out.
Results:
Overall, 2533 primary rotator cuff repairs were analyzed with 81% follow-up at 5 years. The mean age of the cohort was 56 years. In the 2052 patients with final follow-up data, improvement on the FLEX-SF continued until 24 months postoperatively and remained high at 5 years. Mean improvement in FLEX-SF from baseline to 5 years was 15 points. Patients aged >70 years had lower FLEX-SF scores but no significant difference in improvement compared with patients ≤70 years. The mean anteroposterior tear size was 2.2 cm, and on multivariate analysis, tears >4 cm had worse 5-year FLEX-SF scores. If the affected tendon was easily reducible, there was no difference in FLEX-SF score for retracted or larger tears compared with smaller tears. The reoperation rate was 6.2%.
Conclusion:
Results indicated that rotator cuff repairs provide a sustained clinical improvement out past 5 years. Most functional improvement and pain relief occurred within the first 6 months, but improvement continued out to 24 months. Most population groups did well after rotator cuff repairs, including those >70 years. Tear size >4 cm and tendon reducibility correlated with outcome. Even patients with large tear sizes had clinically significant improvement in FLEX-SF scores after repair.
Rotator cuff disease is a leading cause of shoulder pain and dysfunction, accounting for up to 70% of shoulder presentations to primary care. 20 Rates of rotator cuff repair, indicated for those who have failed nonoperative treatment, have steadily increased in most parts of the world. 7,17
Despite this rise, there is limited research with medium- to long-term follow-up after rotator cuff repair surgery. Chalmers et al 2 recently published a systematic review of rotator cuff repair outcomes, with combined results from 32 studies totaling only 1294 repairs. Collin et al 6 analyzed 511 rotator cuff repairs from across 15 centers in Europe. Follow-up was out to 10 years but with more of a focus on radiological outcome.
Understanding the effect of patient variables on outcomes after rotator cuff repair will aid in counseling patients and their expectations. The effect of age on rotator cuff repair radiological outcome has been reported extensively, with older age linked to poorer radiological outcomes, 4,9,19,22,26 although clinical outcome in older patients may differ from radiological outcomes. 21 Female sex and high-demand occupations have also been linked to poorer outcomes after rotator cuff repair. 3,13,15
Tear characteristics are linked to outcomes post–rotator cuff repair. Significant parts of the literature have focused on tear size and the effect on outcome. 4,14 Tendon retraction has been shown to be an independent risk for rotator cuff failure. 13 Tendon reducibility and tension of repair is also linked to outcome. 15 Fatty degeneration in the rotator cuff muscle preoperatively is linked to poorer clinical outcomes after surgery. 16
The New Zealand Rotator Cuff Registry was designed to assess medium-term outcomes of a large group of rotator cuff repairs from multiple centers across New Zealand. The registry design allows collection of data over time from normal everyday practice, minimizing intervention bias. 11
The aim of the current study was to (1) analyze the medium-term pain and functional outcomes in patients from the New Zealand Rotator Cuff Registry and (2) evaluate the effect of certain demographic and tear characteristics on medium-term outcomes. We hypothesized that rotator cuff repairs would continue to improve clinically out to 5 years and that tear characteristics (size, amount of retraction, reducibility) would influence outcomes.
Methods
Participants
The New Zealand Rotator Cuff Registry is a prospective multicenter study of rotator cuff operations undertaken in New Zealand from March 1, 2009, until December 31, 2010. Surgeons from the New Zealand Shoulder and Elbow Society were informed of the study, invited to participate, and then educated about the study protocols: A total of 90 surgeons from across the country participated. Recruitment of patients to the cohort was undertaken by the operating surgeon as per a surgical registry design. Approval for this study was gained from a regional ethics committee.
