
Abstract
Proximal fibular osteotomy (PFO) is an emerging joint-preserving procedure for medial compartment knee osteoarthritis (OA), with most evidence derived from East Asian populations. Its safety and efficacy in Western patients remain underexplored. This prospective single-centre study, conducted at a tertiary university hospital in Greece (Southern Europe), evaluated 27 patients (30 knees) with medial compartment OA or knee OA with predominantly medial symptoms who underwent PFO. Primary outcomes were changes in VAS pain, Knee Society Score (KSS), Oxford Knee Score (OKS), KOOS-Jr, and EQ-5D-5 L at 12 months. Secondary outcomes included postoperative complications and conversion to total knee arthroplasty (TKA). At 12 months, all outcomes improved significantly from baseline (p < 0.001), exceeding established minimal clinically important differences: VAS −4.4, KSS +27.9, OKS +14.8, KOOS-Jr +20.6, EQ-5D-5 L + 0.27. One knee (3.3%) converted to TKA due to persistent pain. Peroneal nerve–related symptoms occurred in 36.7% of knees but resolved by 6 months. In this European (Greek) cohort, PFO provided substantial pain relief, functional improvement, and quality-of-life gains at 12 months with a favorable safety profile. These findings align with prior reports from East Asian populations and suggest that PFO may be a viable minimally invasive option for carefully selected Western patients with mild-to-moderate varus OA and medial compartment symptoms. Further high-quality research is needed to confirm these results and define PFO’s role in knee OA management.
Keywords
Introduction
Medial compartment knee osteoarthritis (OA) is a common degenerative joint disease closely linked to varus malalignment and increased medial tibiofemoral loading, leading to progressive cartilage loss, pain, and disability.1,2 Established surgical treatments for advanced medial compartment OA include high tibial osteotomy (HTO), unicompartmental knee arthroplasty (UKA), and total knee arthroplasty (TKA). 3 In younger, more active patients, TKA is often avoided due to higher lifetime revision risk—up to 35% in men in their early 50s—and concerns regarding implant longevity and patient satisfaction. 4 Consequently, joint-preserving realignment procedures, most notably HTO, are frequently preferred, and in recent years, proximal fibular osteotomy (PFO) has emerged as an alternative joint-preserving option.5,6
PFO is a relatively recent surgical approach with encouraging pain and functional outcomes supported by multiple systematic reviews and meta-analyses.2,5–7 The technique involves resection of a short segment of the proximal fibula, which biomechanical and cadaveric studies have shown to redistribute axial loads more evenly across the tibial plateau, thereby decompressing the medial compartment.8–10 Finite element analyses further indicate that PFO can correct mild varus malalignment and reduce medial compartment contact stress without significantly affecting knee stability.10,11 Compared with HTO, pooled evidence suggests that PFO can achieve comparable short-term functional improvements while offering advantages such as reduced operative time, less intraoperative blood loss, and quicker early rehabilitation—underscoring its minimally invasive profile.12,13
To date, the clinical evidence for PFO is largely derived from studies from Asia and other Eastern regions, where medial compartment OA is often associated with greater varus deformity.2,14 Epidemiological differences exist between Eastern and Western populations, with the latter showing a more balanced medial–lateral OA distribution and distinct anthropometric and alignment profiles.15,16 These differences are partly attributable to lifestyle and occupational factors common in Asian populations—such as frequent squatting, kneeling, and sitting cross-legged—which increase medial tibiofemoral loading and accelerate cartilage degeneration in the medial compartment. 17 In contrast, Western populations tend to have higher average BMI, lower engagement in deep knee flexion postures, and different gait mechanics, contributing to a more balanced medial–lateral OA distribution and a distinct pattern of disease progression.18,19 Direct comparative studies have confirmed anatomical alignment differences between Asian and Western populations, which may further influence OA presentation and progression.1,15,20 Such disparities highlight the importance of evaluating PFO outcomes in Western patients.
