
Abstract
Background:
A fibular shortening osteotomy is needed to perform lateral closing-wedge high tibial osteotomy (LCW-HTO). To achieve this shortening, we have recently developed an acute oblique osteotomy and ligation (AO/L) procedure for the center of the fibular shaft, based on the AO procedure.
Purpose:
To compare the 2-year follow-up outcomes between the AO/L procedure and the AO procedure.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A prospective comparative cohort study was conducted involving 83 patients (83 knees) who underwent shortening osteotomy of the fibula in LCW-HTO between April 2017 and March 2019. The first consecutive 41 knees (AO group) underwent fibular osteotomy with the AO procedure. The remaining 42 knees (AO/L group) underwent fibular osteotomy with the AO/L procedure. All of the patients were evaluated for at least 2 years postoperatively via clinical and radiological assessments. To determine the time needed for complete union at the osteotomy site, we evaluated the radiographs using a radiographic union score for tibial fractures, which was modified for fibular osteotomy. Comparison of outcomes between the 2 groups was performed using the Student t test for continuous variables and the Mann-Whitney U test or Fisher exact test for discrete variables.
Results:
Around the fibular osteotomy site, no perioperative complications were found in either group. The radiographic union score was significantly higher in the AO/L group than in the AO group (P < .0001 at 2, 3, and 6 months; P = .0290 at 12 and 24 months). The union rate at the fibular osteotomy site was significantly higher in the AO/L group (97.6%) than in the AO group (82.9%) at 12 months (P = .0290).
Conclusion:
The AO/L procedure significantly accelerated the formation of bridging callus at the fibular osteotomy site and provided a significantly higher union rate compared with the AO procedure. Both AO/L and AO procedures were free from perioperative complications. These results suggest that the AO/L procedure is clinically useful as an osteotomy procedure to shorten the fibula in LCW-HTO.
Lateral closing-wedge high tibial osteotomy (LCW-HTO) is a useful surgical option for knees that have medial osteoarthritis with severe varus deformity. However, a major disadvantage is that this procedure requires shortening of the fibular shaft or manipulation of the fibular head to correct tibial alignment. Many osteotomy procedures to shorten the fibula have been reported. Previously, fibular osteotomy was carried out by transversely resecting an approximately 1 cm–long fibular shaft at the proximal one-third portion. 5,9 However, peroneal nerve palsy frequently occurred with this procedure. 3,10,19,24 Therefore, it is currently recommended that the 1 cm–long resection of the fibular shaft be performed at the central portion of the fibula. However, various complications continue to be reported. 2,4,7,12,14,18,24 For example, the incidence of peroneal nerve palsy in this procedure has been reported to range from 2.8% to 13.7%. 14,18 In addition, the nonunion rate at the fibular osteotomy site has been reported to range from 14% to 68%. 3,14,18 The high rate of nonunion at the fibular osteotomy site has been recognized as a clinical problem in this procedure because Kurosaka et al 14 pointed out that 13.7% of patients with fibular nonunion reported chronic leg pain during walking. Therefore, fibular head manipulation procedures, including fibular head osteotomy and tibiofibular joint dislocation, have currently attracted notice because these procedures avoid nonunion at the fibular shaft. 8,12,14,16,20,22 In fibular head osteotomy procedures, however, the risk of peroneal nerve palsy or lateral knee pain remains unsolved. 14,16 In tibiofibular joint dislocation procedures, progression of tibiofibular arthritis and lateral knee pain have been reported as potential problems, although the incidence of peroneal nerve palsy has been reduced. 8,16,20 Thus, current fibular osteotomy procedures have not eliminated intra- or postoperative complications. Therefore, there is a need for a new fibular osteotomy procedure that is free from perioperative complications and provides a high union rate at the fibular osteotomy site.
In 2016, we developed the acute oblique osteotomy (AO) procedure, in which a simple osteotomy is made at the central portion of the fibular shaft in an acutely inclined frontal plane. 26 In our experience, this procedure was easy and safe, but bone union at the osteotomy site was occasionally delayed. Therefore, in 2018 we developed the AO and ligation (AO/L) procedure. 26 In the AO/L procedure, fibular shaft osteotomy is performed using the AO procedure, and then the osteotomized ends are reduced and ligated using a polyester thread to accelerate bone union at the fibular osteotomy site. It was hoped that the AO/L procedure would resolve the above-described problems in fibular osteotomy. However, clinical results of the AO/L procedure have not yet been assessed.
The purpose of the present study was to evaluate the 2-year follow-up results of the AO/L procedure and compare outcomes with those of the AO procedure. The hypotheses tested in this study were as follows: (1) bridging callus formation at the fibular osteotomy site would be significantly accelerated after the AO/L procedure compared with the AO procedure, (2) the union rate at the fibular osteotomy site would be significantly higher after the AO/L procedure than after the AO procedure, (3) no perioperative complications around the fibular osteotomy site would be found after either procedure, and (4) the incidence of lateral leg pain at the final follow-up would be lower after the AO/L procedure than after the AO procedure.
Methods
Study Design
The study protocol was approved by the ethics review board of our institution, and informed consent was obtained from all individual participants. In a prospective comparative cohort study conducted in April 2017, a total of 83 patients underwent inverted V-shaped HTO (iV-HTO) in a single knee with severe varus deformity. 13 The iV-HTO is a type of LCW-HTO procedure, and as in the iV-HTO procedure, fibular osteotomy is needed to shorten the fibula. The iV-HTO is defined as a hemi-LCW and hemi–medial opening-wedge osteotomy with local bone graft. This procedure was used because (1) it could provide sufficient valgus correction of the knee with severe varus deformity more easily than could LCW-HTO procedures 1,13 ; (2) the long-term results are significantly better than those of conventional LCW-HTO 1 ; and (3) the iV-HTO does not change the posterior tibial slope angle of the tibial plateau, the patellar height, or the length of the lower limb because the center of tibial alignment correction is located approximately at the center of rotation of angulation for the lower limb deformity. 13,17
To be included in the current study, patients needed to have (1) persistent knee pain due to medial osteoarthritis (OA) that did not improve despite 3 months of nonoperative therapy, (2) a knee that needed a wedge osteotomy angle ≥10°, (3) a loss of knee extension <10°, (4) range of knee motion >130°, (5) no or mild OA changes in the patellofemoral joint, (6) intact cruciate and collateral ligaments, and (7) intact fibula surrounded by normal soft tissue.