Included were patients who were undergoing primary rotator cuff repair as part of the surgical procedure. Open, miniopen, and arthroscopic repairs were included as well as concurrent shoulder procedures. Revision repairs were excluded from this current study. Patients with cognitive impairment or who died during the study time frame were also excluded from the study. Cognitive impairment was defined by the researcher if the patient was unable to recall sufficient details or the family informed the researcher of a diagnosis of dementia. A total of 2533 patients were initially enrolled. Figure 1 describes the numbers of included and excluded patients.

Flowchart of included and excluded patients.
Outcome Measures
Once enrolled, follow-up was taken over by the research team. At enrollment, patients completed a baseline demographic questionnaire that included age, sex, ethnicity (European, Maori, Pacific Islander, or Asian), and occupation type (high demand or low demand). Preoperative pain and functional scores were collected at baseline. The pain score was a 1 to 10 scale quantifying mean pain levels over the preceding month, with a lower score representing less pain. The Flexilevel Scale of Shoulder Function (FLEX-SF) was the chosen functional score. The FLEX-SF score has been validated against other shoulder functional instruments. 8,24,25 The set of shoulder-specific questions generates a FLEX-SF score from 1 to 50, with higher scores representing better function.
Intraoperative data were collected by the primary operating surgeon. This included intraoperative tear findings, presence of concurrent surgical pathology, and surgical techniques. Tear size and tear retraction were measured by the surgeon. Tendon reducibility was judged on the ability to reduce the tendon back to the anatomic footprint and was subjectively classified as easy to reduce, requiring releases, unable to fully reduce, or unable to reduce at all.
Outcome data were collected at 6, 12, and 24 months and then at 5 years postoperatively. Forms were mailed to patients for the 6-, 12-, and 24-month scores. For the 5-year follow-up, this was changed to an online method, and this was extended for a total collection period of 18 months. Pain score, FLEX-SF score, and postoperative questionnaire responses were collected. The postoperative questionnaire included secondary outcomes such as complications data, global function, and return to work. Information regarding postoperative complications was collected over 5 years.
Statistical Analysis
Pain and FLEX-SF trends were analyzed over time. Patient and tear characteristics were analyzed. For comparison purposes, patient age was grouped into 5 categories (<50, 50-59, 60-69, 70-79, and >80 years), tear size and tear retraction were each grouped into 5 categories (<1, 1-1.9, 2-2.9, 3-3.9, and >4 cm), and tendon involvement as 1, 2, or 3 tendons. We examined statistical relationships using the independent t test, chi-square test, and analysis of variance, with P < .05 considered statistically significant. Univariate analysis was carried using the Sofa statistics program (Version 1.4.3). Normal distribution was examined using kurtosis, skewness, and histogram analysis. Multivariate analysis was carried out using multiple regression model. The regression model was formed using variables found to be significant on the univariate analysis (P < .05).
Results
Of the initial 2533 patients undergoing primary rotator cuff repairs, minimum 5-year follow-up data were available for 2052 patients (81%). The mean age of the initial cohort was 56 years; 214 patients (8.5%) were >70 years. The indigenous Maori population represented 5.6% of the cohort and Pacific Islanders 1.6% (Table 1). The mean tear size was 2.2 ± 1.2 cm, and mean retraction was 1.8 ± 1.1 cm (Table 2).
Patient Characteristics (N = 2533)

a The ethnicity sample size does not include those patients who recorded “other or “unspecified.”
