
Abstract
Background:
Structural characteristics of rotator cuff tears are used in surgical decision making. However, data on the association of tear size with patient-reported pain and function are sparse.
Purpose:
To assess the association of tear size, fatty infiltration, and muscle atrophy with shoulder pain/function in patients with cuff tears undergoing operative and nonoperative treatment.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 67 patients with rotator cuff tears were recruited for this longitudinal cohort study. Patients were determined to have a cuff tear using clinical assessment and blinded magnetic resonance imaging review. The Shoulder Pain and Disability Index (SPADI) was used as a measure of shoulder pain and function.
Results:
Tear size and thickness were not significantly associated with pain (SPADI pain score, 60.6 [95% CI, 49.8-71.5] for partial-thickness tear; 56.8 [95% CI, 42.8-70.7] for <2 cm full-thickness tear; 60.4 [95% CI, 51.7-69.0] for ≥2 cm full-thickness tear). Tear size and thickness were not associated with function (SPADI disability score, 42.7 [95% CI, 29.8-55.6] for partial-thickness tear; 37.6 [95% CI, 23.9-51.4] for <2 cm full-thickness tear; 45.1 [95% CI, 35.4-54.8] for ≥2 cm full-thickness tear). Fatty infiltration, muscle atrophy, and tendon retraction were also not significantly associated with SPADI pain and disability scores. A Mental Health Index score of <68 as well as age ≥60 years were significantly associated with a higher SPADI pain score. Female sex, increased number of comorbidities, Mental Health Index score of <68, and age <60 years were significantly associated with a higher SPADI disability score.
Conclusion:
In patients with rotator cuff tears undergoing operative and nonoperative treatment, pain and functional status were not associated with tear size and thickness, fatty infiltration, and muscle atrophy. Conversely, factors unrelated to cuff anatomy such as mental health, comorbidities, age, and sex were associated with pain/function. These findings have clinical implications during surgical decision making and suggest that pain and functional disability in patients with rotator cuff tears is multifactorial and should not solely be attributed to structural characteristics.
In the United States, an estimated 272,148 rotator cuff repairs were performed in 2006—an increase of 141% from 1996. 5 Although structural characteristics such as size of rotator cuff tear, fatty infiltration, and muscle atrophy are some of the factors considered during surgical decision making, 8,23 the association of tear size with patient symptoms and function is debated. 6,10,13 A few previous studies suggest that increase in rotator cuff tear size is associated with progression from an asymptomatic to a symptomatic rotator cuff tear. 15 –17,28,29
The objective of our study was to determine the association of structural characteristics such as rotator cuff tear size, muscle atrophy, and fatty infiltration with shoulder pain and function in patients with cuff tears undergoing nonoperative and operative treatment. We also assessed the relationship of age, sex, symptom duration, body mass index, and mental health with shoulder pain and function. Our hypothesis was that shoulder pain and function were not associated with tear size but are associated with social and demographic factors.
Methods
Patient Population
We recruited a longitudinal cohort of patients with shoulder pain from orthopaedic and physiatry clinics at 2 academic medical centers between February 2011 and December 2012. The study is termed the ROW (Rotator Cuff Outcomes Workgroup) Study. Eligibility criteria for this cohort study include age 45 years and older and shoulder symptoms for at least 4 weeks. Exclusion criteria include a current shoulder fracture, prior shoulder surgery, evidence of cervical radiculopathy (assessed by neck pain radiating to the shoulder/arm/hand), and presence of claustrophobia, pacemaker, defibrillator, or other surgical hardware that would be a relative magnetic resonance imaging (MRI) contraindication. All the eligibility and exclusion criteria were applied to the symptomatic shoulder. In cases with bilateral shoulder involvement, the shoulder with a greater degree of pain was assessed. We recruited 79 patients with rotator cuff tears that met our diagnostic criteria for the ROW study. Of the 79 patients, 8 patients were excluded because they ultimately needed a shoulder arthroplasty, and 4 patients were excluded because of missing data on Shoulder Pain and Disability Index (SPADI) scores.