The present study aims to address this gap by assessing the short-term effectiveness of PFO in a European (Greek) cohort with medial compartment OA or knee OA with symptoms predominantly localized to the medial compartment, thereby contributing to the evidence and bridging the East–West disparity in the current literature.
Material and methods
Study design
This was a prospective, single-center, single-arm cohort study of consecutive adults undergoing proximal fibular osteotomy (PFO) at a tertiary university hospital in Greece (Southern Europe). Power analysis was conducted a priori for a paired-samples t-test (two-tailed, α = 0.05, power = 0.80) using the paired-design effect size dz (mean pre–post difference divided by the SD of the paired differences). The primary outcome for the a priori sample-size calculation was pain (VAS; baseline to 12 months). Published studies of proximal fibular osteotomy consistently report substantial reductions in VAS pain scores. For example, a systematic review reported mean VAS improvement from 6.32 preoperatively to 1.23 postoperatively after PFO(2). Because the standard deviation of the paired differences required to derive Cohen’s dz was not reported in these studies, we prespecified a conservative moderate paired effect size of dz = 0.60 for the a priori power calculation.2,21 Using G*Power 3.1(Heinrich-Heine-Universität Düsseldorf) (t tests → Means: Difference between two dependent means, matched pairs), the required sample was n = 22 knees; to allow for attrition and sensitivity analyses, the target was set at n = 30 knees.
Participants
Adult patients with clinically and radiographically confirmed knee osteoarthritis (OA) who attended the outpatient clinics of the Orthopaedic Department between June 2022 and June 2024 and were scheduled for surgical intervention with proximal fibular osteotomy (PFO) were eligible for inclusion. Radiographic osteoarthritis severity was graded preoperatively using the Kellgren–Lawrence classification by the senior treating orthopaedic surgeon (single reader) with extensive experience in knee osteoarthritis. Grading was not blinded to clinical information, and formal inter- or intra-observer reliability testing was not performed. 22 Preoperative knee radiographs were obtained in the standing weight-bearing position (anteroposterior and lateral views). Kellgren–Lawrence grading and assessment of medial joint space narrowing were based on the standing anteroposterior radiograph. At baseline, demographic characteristics, clinical assessment, and patient-reported outcome measures (PROMs) were collected. Ethnicity data were not systematically collected as part of the study protocol. However, the study was conducted at a tertiary university hospital in Greece, and the patient population reflects the typical demographic composition of patients presenting with knee osteoarthritis in this European clinical setting.
Inclusion criteria comprised adults with radiographic knee OA confined to the medial compartment or with symptoms predominantly localized to the medial compartment. Exclusion criteria included secondary OA (e.g., post-traumatic or inflammatory), valgus malalignment, and any condition precluding postoperative ambulation or rehabilitation.
Patients were included consecutively if they met the predefined inclusion criteria and were considered appropriate candidates for proximal fibular osteotomy based on clinical and radiographic evaluation.
Surgical technique — proximal fibular osteotomy
All procedures were performed by the same senior orthopaedic surgeon with experience in knee preservation surgery. Under spinal anaesthesia with the patient supine, a 5 cm lateral incision was made approximately 6–10 cm distal to the fibular head. The fibula was exposed between the peroneal and soleus compartments, and a 1–2 cm diaphyseal segment was resected from the central third. Closure was performed in layers (Figure 1, Figure 2). Surgical technique for proximal fibular osteotomy. (a) Skin incision marked approximately 6–10 cm distal to the fibular head, (b) Intraoperative fluoroscopic image confirming fibular segment location before resection, (c) Resected fibular segment (approximately 1–2 cm). (a) Preoperative radiograph showing medial compartment narrowing. (b) Twelve months postoperatively, widening of the medial joint space is evident following proximal fibular osteotomy.