Tear Characteristics (N = 2533) a
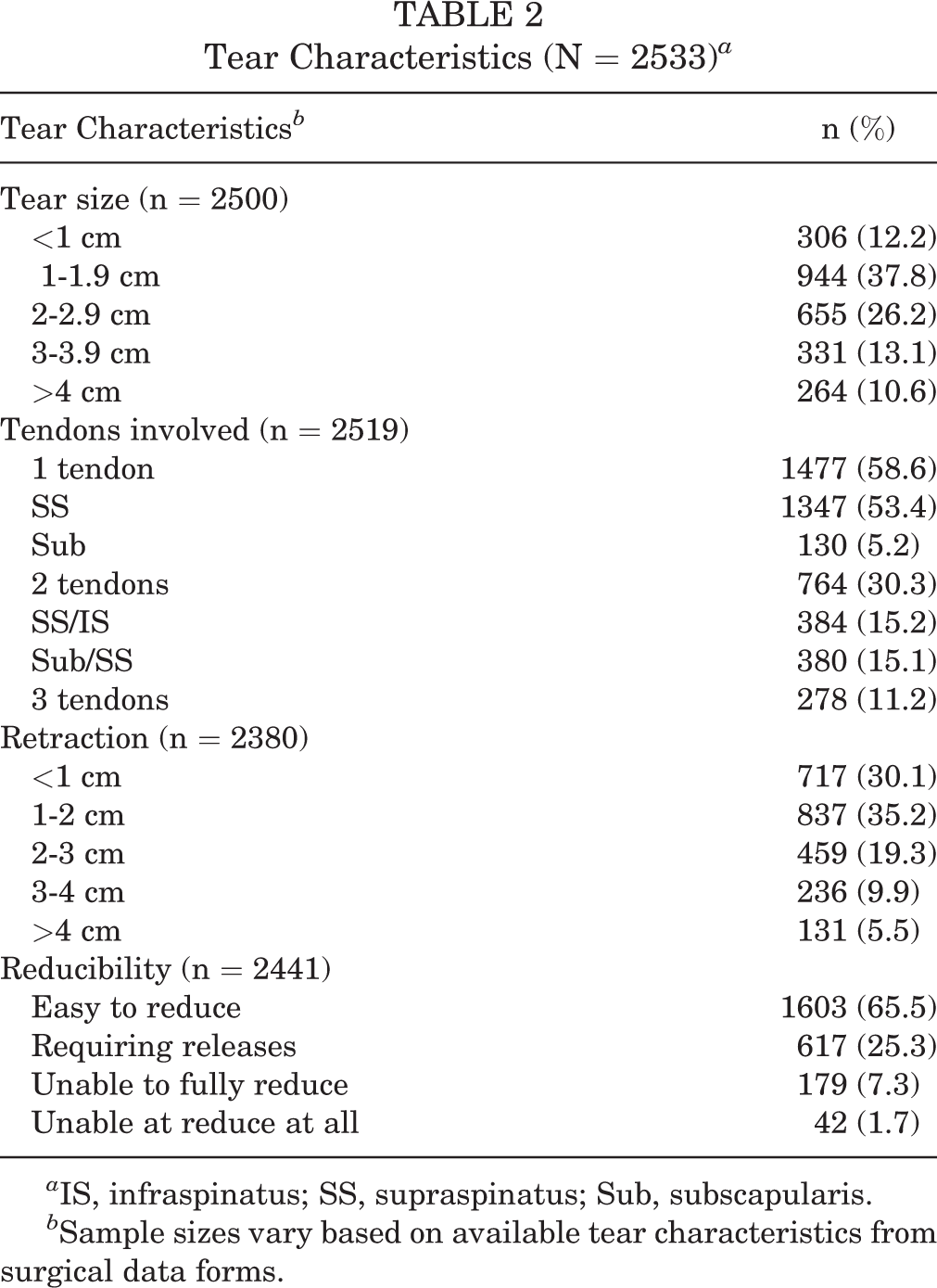
a IS, infraspinatus; SS, supraspinatus; Sub, subscapularis.
b Sample sizes vary based on available tear characteristics from surgical data forms.
Overall Outcome Scores
For the patients with follow-up data (n = 2052), the mean (±SD) improvement in FLEX-SF from baseline to 5-year follow-up was 15 ± 9.8 points. Significant improvement in FLEX-SF score occurred at each time point until 24 months; after this point, scores were maintained past 5 years (Figure 2A). The mean improvement in pain scores was 3.2 ± 1.6 points. Most improvement in pain was in the first 6 months, a small but significant improvement in pain occurred until 12 months postoperatively (Figure 2B).