A total of 83 knees in 83 patients (34 men and 49 women) who met the inclusion criteria underwent iV-HTO between April 2017 and March 2019 (Figure 1). This period was divided into 2 subperiods. In the first subperiod (April 2017 to March 2018), the AO procedure was performed to shorten the fibula during the iV-HTO. In the following subperiod (April 2018 to March 2019), the AO/L procedure was carried out instead of the AO procedure (Figure 1). Consequently, the first consecutive 41 knees of 41 patients (16 men and 25 women) underwent the AO procedure (AO group), and the remaining 42 knees of 42 patients (18 men and 24 women) underwent the AO/L procedure (AO/L group). All operations were performed by a senior orthopaedic surgeon (K. Yasuda), who was sufficiently trained in knee surgery. The same rehabilitation protocol was used after surgery for all 83 knees. All the patients underwent follow-up evaluations in our outpatient clinic for at least 2 years after surgery. Thus, these 83 patients were enrolled in the present study (Figure 1).

Flowchart of the patients in the 2 study groups. AO, acute oblique osteotomy; AO/L, acute oblique osteotomy and ligation.
To compare preoperative background factors between the AO/L and AO groups, we determined the patients’ age, sex, height, body weight, Kellgren-Lawrence OA grade, 11 preoperative femorotibial angle (FTA), preoperative hip-knee angle (HKA), and anatomic medial proximal tibial angle (aMPTA) before surgery. To compare the operative background factors for the performed HTO, we measured the angle of the resected bone wedge, the postoperative FTA, the postoperative HKA, and the postoperative aMPTA. To evaluate the clinical utility of each fibular osteotomy procedure, we measured the following variables and compared them between the AO and AO/L groups. (1) The operation time needed for the fibular osteotomy surgery was intraoperatively measured. (2) When perioperative complications, such as peroneal nerve palsy, vascular injury, compartment syndrome, and infection, were detected, details were precisely described in the medical record. (3) The period needed for complete union at the fibular osteotomy site was determined by evaluating the radiographs taken at 2, 3, 4, 6, 9, 12, and 24 months after surgery using the below-described radiographic union score. (4) Clinical symptoms at the osteotomy site were examined in the outpatient clinic at 24 months after surgery. (5) Overall clinical results of the HTO surgery with the fibular osteotomy were assessed using the below-described scoring systems at 24 months after surgery.
Fibular Osteotomy Procedures
The techniques of the AO procedure and the AO/L procedure were previously reported in detail. 26 In brief, for the AO procedure, the central portion of the fibula was circumferentially isolated from the surrounding tissues using 2 curved retractors using an air tourniquet (Figure 2A). Fibular osteotomy was made at the center point of the shaft on the quasi-frontal plane, which was inclined by 25° to 30° to the long axis of the fibula, using a thin oscillating saw. After completion of the HTO surgery, the ends of the osteotomized fibula were found to be displaced mainly in the coronal plane due to the change of the tibial shape (Figure 2, B and C).
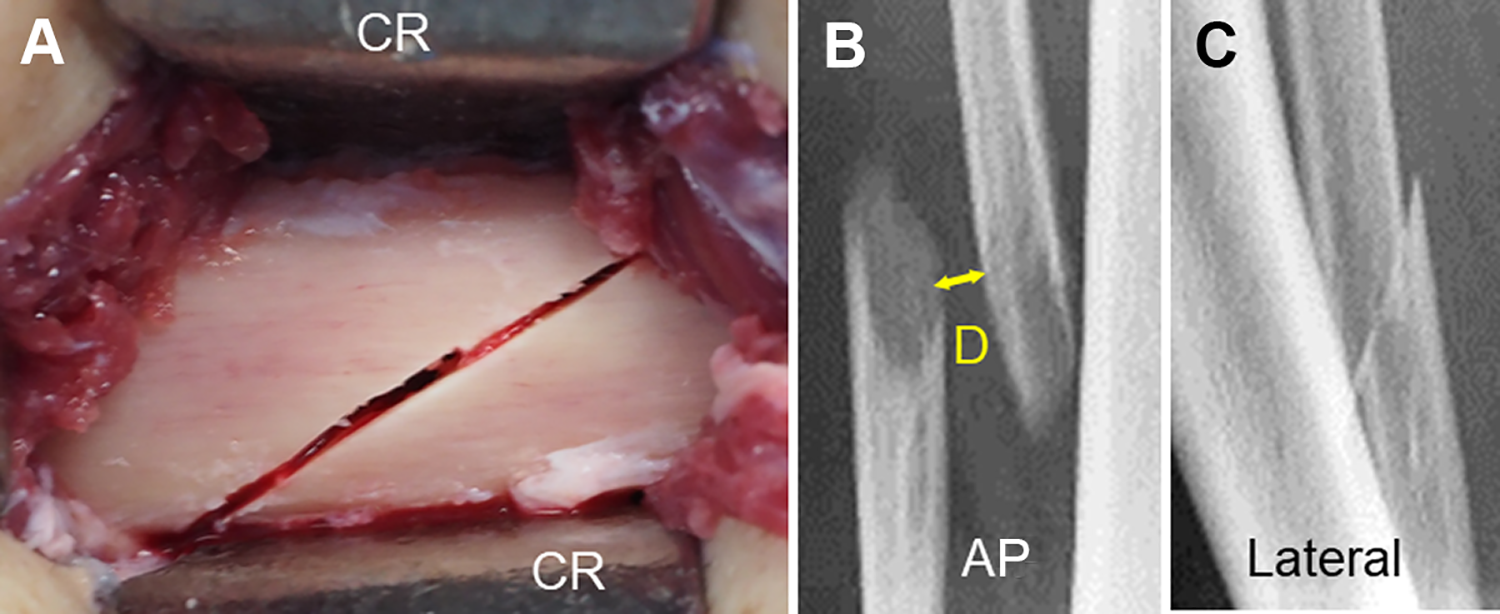
Surgical features of the acute oblique osteotomy procedure. (A) The central portion of the fibula was circumferentially isolated from all of the periosteal tissues by inserting 2 curved retractors (CR). The osteotomy line was on the quasi-frontal plane, which is inclined by 25° to 30° to the long axis of the fibula. (B and C) Anteroposterior (AP) and lateral radiographs of the fibula taken immediately after surgery. The ends of the osteotomized fibula were displaced in the coronal plane. The shortest distance (yellow arrow marked D) between the separated bone ends was defined as the initial separation distance between the osteotomized fibular ends.