Approval for this study was obtained from the institutional review boards at our institutions, and informed consent was obtained from all participants.
Shoulder Questionnaire and Standardized Pain and Function Questionnaires
A standardized shoulder and general health questionnaire was developed based on published literature and input from our shoulder experts prior to recruitment for the study. This questionnaire included information on age, sex, smoking status, symptom duration, comorbidities, and whether the patient had prior surgery (for any reason). It was administered at the patient’s baseline visit. Mental health was assessed using the Mental Health Index–5 questionnaire (MHI-5), 2 a component of the 36-item Short Form Health Survey (SF-36). 25 MHI-5 scores range from 0 to 100, and a score of ≤68 on the MHI-5 is indicative of a probable mood disorder (including depression). 12,24 Shoulder pain and function were assessed using the SPADI, 21 a standardized questionnaire. There is a pain scale and a disability scale associated with the SPADI. It has good psychometric properties, in general and specific to rotator cuff tear, 1,4,7,14,19,27 and has a minimal clinically important difference of >10 points. 27 As compared with visual analog pain scores, the SPADI pain score provides more detailed information on shoulder pain during activities such as lying down, overhead tasks, pushing objects, and internal rotation of the arm. The SPADI disability scale provides composite information on functional limitations during activities such as washing hair/back, dressing, and carrying objects and with internal rotation of the arm. SPADI scores range between 0 and 100, with lower scores representing better pain and functional status.
Standardized MRI Assessments
Once a patient was recruited, an MRI review was performed by 2 fellowship-trained shoulder experts until consensus. The reviewers were blinded to patient identifiers and clinical findings. Substantial intra- and interrater reliability of MRI assessments have been shown when compared with a musculoskeletal radiologist, with point estimates for kappa ranging from 0.75 to 0.90 for tear presence, tear size, and tear thickness. 11 Our imaging parameters for diagnosing full- and partial-thickness tears have been previously described and are based on published literature. 11,18,20 Tear size was measured for full-thickness tears in longitudinal and transverse planes. Tear size was categorized into partial-thickness tear, <2 cm full-thickness tear, and ≥2 cm full-thickness tear. In cases of multiple tendon tears, only the largest longitudinal/transverse tears were considered in the analyses. Fatty infiltration was determined based on the classification described by Goutallier et al, 9 and classification of muscle atrophy was based on that by Warner et al. 26 Tendon retraction in the coronal plane was classified in stages as described by Boileau et al. 3
Determination of Rotator Cuff Tear
We used strict criteria to determine the presence of a rotator cuff tear. Participants underwent a clinical assessment (without taking imaging findings into consideration) by a fellowship-trained shoulder/sports medicine attending physician. Based on their clinical assessment, the attending physician marked the degree of certainty, on a continuous scale of 0 to 100, that the patient’s symptoms were attributable to a rotator cuff tear. As described above, a blinded standardized MRI review was subsequently performed. Participants were determined to have a symptomatic rotator cuff tear if the degree of certainty marked by the attending physicians was at least 50% and the MRI confirmed the presence of a rotator cuff tear on blinded review.
Patients were referred for operative or nonoperative treatment during their clinical visit independent of our study protocol.
Statistical Analysis
Since SPADI pain and disability scales capture different dimensions in patients with rotator cuff disorders, we assessed these 2 scales as separate outcome measures (rather than as a composite scale). We determined bivariate associations of SPADI pain and SPADI disability scores with characteristics such as age, body mass index, MHI-5 score, and number of comorbidities. We also assessed the relationship between SPADI scales and MRI features such as tear size, fatty infiltration, and muscle atrophy. We used analysis of variance to assess association between SPADI scores and the variables of interest.