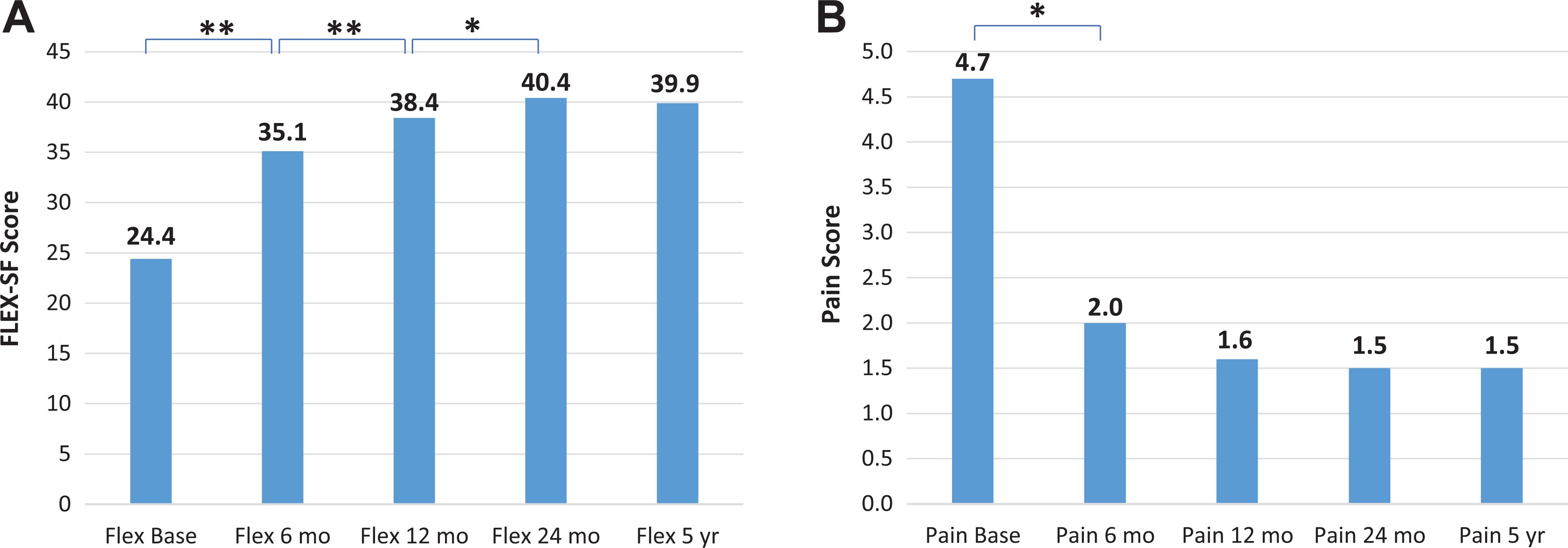
Mean (A) FLEX-SF, Flexilevel Scale of Shoulder Function (FLEX-SF) and (B) pain scores from baseline to final follow-up (n = 2052). Statistically significant difference between groups: *P < .05, **P < .01.
Outcomes According to Patient and Tear Characteristics
Patients aged >70 years had a significantly lower FLEX-SF score compared with those ≤70 years (37.5 vs 40; P < .001), as shown in Figure 3. However, the improvement from baseline was no different between patients aged >70 versus ≤70 years (15.6 vs 15.4; P = 0.29). Tears were more retracted (2.23 vs 1.50 cm; P < .001) and larger in size (2.69 vs 2.18 cm; P < .001) in patients >70 years.

Mean FLEX-SF at 5 years (Flex 5) and improvement from baseline to 5 years in FLEX-SF (Flex Imp), according to age categories (n = 2052). FLEX-SF score is a score of 1 to 50, with higher score indicating better functional outcome. FLEX-SF, FLEX-SF, Flexilevel Scale of Shoulder Function.