In the AO/L procedure, the fibular osteotomy technique was the same as the AO procedure. Immediately before the osteotomy was completed, however, 2 holes were created using a 2 mm–diameter K-wire in the lateral cortices of the 2 fibular fragments (Figure 3A), and then a No. 2 polyester thread (Ethibond Excel Suture; Johnson & Johnson Medical N.V.) was passed through the 2 holes (Figure 3B). At this point, the HTO surgery was started. After completion of the HTO, the ends of the osteotomized fibula were displaced (Figure 3C). Then, the displaced ends of the osteotomized fibula were reduced using a thin elevator to ensure as much contact as possible between the osteotomy surfaces (Figure 3D), and the polyester thread was securely tied (Figure 3E). This ligation technique could maintain contact between the fibular ends after surgery, leaving some degree of displacement and angulation (Figure 3F). In each surgery, the subcutaneous tissue and the skin were closed after irrigation. There was no need to leave a suction tube connected to a drainage bag at the osteotomy site because postoperative bleeding from this site was minimal.

Surgical features of the acute oblique osteotomy and ligation procedure. (A) Immediately before completion of the osteotomy, 2 holes (H) were created using a 2 mm–diameter K-wire in the lateral cortices of the 2 fibular fragments. (B) A No. 2 polyester thread (PT) was passed through the 2 holes. (C) After completion of the high tibial osteotomy, the ends of the osteotomized fibula were displaced. (D) To reduce the displaced ends, the surgeon inserted a thin elevator (EL) between the ends of the osteotomized fibula. A polyester thread (PT) was passed through the 2 holes. (E) The polyester thread was securely tied several times. (F) Contact between the ends was retained after surgery, leaving some degree of displacement and angulation.
iV-HTO Procedure
The details of the iV-HTO procedure have been previously reported. 13 In brief, a lateral wedge resection angle was determined for each knee so that the mechanical axis in the corrected limb passed through a point on the lateral tibial plateau, which was 65% lateral to the medial edge of the tibial joint surface. Under observation via a C-arm fluoroscope, a K-wire was inserted perpendicular to the anterior surface of the proximal tibia and into the apex of the V-shaped osteotomy (Figure 4A). The apex of the V-shaped osteotomy is located at the center of the tibial condylar width and approximately 2.5 cm distal to the joint surface line. A Protractor Installed Wire Insertion Guide (Olympus Terumo Biomaterials Corp), in which the angle of the 2 sleeves was matched to the angle of the planned bone resection, was attached to the apex K-wire (Figure 4B). Then, 2 other K-wires were inserted from the lateral side of the tibia through the sleeves so that each inserted K-wire precisely reached the apex wire (Figure 4C). The coronal ascending osteotomy parallel to the anterior surface of the tibial tubercle was made using a thin oscillating saw, leaving the proximal part of the tibial tubercle intact with a width of 10 mm (Figure 4D). Next, a lateral hemiwedge bone resection was made along the 2 previously inserted K-wires, using a thin oscillating saw and a thin chisel (Figure 4E). The anteromedial periosteum and a part of the superficial medial collateral ligament were scraped from the tibia just along the medial osteotomy line. A Parallel Drill Guide (Olympus Terumo Biomaterials) was attached to the apex K-wire so that the guide was located on the medial osteotomy line (Figure 4F). Multiple parallel holes were created in the tibia by inserting a 2 mm–diameter K-wire into parallel sleeves in this guide (Figure 4G). The medial side osteotomy was performed using a thin chisel along the created parallel holes. The valgus tibial correction was made by making an incomplete fracture at the apex portion of the V-shaped osteotomy, and temporary fixation was performed using 2 other K-wires (Figure 4H).