Results
A majority of participants in our study were ≥60 years of age (58%), and 55% of patients were male (Table 1). Our cohort consisted of patients undergoing operative (48%) and nonoperative (52%) treatments. The median SPADI pain score was 60.0, and the median SPADI disability score was 40.0. A majority of patients in our cohort had full-thickness tears (69%) (Table 2). Tear size and thickness were not significantly associated with SPADI pain (partial-thickness, 60.6 [95% CI, 49.8-71.5]; <2 cm, 56.8 [95% CI, 42.8-70.7]; ≥2 cm, 60.4 [95% CI, 51.7-69.0]) (Figure 1A and Table 3) or SPADI disability (partial-thickness, 42.7 [95% CI, 29.8-55.6]; <2 cm, 37.6 [95% CI, 23.9-51.4]; ≥2 cm, 45.1 [95% CI, 35.4-54.8]) (Figure 1B and Table 3). Results were similar when tear sizes were assessed in longitudinal or transverse planes. There was no statistically significant association of other structural characteristics of the rotator cuff such as fatty infiltration, tendon retraction, or muscle atrophy with SPADI pain and disability scores.
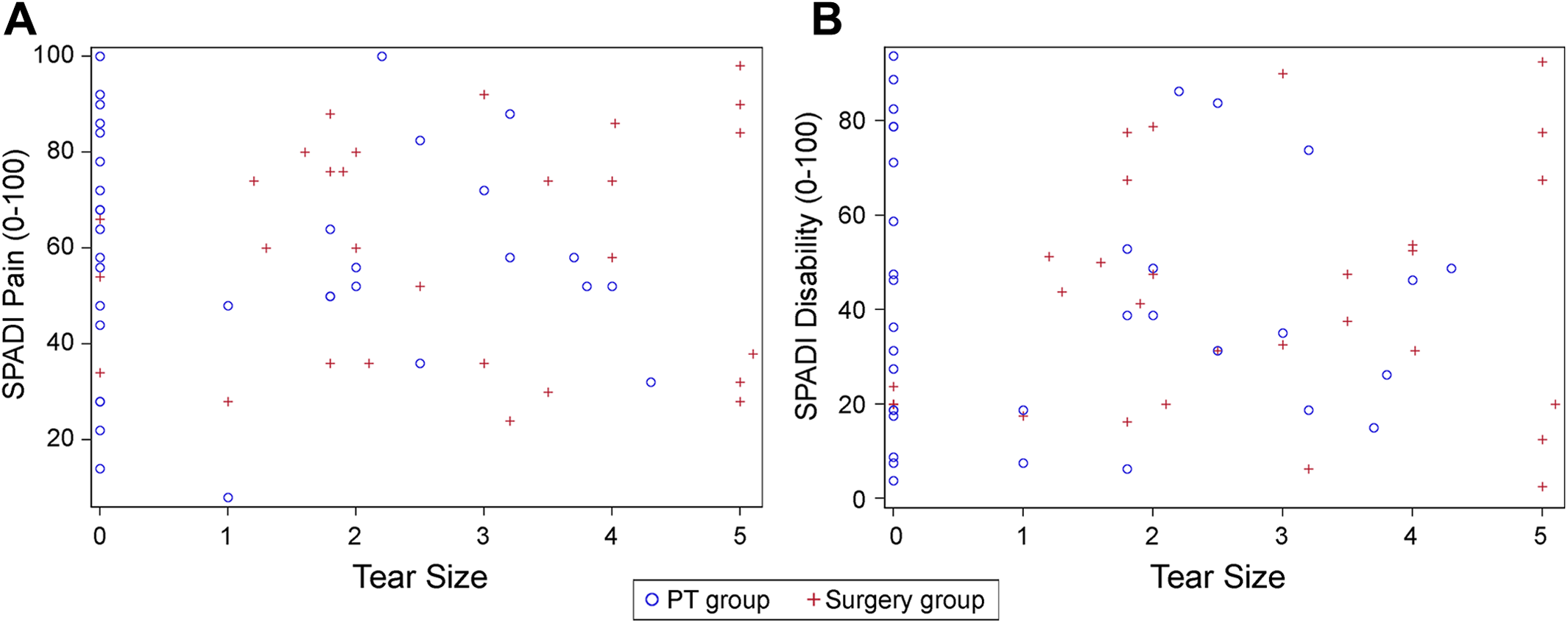
(A) Scatter plot of rotator cuff tear size and Shoulder Pain and Disability Index (SPADI) pain score. Tear size determined by tendon with the largest tear size in longitudinal or transverse planes. (B) Scatter plot of rotator cuff tear size and SPADI disability score. Tear size determined by tendon with the largest tear size in longitudinal or transverse planes.