Male patients had larger tear sizes (2.33 vs 1.96 cm; P < .001) and more retracted tears (1.85 vs 1.53 cm; P < .001) than did female patients. Patients in high-demand occupations were significantly younger (54 vs 59 years; P < .01) than those in low-demand occupations, and patients in high-demand occupations had better mean 5-year FLEX-SF scores (40.5 vs 39.3, P < .01) and better mean pain scores at 5 years (1.4 vs 1.6; P = .02) (Table 3). There was no difference in FLEX-SF improvement from baseline to 5 years in high- versus low-demand occupations (15.5 vs 15.3; P = .60) (Table 3).
Maori patients had lower FLEX-SF scores at 5 years compared with Europeans (37.1 vs 40.1, respectively; P = .01) (Table 3), but the improvement in scores from baseline was similar to Europeans (14.1 vs 15.6, respectively; P = .3). Pacific Islanders had lower 5-year FLEX-SF scores versus Europeans (34.4 vs 40.1, respectively; P = .02) as well as less improvement in scores (8.7 vs 15.6, respectively; P = .01) (Table 3). There was no difference in tear sizes or retraction between different ethnicities.
FLEX-SF and Pain Scores by Patient Characteristics (n = 2052) a

a Boldface P values indicate statistically significant difference between subgroups (P < .05). FLEX-SF, Flexilevel Scale of Shoulder Function.
bP values for comparison with European ethnicity.
Tears >4 cm had worse 5-year FLEX-SF scores (36.7 vs 40.2; P < .01) and less improvement (13.5 vs 15.7; P = .02). Three tendon tears had a lower mean 5-year FLEX-SF score compared with 1 and 2 tendon tears (37.1 vs 40.1; P < .01) as well as lower FLEX-SF improvement scores (15.7 vs 13.6; P < .01) (Table 4).
FLEX-SF and Pain Scores by Tear Characteristics (n = 2052) a

a Boldface P values indicate statistically significant difference between subgroups (P < .05). FLEX-SF, Flexilevel Scale of Shoulder Function; IS, infraspinatus; SS, supraspinatus; Sub, subscapularis.
bP values for comparison with 1 and 2 tendons.
There were significantly lower mean 5-year FLEX-SF (37.7 vs 40.2; P < .01) and improvement scores (13.1 vs 15.8; P < .01) in those with >3 versus <3 cm retraction. There was no difference in pain levels according to retraction. Overall, 65.5% (n = 1605) of tears were categorized as “easy to reduce.” Easily reduced tendons had higher 5-year FLEX-SF scores compared with other tears (ie, difficult to reduce tears; 40.7 vs 38.4; P < .001). Within the easily reduced tendons, there was no difference in mean FLEX-SF scores in those with minimal (<1 cm) or significant (>4 cm) retraction (40.8 vs 39.8; P = .6).
Multivariate Analysis
On multivariate analysis, age >70 years (P < .05), female sex (P < .01), Maori (P < .05) and Pacific Island ethnicity (P < .01), low-demand occupation (P < .05), tear size >4 cm (P < .05), and difficult-to-reduce tendons (P < .01) were significantly associated with lower 5-year FLEX-SF scores, and Maori ethnicity (P < .01) was associated with higher 5-year pain scores (Table 5).