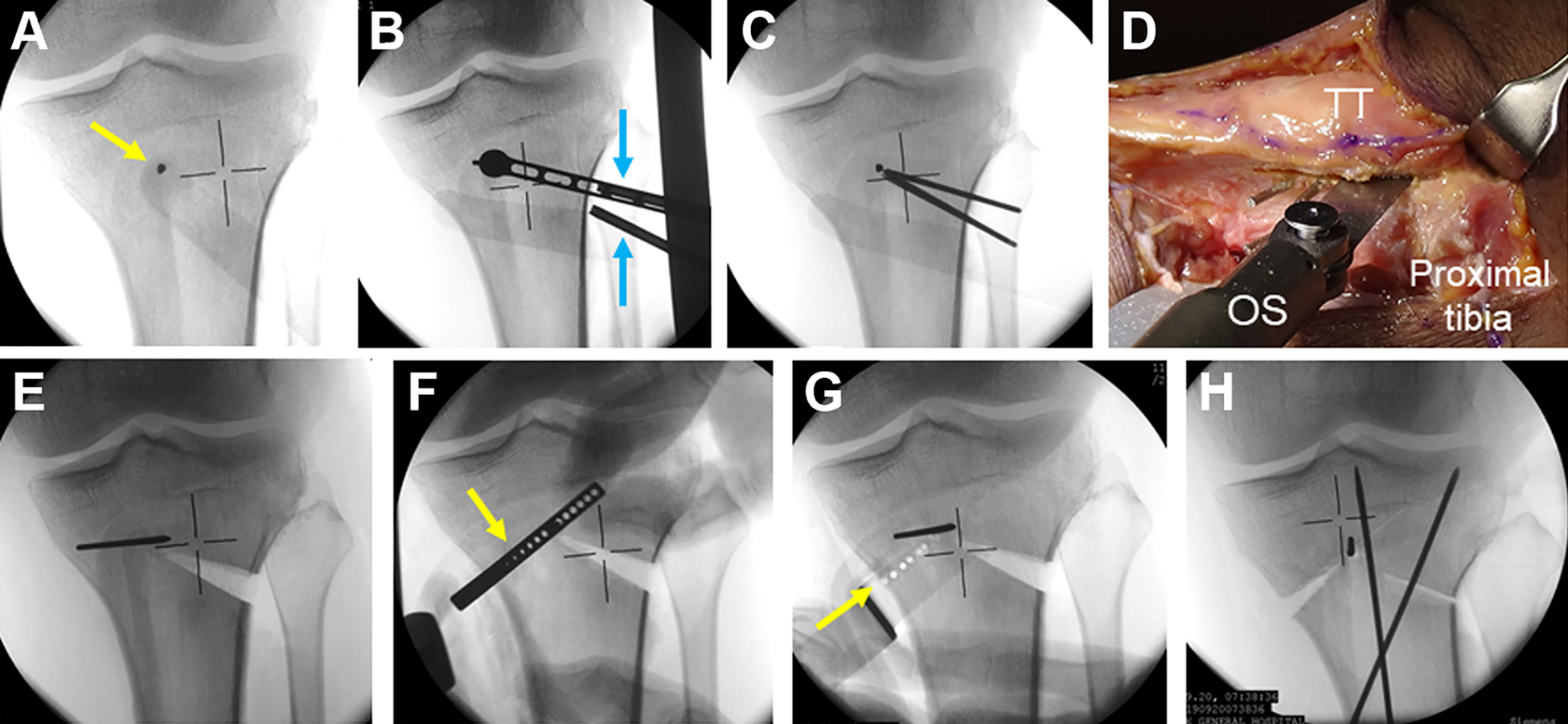
The inverted V-shaped high tibial osteotomy procedure. (A) One K-wire (indicated by a yellow arrow) was inserted perpendicular to the anterior surface of the proximal tibia and into the point that was located at the center of the tibial condyle width and approximately 2.5 cm distal to the joint surface line. (B) The guide (indicated by blue arrows) was attached to the apex K-wire. (C) Two K-wires were inserted from the lateral side of the tibia. (D) The coronal ascending osteotomy was made using an oscillating saw (OS), leaving the proximal part of the tibial tubercle (TT) intact with a width of 10 mm. (E) A lateral hemiwedge bone resection was made. (F) The parallel guide (indicated by a yellow arrow) was attached to the apex K-wire. (G) Multiple parallel holes (indicated by a yellow arrow) were created in the tibia. (H) After the valgus tibial correction was made, temporary fixation was performed using 2 other K-wires.
Tibial fixation was performed using a locking compression plate (Olympus Terumo Biomaterials), which was installed at the lateral side (Figure 5). Finally, morselized bone chips, which were made from the wedged bone resected from the lateral tibia, were implanted in the medial opening space that was created after the alignment correction (Figure 5B). After irrigation, the subcutaneous tissue and the skin were closed.

Representative radiographs of a knee that underwent the inverted V-shaped high tibial osteotomy with fibular osteotomy using the acute oblique osteotomy and ligation procedure. (A) Preoperative radiograph. (B and C) Radiographs taken 1 week postoperatively. The lateral part of the V-shaped osteotomy was in contact after fixation using a locking compression plate. Morselized bone chips were densely implanted in the medial opening space created after the alignment correction (indicated by blue arrows). Contact between the fibular ends was retained via the ligation technique after surgery (indicated by yellow arrows), leaving some degree of displacement and angulation. (D and E) Radiographs taken 3 months postoperatively. The tibial osteotomy portion was united, and callus formation was observed at the fibular osteotomy portion (indicated by yellow arrows). Preop., Pre-operation; Postop., Post-operation; 3M, 3 months; 1W, 1 week.
Postoperative Management
A previously reported rehabilitation protocol, which was created for the iV-HTO, 13 was used for each group postoperatively. No specific rehabilitation for the fibular osteotomy was performed. Quadriceps exercise with quadriceps-setting and straight leg raising was allowed 1 day after surgery. Passive knee motion from 0° to 90° was allowed during the first 2 weeks, and active knee motion from 0° to 120° was encouraged thereafter. Partial weightbearing using a pair of crutches was allowed at 3 weeks, and full weightbearing was permitted at 5 weeks.
Evaluation Methods
The operation time needed for each fibular osteotomy surgery was measured using a stopwatch by a trained paramedical staff member who was independent of this study. The operation time for the AO procedure was defined as the time from starting the lateral skin incision until completion of the oblique fibular osteotomy. The operation time for the AO/L procedure was defined as the total time used for the following 2 phases of this procedure: The first phase was from starting the lateral skin incision until passing a polyester suture into the 2 holes created on the fibula, and the second phase was from starting to reduce the displaced ends of the osteotomized fibula after completion of the HTO until securely tying the polyester suture to fix the ends of the osteotomized fibula.
On anteroposterior (AP) and lateral radiographs taken immediately after surgery, the shortest distance between the separated bone ends at the osteotomy site was defined as initial separation distance between the osteotomized fibular ends (Figure 2).