Baseline Characteristics of Patients With Rotator Cuff Tears (N = 67) a
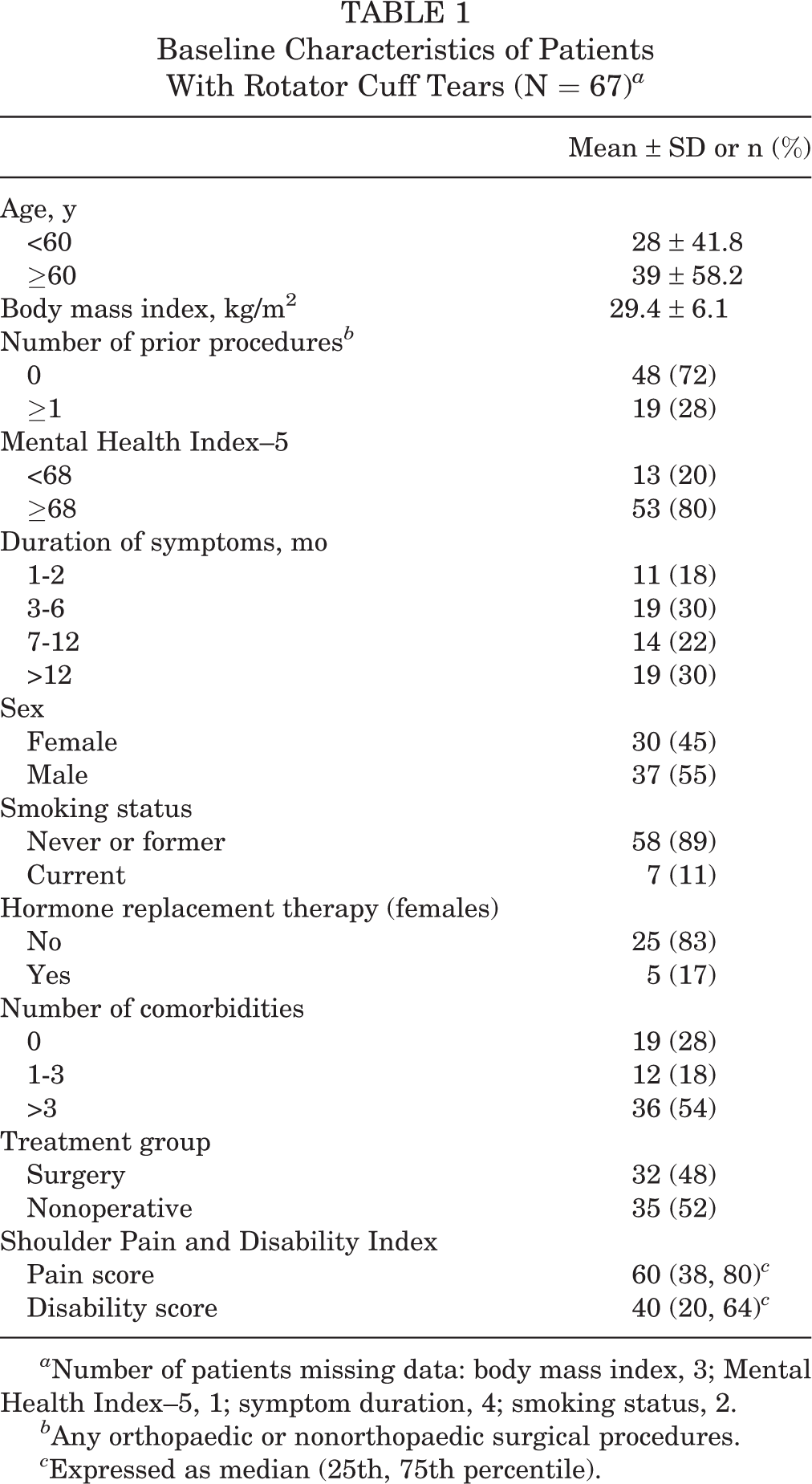
a Number of patients missing data: body mass index, 3; Mental Health Index–5, 1; symptom duration, 4; smoking status, 2.
b Any orthopaedic or nonorthopaedic surgical procedures.
c Expressed as median (25th, 75th percentile).