Postoperative rehabilitation and follow-up protocol
All patients were discharged on the first postoperative day. They were instructed to ambulate with partial weight bearing using crutches, limited by pain tolerance, for the initial 2 weeks. Thereafter, unrestricted full weight bearing was permitted. Antithrombotic prophylaxis was administered for 14 days postoperatively. Patients were reviewed at the outpatient clinic at 6 weeks, and subsequently at 3, 6, and 12 months.
Outcomes and assessments
Primary endpoint: Change from preoperative baseline to 12 months in patient-reported outcomes: VAS (pain), Knee Society Score (KSS), Oxford Knee Score (OKS), KOOS-Jr and EQ-5D-5L.23–27
Secondary endpoint: Postoperative complications through 12 months, including nerve-related events and conversion to TKA.
Statistical analysis
Descriptive statistics were compiled at two levels: patient-level variables (sex, age, BMI, ASA), and knee-level variables (Kellgren–Lawrence grade and previous surgery). Continuous variables are presented as mean ± standard deviation, and categorical variables as counts and percentages using non-missing denominators.
Primary clinical outcomes (VAS, KSS, OKS, KOOS-Jr, EQ-5D-5 L) were compared within subjects between the preoperative and 12-month assessments. Normality of the paired differences was assessed with the Shapiro–Wilk test (α = 0.05); normality was not rejected for any outcome, therefore all primary analyses used paired t-tests with t-based 95% confidence intervals. For completeness, Wilcoxon signed-rank sensitivity analyses produced the same inferences. Change scores were defined as Δ = 12-month − preoperative (improvement corresponds to a decrease for VAS and an increase for KSS, OKS, KOOS-Jr, and EQ-5D-5 L). Subgroup analyses stratified by osteoarthritis severity (Kellgren–Lawrence grade) were not performed because the study was underpowered for these comparisons due to small numbers within each grade.
Postoperative complications were tabulated descriptively as counts and percentages for the overall cohort. All tests were two-sided, with p < 0.05 considered statistically significant. Analyses were conducted using IBM SPSS Statistics, Version 29.0 (IBM Corp., Armonk, NY, USA).
Ethics
This research has been approved by the authors’ affiliated institutions. All participants gave written informed consent; the study complied with the Declaration of Helsinki.
Results
Baseline demographics.

Clinical Outcomes: Preoperative vs 12-Month.

Abbreviations: VAS, visual analog scale (pain); KSS, knee society score; OKS, oxford knee score; KOOS Jr, knee injury and osteoarthritis outcome score–junior; EQ-5D-5 L, EuroQol 5-Dimension 5-Level.

Preoperative and 12-month postoperative patient-reported outcome measures. Bar chart showing significant improvements in Visual Analogue Scale (VAS), Knee Society Score (KSS), Oxford Knee Score (OKS), KOOS-Jr, and EQ-5D-5 L, all p < 0.001.
Postoperative complications.
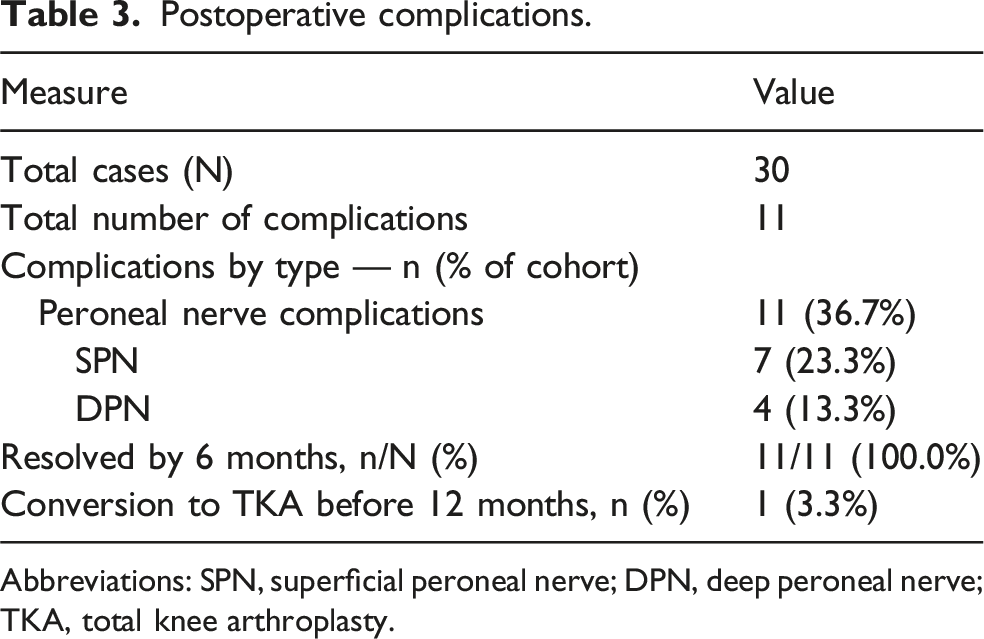
Abbreviations: SPN, superficial peroneal nerve; DPN, deep peroneal nerve; TKA, total knee arthroplasty.