Postoperatively, AP and lateral radiographs was taken at 1, 2, 3, 4, 6, 9, 12, and 24 months after surgery. The shortest distance was measured in the same manner on each set of the radiographs. To evaluate bone union at the fibular osteotomy site on the radiographs, we created a radiographic union score for fibular osteotomy (RUSF) because no such scoring systems applicable to the fibular osteotomy have been reported. We created the RUSF by modifying the radiographic union score for tibial fractures (RUST). 15,23 In the RUSF, healing of the fibular osteotomy site was assessed at each of the medial, lateral, anterior, and posterior cortices visible on AP or lateral radiographs. Each cortex was given a score of 1 point if an osteotomy line was clearly visible with no callus, 2 points if there was callus formation but an osteotomy line was still visible, and 3 points if the cortices were completely bridged by callus formation but an osteotomy line was still visible or if there was a bridging callus with no evidence of an osteotomy line. The individual scores for the 4 cortices were summed to give a total score at each period (Figures 6 and 7).
In the present study, a maximum score of 12 points on the RUSF was considered to indicate complete union, and the time when a total score reached 12 points was referred to as union time at the fibular osteotomy site for each patient. When the osteotomy line was still clear at the osteotomy site at 12 months after surgery, this was considered to indicate nonunion at the osteotomy site. 21 Three experienced orthopaedic surgeons (D.U., T.K., J.Y.), who were blinded to all clinical information, acted as observers and independently scored each set of radiographs. Interrater reliability was evaluated by comparing the scores of the 3 observers. To calculate intrarater consistency, one of the observers (T.K.) was asked to score the radiographs again at 4 weeks after the initial assessment.

Anteroposterior (AP) and lateral radiographs of a representative patient (age, 65 years) in the group that underwent acute oblique osteotomy. (A) Immediately after surgery, the radiographic union score for fibular osteotomy was 4 (the minimum) because an osteotomy line was visible with no callus at the 4 cortices. (B) At 3 months, the score increased to 7. (C) At 6 months, the score was 11.

Anteroposterior (AP) and lateral radiographs of a representative patient (age, 63 years) in the group that underwent acute oblique osteotomy and ligation. (A) Immediately after surgery, the radiographic union score for fibular osteotomy was 4. (B) At 3 months, the score increased to 7. (C) At 6 months, the score was 12 (the maximum) because the 4 cortices were completely bridged by callus.
To evaluate the overall clinical results of the operated lower limb, we used the Japanese Orthopaedic Association (JOA) score, Lysholm knee score, and Knee injury and Osteoarthritis Outcome Score (KOOS). The JOA score was used because it is the most common knee function scale in Japan. 1,25 The evaluations were performed twice: preoperatively and at 24-month follow-up. To assess residual clinical symptoms at the fibular osteotomy site, we asked each patient about the existence of any lateral leg pain during walking and tenderness at the osteotomy site in the final follow-up examination.
Statistical Analysis
Quadratic-weighted kappa was used to assess inter- and intrarater reliabilities concerning the radiographic union score. Comparisons of clinical and radiological parameters between the 2 groups were performed using the Student t test for continuous variables and the Mann-Whitney U test or Fisher exact test for discrete variables. Relationship between the initial separation distance and the period needed for bone union at the osteotomy site was analyzed with the Pearson’s correlation analysis. The analyses were performed using IBM SPSS Statistics (Version 26; IBM Corp). The significance level was set at P = .05.
An a priori power analysis was performed as follows. In the preliminary study using 20 knees in each group, the difference in union rate between the AO/L and AO procedures was 20% to 25%. A sample size of 83 knees was calculated to have 84% to 93% power to test the study hypothesis.
Results
We found no significant differences in pre- and intraoperative background characteristics between the AO/L and AO groups (Table 1). The operation time needed for the AO/L procedure was significantly longer than that needed for the AO procedure (8.2 ± 1.4 vs 5.3 ± 1.1 minutes, respectively; P < .0001). No perioperative complications were found around the fibular osteotomy site in either group. Specifically, there were no cases of peroneal nerve palsy, compartment syndrome, serious bleeding from the peroneal vessels, or postoperative infection for either procedure.
Comparison of Characteristics Between the AO Group and AO/L Group a

a Data are reported as mean ± SD unless otherwise indicated. OA grade, Kellgren-Lawrence grade for osteoarthritis. aMPTA, anatomic medial proximal tibial angle; AO, acute oblique osteotomy; AO/L, acute oblique osteotomy and ligation; FTA, femorotibial angle; HKA, hip-knee-ankle angle; OA, osteoarthritis.
Concerning the intrarater reliability of the RUSF, the weighted kappa was 0.977 (95% CI, 0.966-0.987), indicating strong agreement. Regarding the interrater reliability, the weighted kappa was 0.862 (95% CI, 0.832-0.891) between raters 1 and 2; 0.814 (95% CI, 0.767-0.862) between raters 2 and 3; and 0.781 (95% CI, 0.734-0.829) between raters 3 and 1, all indicating strong agreement. Figure 8 and Table 2 show that the RUSF in the AO/L group was significantly higher than that in the AO group at each period (P < .0001 at 2, 3, and 6 months; P = .0290 at 12 and 24 months). The temporal union rate at the fibular osteotomy site, which was calculated at 6 months, was 88.1% in the AO/L group and 29.3% in the AO group (Table 3). The former was significantly greater than the latter (P < .0001). The final union rate at the fibular osteotomy site in the AO/L group was significantly higher than that in the AO group (97.6% vs 82.9%, respectively; P = .0290) (Table 3).