Magnetic Resonance Imaging Characteristics of Patients With Rotator Cuff Tears a

a Number of patients missing data: tear size and thickness, 2; longitudinal size, 2; transverse size, 2; fatty infiltration, 4; muscle atrophy, 4.
b Tear size determined by tendon having the largest size tear in longitudinal or transverse planes.
c Tear size determined by the tendon having the largest size tear.
d Grading reported for muscle most severely affected.
e Tear was partial-thickness.
f Total is >100% due to multiple tendons torn in some patients.
Association of Structural Characteristics of Rotator Cuff Tears With Pain and Function a

a Number of patients missing data: tear size and thickness, 2; fatty infiltration, 4; muscle atrophy, 4. SPADI, Shoulder Pain and Disability Index.
b Tear size determined by tendon having the largest size tear in longitudinal or transverse planes.
c Reported for the most severe among the tendons torn.
An MHI-5 score of <68 was associated with significantly higher SPADI pain scores (75.0 [95% CI, 60.5-89.4] vs 56.3 [95% CI, 50.3-62.3] in those with MHI-5 ≥68). Younger age was also associated with significantly higher SPADI pain scores (69.4 [95% CI, 61.0-77.9] for <60 years vs 53.8 [95% CI, 46.5-61.1] for ≥60 years) (Table 4). Female sex (52.3 [95% CI, 42.6-62.0] vs 35.6 [95% CI, 27.6-43.5] for males), a greater number of comorbidities, an MHI-5 score of <68, and age <60 years were significantly associated with a higher SPADI disability score (50.6 [95% CI, 39.9-61.3] vs 37.6 [95% CI, 30.0-45.3] for ≥60 years). Symptom duration, smoking status, and body mass index were not significantly associated with SPADI pain or disability.
Association of Patient Demographics and Comorbid Factors With Pain and Function in Patients With Rotator Cuff Tears a
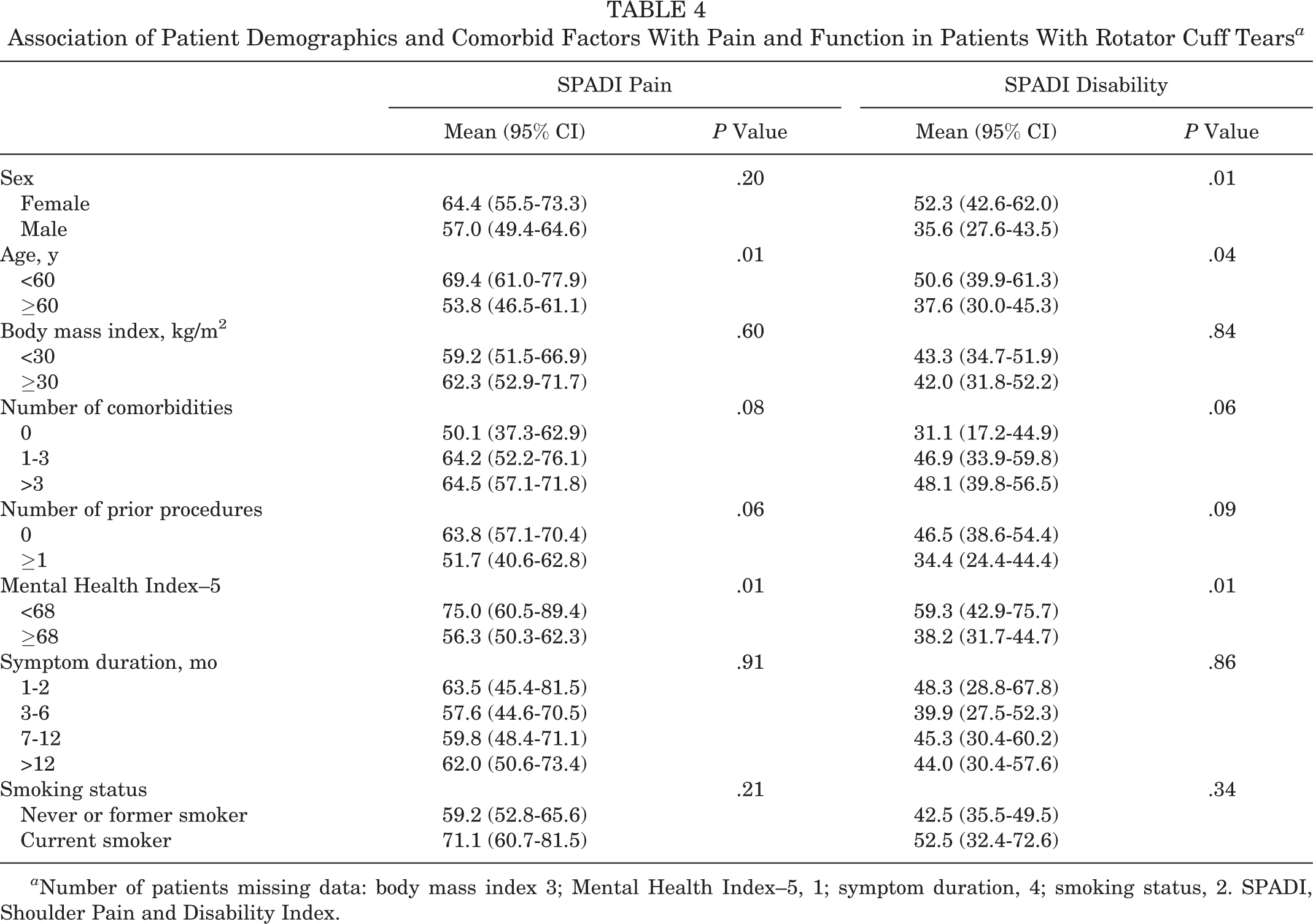
a Number of patients missing data: body mass index 3; Mental Health Index–5, 1; symptom duration, 4; smoking status, 2. SPADI, Shoulder Pain and Disability Index.
Discussion