FLEX-SF and Pain Score 5-Year Univariate and Multivariate Analysis Results a
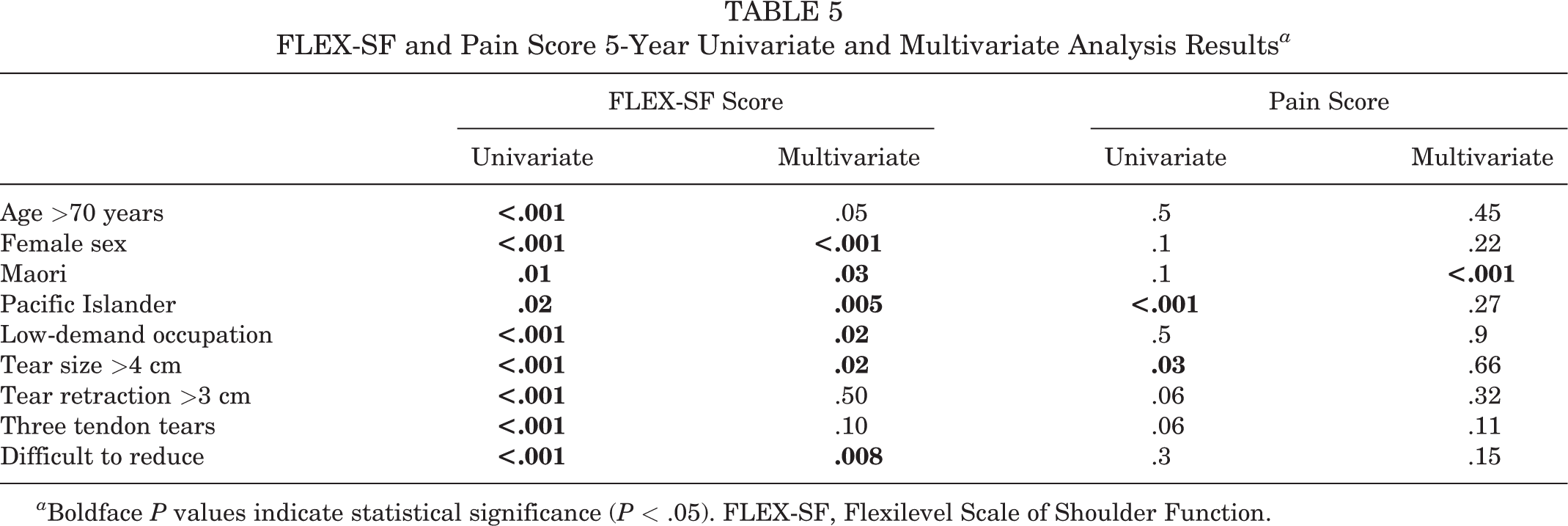
a Boldface P values indicate statistical significance (P < .05). FLEX-SF, Flexilevel Scale of Shoulder Function.
Complications
The overall reoperation rate was 6.2% (146 patients), with 32% for stiffness (46 patients), 27% for retears (40 patients), 7% for infection (10 patients), and 34% other/not specified (50 patients). Retears were reported in 162 patients (7.1%), although this was not confirmed radiologically. In those with retears, the mean FLEX-SF score at 24 months and 5 years was 35.6 ± 9.3 and 32.7 ± 9.4, respectively.
Discussion
In this prospective study of 2533 primary rotator cuff tears with 81% follow-up past 5 years, rotator cuff repair provided a clear benefit to patient function and pain improvement. The mean improvement in functional score of 15 points is higher than the 3-point clinically important difference for FLEX-SF score. 8 The mean improvement in pain score was 3.2 points, with the majority of pain improvement occurring within the first 6 months. Improvements in both pain and functional scores were maintained at the 5-year follow-up. To date, this represents the largest prospective cohort of rotator cuff repairs reported. These findings are useful for patient counseling, and advice can be given that most pain and functional improvement occurs within the first 6 months postsurgery, but further improvement can be seen out to 24 months.
Most patient groups benefited from surgery. The mean age of our cohort was 56 years, but we did report the outcome of 214 repairs in those over 70 years. Traditionally, advancing age has been linked to poorer outcomes post–rotator cuff repair. 19 In our cohort, absolute 5-year functional outcomes were lower in >70 years. However, the improvement compared with baseline was similar to those <70 years, and the retear rates were no different. This mirrors similar findings comparing older age groups with younger age groups, with comparable clinical improvement noted between the 2 groups. 18,21
Other demographic factors also show similar good outcomes with rotator cuff surgery. Previous literature suggests that female patients have inferior outcomes after rotator cuff repairs. 3 We found female patients had poorer functional outcomes compared with their male counterparts, but no difference in pain scores. This difference was small and likely not clinically relevant. Of note, male patients had larger tear sizes and more retracted tears compared with female patients.