Discussion
To the authors’ knowledge this is the first clinical study examining PFO clinical results in a European (Greek) cohort. In this single-centre prospective study, PFO was associated at 12 months with statistically significant and clinically meaningful improvements across all patient-reported outcomes exceeding established minimal clinically important differences (MCIDs) for each measure.28–32 These gains reflect substantial pain relief, functional recovery, and improved quality of life, while maintaining a favourable short-term safety profile in a Western cohort: only one knee (3.3%) converted to TKA due to persistent pain, and all peroneal nerve–related symptoms resolved by 6 months.
To directly contextualize our Western cohort against the predominantly East Asian PFO literature, the magnitude of improvement in our series falls within the range reported in prior pooled evidence. In our cohort, VAS improved by 4.4 points (7.9 ± 0.9 to 3.5 ± 2.1) and KSS improved by 27.9 points (48.0 ± 14.4 to 75.9 ± 17.5) at 12 months. By comparison, a systematic review of largely Asian cohorts reported mean VAS improvement from 6.32 to 1.23 and KSS functional improvement from 43.11 to 66.15 after PFO, supporting broadly similar short-term clinical gains. 2
Peroneal nerve–related sensory symptoms were observed in 36.7% of knees; however, all resolved by 6 months, consistent with transient neurapraxia rather than persistent neurological deficit. Because patient-reported outcome measures were collected at later follow-up intervals, early postoperative PROMs were not available to quantify the short-term functional impact of these transient symptoms. This incidence is higher than pooled estimates from meta-analyses (peroneal paresthesia ∼5.9%; peroneal palsy ∼2.3%). 5
However, higher short-term neurological symptom rates have been reported in individual prospective cohorts, including dorsum-of-foot paresthesia in 10% (6/60) resolving within 6–12 weeks, and combined EHL weakness and/or dorsum-of-foot tingling/numbness in 28.6% (6/21) resolving within 4–6 months.33,34 Taken together, these data indicate substantial between-study variability, likely reflecting differences in adverse-event definitions and ascertainment. The reported incidence of nerve-related symptoms after PFO varies widely across studies, reflecting differences in study design, complication definitions, and follow-up protocols. Our prospective protocol with scheduled early follow-up may have captured mild, transient paresthesia that may be under-reported when complications are not systematically documented. From an anatomical perspective, the typical osteotomy level used in proximal fibular osteotomy (approximately 6–10 cm distal to the fibular head) lies within a region where branches of the common peroneal nerve may course close to the fibular shaft. The superficial peroneal nerve demonstrates considerable anatomical variability in its course and branching pattern, including differences in compartment location and in the level at which it pierces the deep fascia. These variations may place neural structures in closer proximity to the surgical field and have been highlighted in anatomical studies as important considerations during surgical procedures involving the proximal fibula.35–37
The concept of using fibular osteotomy to alleviate medial knee overload stems from foundational biomechanical work. In a cadaveric model, Yazdi et al. (2014) first showed that removing a portion of the fibula redistributes joint loading—reducing medial compartment pressure and increasing lateral pressure—providing a mechanistic rationale for offloading the medial tibial plateau. 38 Consistent with medial unloading across models, finite-element analyses demonstrate reduced medial compartment stresses and increased lateral stresses after PFO(10).