Recent studies have heightened attention to structural attributes of rotator cuff tears, including implications of tear size progression. 15,16,29,30 These structural characteristics are used as a proxy for disease severity to inform surgical decision making. However, the association of structural characteristics with pain and function in patients with rotator cuff tears is debated. 6,10,13 We found that patient-reported pain and function is not associated with structural characteristics such as tear size, fatty infiltration, tendon retraction, and muscle atrophy in patients with rotator cuff tears undergoing operative and nonoperative treatment. Conversely, factors unrelated to structural characteristics of the rotator cuff such as MHI-5, sex, and age were associated with pain and function in patients with rotator cuff tears.
A recent study found that tendon retraction, superior humeral head migration, and fatty degeneration of the supraspinatus were not associated with visual analog pain scores in patients with rotator cuff tears. 6 This was a large and rigorously performed study but only included patients undergoing nonoperative treatment. Our study has a smaller sample size and reports on patients undergoing operative and nonoperative treatment. We also used a multi-item composite SPADI score to assess pain and function during various activities as compared with the visual analog pain score used in this recent study. Harris et al 10 found that tear size was not significantly associated with increased Western Ontario Rotator Cuff Index scores. This study also reported that female sex was associated with higher Western Ontario Rotator Cuff Index scores. 10 Zingg et al 30 reported on a cohort of patients that underwent nonoperative treatment for a massive rotator cuff tear. In this cohort, tear size and fatty infiltration increased over a mean 48-month period of follow-up; however, there was no change in functional status as measured by active range of motion. Krief and Huguet 13 found that tear size did not correlate with pain and disability as measured by the L’Insalata Self-Administered Questionnaire. Our study found that structural characteristics of the rotator cuff in patients with symptomatic rotator cuff tears were not significantly associated with pain and disability as measured by the SPADI. 15 Duration of symptoms was also not significantly associated with SPADI.