The ethnicity of our cohort was dominated by New Zealand European, with only a small percentage of the Indigenous Maori population, and a small percentage of Pacific Island peoples. There is a concern with ethnic disparity in health outcomes in New Zealand and other parts of the world. 1,10,23,27 Maori patients do have lower functional scores, but their improvement from baseline is comparable with non-Maori. However, the Pacific Island population does not seem to do as well. They have lower mean 5-year functional scores, and almost half the improvement scores compared with baseline, despite similar ages of presentation and similar tear sizes. It is possible that poorer access to health care may underlie this observation, as seen in other conditions in other health outcomes in New Zealand. 1,23
The retear rate in our cohort was 7.1%, with the reoperation rate even lower at 6.2%. This was taken from the patient questionnaire, as routine postoperative imaging was impractical due to the study size. This will represent a significant underestimate of actual retear rates. This makes comparison with other series difficult.
Tendon reducibility appears to be an important factor in outcome. Reducibility can be thought as a surrogate marker for repair tension, and repair tension may be an independent predictor of outcome. 12 In our cohort, the worst outcomes were seen in tendons that were unable to be reduced fully, with over 6 points difference in FLEX-SF scores. Even tears with severe retraction, or poor tendon quality, still had largely successful clinical outcomes postrepair if the tendon was easily reducible.
Tear size and outcome has been the subject of much debate. Functional scores declined with tears over 4 cm. Similarly, there was an increase in retear rates and a dropoff in functional scores in 3 tendon tears versus 1 and 2 tendon tears; however, not so in the multivariate model. Even tears over 4 cm had improvement in functional scores of over 13 points at 5 years in our cohort, making surgery still functionally beneficial for this difficult group. This mirrors other literature that found high anatomic failure after repair of massive tears, yet with reasonable functional results. 5
Limitations
There are several limitations to this study. Patient recruitment was a registry design, whereas follow-up was a cohort design. This is both an advantage and also a limitation. This allowed a large number of patients to be recruited, in an attempt to closely represent the general population. Participating surgeons were asked to enroll all patients undergoing rotator cuff under their care during the study period. Based on unpublished data from Ministry of Health and private insurance companies, we estimate the cohort covers over 70% of the total repairs carried out across New Zealand during the study period. The multicenter, registry cohort design also introduces variability in surgical technique and postoperative rehabilitation. In total, 90 surgeons submitted data, which creates variability in subjective operative findings such as tendon quality and tendon reducibility. In an attempt to limit variability, all surgeons were part of the New Zealand Shoulder and Elbow Society. Surgeons were educated on study protocols and data collection, and data collection tools were kept as user-friendly as possible.
The lack of follow-up examination and follow-up and imaging is also a limitation. The large number of patients meant follow-up imaging was impractical. The cost of imaging was beyond the scope and budget of this study. We therefore report complication rates and, in particular, retear rates with caution. These were not confirmed with radiological imaging. The large numbers made radiological follow-up impractical; however, we achieved a high follow-up percentage in a large cohort for the key patient-focused outcomes of pain and functional scores.
Conclusion
Surgical rotator cuff repairs provide a sustained clinical improvement out to 5 years. Most pain and functional gains occur within the first 6 months but can continue to improve out to 24 months. Most population groups do well after rotator cuff repairs, including those aged over 70 years. Tear sizes over 4 cm have lower functional scores but still acceptable improvement postsurgery, with tendon reducibility associated with successful clinical outcomes. These data will be useful in counseling patients about the outcomes of rotator cuff repairs.
Footnotes
Final revision submitted January 30, 2022; accepted March 9, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The New Zealand Rotator Cuff Registry is a charitable trust that has received funding from a number of sources: a majority grant from the New Zealand Accident Compensation Commission (government-funded agency) as well as funding from the New Zealand Shoulder and Elbow Society, The New Zealand Orthopaedic Association Trust and The Wishbone Trust, Device Technologies, Johnson & Johnson, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Northern X Regional Ethics Committee (ref No. NTX/07/04/034).