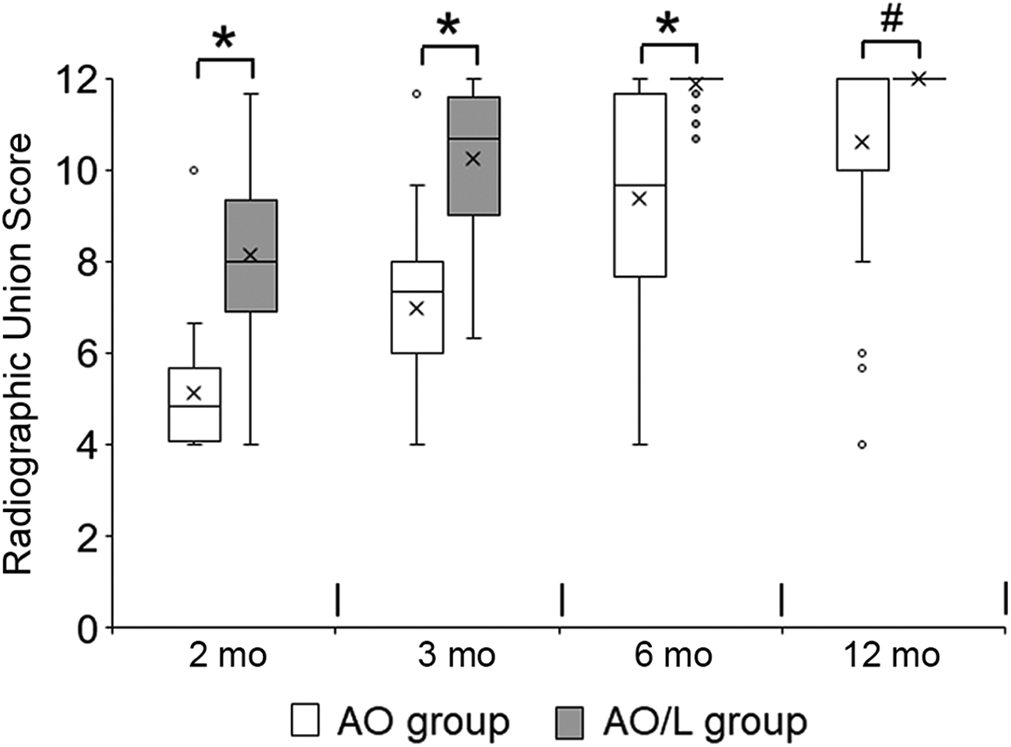
Box-and-whisker plot showing differences in distribution of the radiographic union score for fibular osteotomy at 2, 3, 6, and 12 months between the patients who underwent acute oblique osteotomy (AO group) and those who underwent AO and ligation (AO/L group). The × symbol in each box represents the mean, the line in the box represents the median, the top and bottom boundaries of the box represent the interquartile range, and the whiskers represent the minimum and maximum values. Outliers are plotted with small circles. The score in the AO/L group was significantly greater than that in the AO group at each period (*P < .0001, # P = .0290; Mann-Whitney U test). The data at the 24-month period were omitted because they were identical to those at 12 months. The actual values are shown in Table 2.
Distribution of the RUSF (Modified RUST) in the AO/L and AO Groups at Each Follow-up Point a
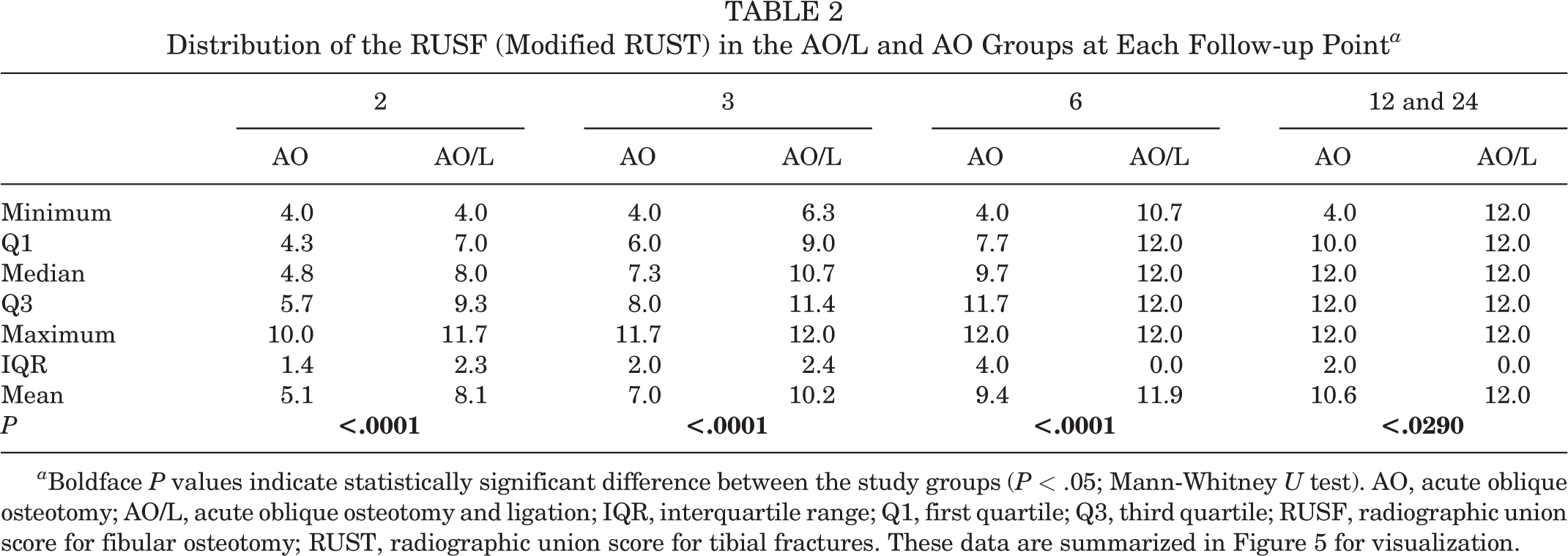
a Boldface P values indicate statistically significant difference between the study groups (P < .05; Mann-Whitney U test). AO, acute oblique osteotomy; AO/L, acute oblique osteotomy and ligation; IQR, interquartile range; Q1, first quartile; Q3, third quartile; RUSF, radiographic union score for fibular osteotomy; RUST, radiographic union score for tibial fractures. These data are summarized in Figure 5 for visualization.