In addition to these empirical and computational findings, several theoretical models have been proposed to explain the observed load redistribution. The “non-uniform settlement” theory (Zhang et al.) proposes that in varus-aligned knees, the medial plateau progressively collapses under load while the lateral side is buttressed by the fibula; resecting the proximal fibula reduces this support, allowing slight lateral settlement and rebalancing forces. 39 The related “too-many-cortices” theory notes that the lateral compartment is supported by two tibial cortices plus the fibula, versus one cortex medially; fibular resection removes one support and helps equalize loading. 40 Although the fibula bears only ∼6–16% of axial load, it provides key structural support to the lateral column, so its removal can shift forces and modestly improve coronal alignment without the extensive bone cuts required in high tibial osteotomy. 41 Additional complementary mechanisms have been proposed. Qin et al. described a “dynamic fibular distalization” hypothesis in which interruption of the fibular load path after PFO allows muscle traction (e.g., soleus/peroneus longus) to produce distal displacement of the fibular head; in their prospective series, the degree of distalization correlated with symptomatic improvement and varus correction. 42 Xie et al. proposed a “ground reaction vector readjustment” hypothesis, suggesting that changes in ankle/hindfoot mechanics may shift the ground-reaction force laterally and reduce the knee adduction moment, potentially contributing to early pain relief. 43 Overall, current evidence suggests PFO biomechanics are likely multifactorial, and the relative contribution of each proposed mechanism remains to be established. 40
Following the biomechanical evidence, the first clinical study of PFO was reported by Yang et al. in 2015. 39 In 110 knees, PFO produced marked pain relief and functional gains at mid-term follow-up: VAS pain scores fell significantly, while KSS and medial joint space width increased. 39 These findings have since been confirmed by multiple subsequent studies. A 2020 systematic review of case series found knee pain improved by roughly 5 points (VAS from ∼6.3 to ∼1.2) and KSS functional scores rose from ∼43 to ∼66 after PFO. 2 Mild correction of varus alignment was also observed, with femorotibial or hip–knee–ankle angles improving by 5–7° across studies.2,5 Collectively, nearly all reports describe meaningful pain reduction, better weight-bearing tolerance, and improved daily function, supporting PFO as a simple, minimally invasive option for select patients—typically those with moderate varus and medial joint space narrowing—to delay or avoid more complex surgery.7,12
An important consideration is how PFO compares to the established realignment surgery, HTO. HTO has long been used for varus knee osteoarthritis because it physically corrects malalignment by opening or closing a wedge in the proximal tibia. 12 Unlike HTO, PFO does not explicitly shift the mechanical axis by bone wedge removal, so some differences in outcomes are expected.12,44,45 Recent evidence suggests both can deliver comparable short-term pain relief and functional improvement, but with distinct trade-offs. 12 In a prospective comparative study by Zou et al., PFO achieved equivalent or better early results, with shorter operative time, less blood loss, and faster return to full weight-bearing. PFO patients also reported lower early postoperative pain, mobilized sooner, and had shorter hospital stays. Complication rates were lower with PFO (∼7.7% vs 11% for HTO), avoiding issues such as delayed bone healing, hardware problems, and thromboembolic events. 46 However, HTO provided more substantial varus correction; in some series, it shifted the mechanical axis several degrees more than PFO typically achieves.13,45,47,48 Consequently, most authors recommend PFO for mild-to-moderate varus knees, reserving HTO for severe deformity or marked lateral thrust where larger angular correction is needed.12,13,46,48
Thus, PFO emerges as a simpler, lower-risk alternative to HTO in appropriately selected patients, offering faster rehabilitation while acknowledging its more limited capacity for alignment change. Notably, all existing studies have been conducted in East Asian populations, where patient anthropometrics, activity levels, and OA patterns may differ from those in the West. Our findings provide feasibility and external validity evidence that the magnitude of short-term improvements reported in predominantly East Asian cohorts can also be observed in a Western cohort.