A limited number of studies have reported on progression of tear size and patient symptoms. Mall et al 15 found that a mean increase in tear size of 0.51 cm was significantly associated with progression from asymptomatic to symptomatic rotator cuff tear. Moosmayer et al 17 found that symptomatic rotator cuff tears were associated with tear size >3 cm (medial to lateral) and >grade 1 supraspinatus and infraspinatus fatty degeneration as compared with asymptomatic tears. Although our study does not provide longitudinal data on whether increase in tear size leads to deterioration in SPADI pain and disability scores, it provides evidence that structural attributes of rotator cuff tears are not associated with pain and function at baseline.
Our data show that increased pain and decreased function were associated with variables unrelated to structural characteristics of the rotator cuff such as mental health, sex, and age. Younger age was associated with increased pain and reduced function in our cohort, which may be as a result of higher demand in younger and more active patients. Similar to our results, Dunn et al 6 recently reported that an increased number of comorbidities, a lower education status, and black race were associated with a higher visual analog pain score in patients with rotator cuff tears undergoing nonoperative treatment. Harris et al 10 found that male sex was related to reduced function and increased pain in patients with a rotator cuff tears. Scarlat and Florescu 22 reported reduced shoulder function and a higher demand for treatment in patients with depression.
Limitations of our study include the inability to provide longitudinal data on progression of tear size and fatty infiltration, and its association with shoulder pain and disability. We also had a relatively smaller sample size of patients with subscapularis tears that may have different pain and functional profiles as compared with supraspinatus and infraspinatus tears. Our study also had small sample sizes for other subgroup analyses, and we do not present information on treatments received prior to presentation or whether the tear was a result of trauma. Strengths of our study include a robust cohort study design, a strict definition of rotator cuff tear based on structural findings and clinical assessment, use of a composite pain and function scale (SPADI), and the inclusion of patients undergoing operative and nonoperative treatments.
Our study provides evidence that patient-reported pain and function are not associated with tear size, tear thickness, fatty infiltration, or muscle atrophy. Factors unrelated to anatomy of the rotator cuff, such as mental health, comorbidities, younger age, and female sex were associated with pain/functional status. Our study adds to the recent literature 6 by including patients with rotator cuff tears undergoing operative and nonoperative treatments. These findings have clinical implications during surgical decision making in patients with rotator cuff tears and suggest that pain and functional disability in patients with rotator cuff tears are multifactorial and should not solely be attributed to structural characteristics of the rotator cuff.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: The project was supported by the National Center for Research Resources grant UL1RR024975-01 and is now supported by the National Center for Advancing Translational Sciences grant UL1TR000445-06. UL1TR000445-06. N.B.J. is supported by funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) 1K23AR059199, Foundation for PM&R, and Biomedical Research Institute at Brigham and Women’s Hospital. J.N.K. is in part supported by NIAMS P60 AR 047782.
Acknowledgment
The authors thank the entire ROW team (Gregory [Dan] Ayers, Lauren Burton, Abigail Byrne, Li Chen, Laurel Donnell-Fink, Peter Douglass, Alex Girden, Petar Golijanin, Frank Harrell, Elena Losina, Caitlyn McCarthy, Emily Peterson, Lindsay Miller, Matthew Provencher, Brooke Rode, Rosemary Sanders, Swastina Shrestha, Elana Siegel, Nathan Sinz, Doris Strnad, Kristin Archer Swygert, Jon J.P. Warner, Laura Huston Withrow, and Paul Yannopoulos) for their efforts. The authors also thank the clinical staff at the Orthopedic and Arthritis Center at Brigham and Women’s Hospital, the Shoulder Service at Massachusetts General Hospital, and the Sports Medicine service at Vanderbilt University Medical Center for their efforts and cooperation.