Cumulative Number of Knees in Which the Fibular Osteotomy Site Achieved Complete Union at Each Follow-up Point a

a Data are reported as No. of knees (cumulative union rate, %). Complete union was defined as the knee to which all raters provided full marks (12 points) when evaluating healing at the fibular osteotomy site using the radiographic union score for fibular osteotomy, a modification of the radiographic union score for tibial fractures. The cumulative union rate was the cumulative number of knees divided by the total number of knees. Boldface P values indicate statistically significant difference between groups (P < .05). AO, acute oblique osteotomy; AO/L, acute oblique osteotomy and ligation. Dash indicates comparison was not made.
The initial separation distance between the osteotomized fibular ends in the AO/L group was significantly smaller than that in the AO group (0.4 ± 0.1 vs 3.6 ± 2.3 mm, respectively; P < .0001). In both groups, there were no cases in which the separation distance was enlarged on the radiographs taken at 1 month or later compared with the initial distance. Concerning the AO group, additional analyses were performed to explain the effects of suture ligation. First, the initial distance in the 7 knees in the AO group that had nonunion was significantly greater than that in the remaining 34 knees, which had bone union (6.0 ± 1.5 vs 3.1 ± 2.1 mm, respectively; P = .0003). Second, in the 34 knees that had bone union, a significant correlation was found between the initial separation distance and the period needed for bone union at the osteotomy site (r = 0.7987; P < .0001) (Figure 9).

In the 34 knees of the acute oblique osteotomy (AO) group that had bone union without ligation, we found a significant correlation (r = 0.7987; P < .0001) between the initial separation distance and the period needed for bone union at the fibular osteotomy site.
A total of 5 patients in the AO group reported lateral leg pain during walking and tenderness at the fibular osteotomy site, whereas only 1 patient in the AO/L group reported these symptoms. All 6 of these patients had nonunion at the fibular osteotomy site. In each group, the patients who had bone union at the fibular osteotomy site did not report lateral leg pain or tenderness. Concerning the incidence of the lateral leg pain in each group, however, no statistical significance was found between the 2 groups (P = .1090).
In each group, the JOA score, the Lysholm score, and the KOOS significantly improved from preoperative to postoperative assessments (P < .0001) (Table 4). For each score, there were no significant differences between the AO/L and AO groups pre- or postoperatively (Table 4).
Overall Clinical Results Between Study Groups a

a Data are reported as mean ± SD. There were no significant differences in each score between the AO/L and AO groups preoperatively or at 24-month follow-up. ADL, Activities of Daily Living subscale; AO, acute oblique osteotomy; AO/L, acute oblique osteotomy and ligation; JOA, Japanese Orthopaedic Association; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Quality of Life subscale; Sport/Rec, sports and recreation.
b Statistically significant difference compared with preoperative value (P < .0001).
The temporal union rate at the HTO site was 36.1% at 2 months, 85.5% at 3 months, and 100% at 4 months. Thus, bone healing at the HTO site occurred much earlier than that at the fibular osteotomy site in each group. We found no correlation between union time at the HTO site and that at the fibular osteotomy site.
Discussion
The most important findings of the study are that bone healing at the fibular osteotomy site progressed significantly faster in the AO/L group than in the AO group and that the bone union rate was significantly higher in the AO/L group than in the AO group. Specifically, the temporal bone union rate calculated at 6 months was 88.1% and 29.3% in the AO/L and AO groups, respectively. The final union rate calculated at 12 months was 97.6% and 82.9% in the AO/L and AO groups, respectively. These findings showed that the AO/L procedure shortened the time to bone union with bridging callus formation at the fibular osteotomy site and provided a high union rate compared with the AO procedure.
To evaluate bone union at the fibular osteotomy site in the present study, we created the RUSF by modifying the RUST. The RUST was developed Whelan et al 23 in 2010 to standardize the evaluation of tibial fracture healing and was slightly modified by Leow et al 15 in 2016. The RUST system has been recognized as the most reliable and repeatable outcome measure to evaluate radiographic union of tibial fractures, and this system is frequently applied to fractures of other bones. 6 In the present study, the intra- and interrater reliability of the RUSF scoring system was evaluated using the weighted kappa. The results showed that the weighted kappa for intrarater reliability of the RUSF was 0.977 and the weighted kappa for interrater reliability ranged from 0.781 to 0.862. These findings indicate that the reliability of the RUSF scoring system was high enough to evaluate the healing process at the fibular osteotomy site.
The high union rate in the AO/L group can be explained by the following study findings. First, the present study showed that the bone ends were united by a rich callus formation in 82.9% of the patients in the AO group, even though the bone ends were not reduced or fixed, as shown in Figures 6 and 9. This finding indicates that the fibular ends osteotomized using the AO procedure fundamentally have a high capability of bone healing. This capability may be enhanced by the acutely inclined osteotomy, which increased the area of the cut surface of the fibula compared with the axial osteotomy. Second, in the 34 knees with bone union in the AO group, the degree of the initial separation distance significantly affected the period needed for the bone union at the osteotomy site. In addition, the separation distance in each of the 7 knees without bone union was much greater than that in the 34 knees with bone union. These findings demonstrate that bone healing at the fibular ends osteotomized using the AO technique is dependent on the initial separation distance between the fibular ends. Therefore, if the initial distance between the ends of the osteotomized fibula can be brought into contact with any surgical technique, the incidence of the nonunion can be reduced, and the period needed for bone union can be shortened. A third finding was that, as Figure 3 shows, the AO/L procedure was able to bring most of the 2 osteotomized fibular surfaces into contact. This was confirmed via radiological measurement of the initial separation distance in the AO/L group, which was approximately zero on average. In addition, there were no cases in the AO/L group in which the initial distance increased in the follow-up period after surgery. Thus, the suture used for the ligation was strong enough to keep the 2 ends of the osteotomized fibula in contact until bone union.