Although most clinical evidence on proximal fibular osteotomy originates from East Asian cohorts, the magnitude of improvement observed in our study was comparable to that reported in previous studies. One possible explanation is that the proposed biomechanical mechanisms of PFO—namely redistribution of load across the tibiofemoral joint and partial unloading of the medial compartment—are not population specific but relate primarily to local structural mechanics of the knee joint. Cadaveric, biomechanical, and finite-element studies suggest that fibular resection alters load transmission within the lateral column of the leg, allowing redistribution of forces across the tibial plateau.10,38,40 Because these biomechanical principles depend mainly on the structural relationship between the fibula and tibia rather than population-specific factors, they may operate similarly across different populations. Nevertheless, comparisons between studies conducted in different geographic regions should be interpreted cautiously, as variations in study design, patient selection, alignment characteristics, and outcome assessment methods may influence reported results.
This study has some limitations. First, the sample size was small (30 knees), although determined by a priori power analysis to be sufficient for detecting clinically meaningful pain improvement, providing confidence despite the modest cohort. Second, although adequately powered for the primary pre–post pain endpoint, the cohort included K–L II–IV with limited numbers per grade, precluding meaningful severity-stratified subgroup analyses, which may be relevant because osteoarthritis severity could influence clinical outcomes after PFO. Third, the 12-month follow-up may be too short to assess long-term outcomes, but it is consistent with most published PFO series, which rarely exceed 1 year. 7 Moreover, as this was a single-arm study without a comparator, we were unable to directly compare outcomes with alternative treatments (e.g., HTO). Another limitation of the present study is the absence of radiographic alignment parameters such as the femorotibial angle (FTA), hip–knee–ankle (HKA) angle, or quantitative assessment of joint space width. Although standard knee radiographs were obtained preoperatively for clinical evaluation and Kellgren–Lawrence grading, standardized long-leg radiographs required for formal alignment measurements were not systematically collected as part of the study protocol. Consequently, radiographic parameters were not predefined study outcomes and were not analyzed. Finally, as a single-center study with a relatively homogeneous patient group, generalizability to the broader Western population is uncertain, particularly as most existing evidence comes from Asian cohorts, mainly in China and India, with minimal Western representation.2,5
Nevertheless, despite these constraints, the present study adds novel evidence from a Western cohort, demonstrating that PFO can achieve clinically meaningful improvements in pain, function, and quality of life with a favorable safety profile. These findings, in line with the predominantly Asian literature, suggest that PFO may be a viable minimally invasive alternative to high tibial osteotomy for carefully selected Western patients, particularly those with mild-to-moderate varus deformity.
Future research should include multicenter, prospective trials with larger, more diverse populations, longer follow-up, and standardized outcome reporting to clarify PFO’s role in medial compartment knee osteoarthritis.
Conclusion
In this study, PFO achieved clinically meaningful improvements in pain, function, and quality of life at 12 months, with a favorable safety profile in patients with medial compartment OA or symptoms predominantly in medial knee compartment. While most prior evidence comes from East Asian cohorts, our results suggest PFO may also be safe and effective in European/Western populations. More high-quality research is needed to confirm these findings and clarify PFO’s role in knee OA management.
Footnotes
Ethical considerations
The local Institutional Review Board approved the study (registration No. 52871/4861/01-06- 2022). All participants gave written informed consent; the study complied with the Declaration of Helsinki.
Author contributions
K.T and AV conceived the idea for the study and supervised the whole study process. KGM, PC and SPD designed the manuscript and helped to draft the manuscript and review it. GD, V.S.I and EI participated in the study design and helped to draft the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.