Considering these 3 study findings, we believe that the high union rate in the AO/L group was caused by contact between the 2 osteotomized fibular ends, which was made using the ligation technique. Therefore, it is technically important for the AO/L procedure to keep the osteotomized fibular ends in contact as much as possible, although ridged fixation or complete reduction at the fibular osteotomy site is not needed.
Previous studies have reported that peroneal nerve palsy could not be completely avoided; namely, peroneal nerve palsy occurred in 2.8% to 13.8% of patients who underwent surgery. ∥ Peroneal nerve palsy is one of the most serious complications after fibular osteotomy because this palsy is commonly regarded as an iatrogenic complication. Therefore, elimination of any risk of peroneal nerve palsy is a fundamental requirement for a new fibular osteotomy technique. The present study showed that not only peroneal nerve palsy but also other perioperative complications could be completely avoided in both the AO and AO/L groups. The reasons why these 2 procedures could be performed safely are explained by 2 technical features. First, only a simple osteotomy was performed at the central portion of the fibular shaft, which was the safest portion for avoiding peroneal nerve palsy. 5,9,25 Second, the 2 curved retractors could isolate the anterior, posterior, and medial surfaces of the fibula from the surrounding neurovascular tissues when the fibular osteotomy was performed.
In the present study, fewer patients reported lateral leg pain during walking in the AO/L group (1 patient) than in the AO group (5 patients). These 6 patients had nonunion at the fibular osteotomy site. In contrast, the patients who had complete union at the fibular osteotomy site did not report any symptoms around this site. Therefore, because the bone union rate at the fibular osteotomy site in the AO/L procedure was nearly 100%, we believe that the AO/L procedure is clinically beneficial to minimize the incidence of postoperative lateral leg pain. Concerning the incidence of this symptom in all patients, no statistical significance could be calculated between the AO/L and AO groups. The reason may be that the number of the patients in each group was insufficient for this comparison to be made. Therefore, to obtain a definite conclusion on this comparison, further studies including a larger number of patients need to be conducted in the near future.
In the present study, the overall clinical results were evaluated using the JOA score, the Lysholm score, and the KOOS because no specific scoring systems are available to evaluate fibular osteotomy procedures combined with HTO. It is fundamental to use these scoring systems in clinical studies that assess patients who undergo HTO. However, these scores mainly reflected clinical symptoms due to medial OA of the knee and results of the HTO. This may be one reason why we found no significant difference, even for the KOOS Pain subscale, between the AO/L and AO groups, which underwent HTO using the same procedure.
One of the most important requirements for fibular osteotomy is that it should be technically easy to perform. The operation time is one of the indicators used to quantify the ease of a surgical procedure. In the present study, the mean operation time needed for the AO/L and AO procedures was 8.2 and 5.3 minutes, respectively. Each operation time was short enough as a preparatory surgery for the HTO surgery, which took approximately 90 minutes to perform. To our knowledge, no previous studies have reported the operation time required for other fibular osteotomy procedures. Therefore, we could not compare the operation times measured in the present study with the time needed for other fibular osteotomy procedures. However, we believe that each operation time was one of the shortest operation times for fibular osteotomy, according to our clinical experience. The operation time needed for the AO/L procedure was longer than that needed for the AO procedure by approximately 2 minutes. This additional time interval was used to ligate the fibular ends in the AO/L procedure. Therefore, the 2-minute elongation of the operation time in the AO/L procedure was of significant value, leading to a significant increase of the bone union rate at the osteotomy site.
Strengths and Limitations
This study had several strengths. First, it was a prospective study. Second, the 2 procedures were performed by a single, highly qualified surgeon. Third, all patients underwent the same postoperative management and were followed up at the outpatient clinic for 2 years or more. Fourth, bone union at the osteotomy site was evaluated using a scoring system with high intra- and interrater reliability. However, several limitations should also be noted. First, the present study was not a randomized comparative trial. Second, the number of patients in this study was not sufficient to reach a definitive conclusion. Third, the long-term follow-up results remain unknown. Fourth, utility of the AO/L and AO procedures has not been evaluated in other LCW-HTO procedures except for the iV-HTO procedure. Fifth, the clinical results of the AO/L procedure have not been compared with previously reported procedures except the AO procedure. Beyond these limitations, we believe that the present study has added important new information to the field of knee osteotomy.
Thus, the present study showed that the AO/L procedure has 3 advantages: (1) It is simple and technically easy to perform. (2) It is safe enough to avoid perioperative complications. (3) The union rate at the fibular osteotomy site is high enough (nearly 100%) so that lateral leg pain during walking, due to nonunion of the fibula, can be avoided almost completely. Additionally, this procedure has an economic advantage; namely, the AO/L procedure does not impose any additional cost for devices to fix the fibular osteotomized site except for a nonabsorbable thread. Therefore, we believe that the AO/L procedure is clinically useful as an osteotomy procedure to shorten the fibula in LCW-HTO.
Conclusion
The AO/L procedure significantly accelerated bridging callus formation at the fibular osteotomy site and provided a significantly higher union rate (nearly 100%) compared with the AO procedure. In addition, both AO/L and AO procedures were easy and free from complications except for nonunion. These results suggest that the AO/L procedure is clinically useful as an osteotomy procedure to shorten the fibula in LCW-HTO.
Footnotes
Acknowledgment
The authors appreciate Professor Emeritus Howard Tarnoff for proofreading the English text.
Final revision submitted April 9, 2022; accepted May 17, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yagi Orthopaedic Hospital (ref No. H28-0001).