
Abstract
Background:
Thoracic outlet syndrome is more common in overhead athletes. The anterior and middle scalene muscles have been associated with thoracic outlet syndrome; however, the relationship between the elastic moduli of the scalene muscles and the overhead-throwing position has not been evaluated.
Purpose:
To investigate the elastic moduli of the anterior and middle scalene muscles in simulated throwing positions using shear wave elastography.
Study Design:
Descriptive laboratory study.
Methods:
We enrolled collegiate baseball players who underwent preseason medical checkups in January and February 2020. The anterior and middle scalene muscles were visualized in the short-axis view using ultrasound. In this view, the elastic moduli of the anterior and middle scalene muscles were measured using shear wave elastography in the following arm and neck positions: (1) adduction and neutral rotation of the shoulder (neutral), (2) 90° of abduction and external rotation of the shoulder (ABER), and (3) ABER with neck rotation toward the nonthrowing side (ABER+NR). Repeated-measures analysis of variance and a paired t test were used to compare the elastic modulus values among the 3 positions and between the 2 muscles, respectively.
Results:
Overall, 30 baseball players were included. In both scalene muscles, the elastic moduli were significantly greater in the ABER versus neutral position (anterior scalene: 14.4 ± 3.8 vs 9.4 ± 2.0 kPa, respectively [P < .001]; middle scalene: 15.8 ± 5.0 vs 10.9 ± 3.4 kPa, respectively [P < .001]). In the neutral position, the elastic modulus was significantly greater in the middle scalene than the anterior scalene (10.9 ± 3.4 vs 9.4 ± 2.0 kPa, respectively; P = .03). In the ABER+NR position, the elastic modulus was significantly greater in the anterior scalene than the middle scalene (18.1 ± 4.6 vs 15.8 ± 2.6 kPa, respectively; P = .03).
Conclusion:
Because the ABER position was a simulation of the throwing position, these results indicate that this position could be associated with high elastic moduli of the scalene muscles, and both the anterior and middle scalene muscles may be involved.
The anterior and middle scalene muscles arise from the cervical spine’s transverse processes and insert into the first rib. 24 The brachial plexus and subclavian vessels travel along the scalene triangle interval, surrounded by the anterior and middle scalene muscles and the first rib bone. Thoracic outlet syndrome (TOS) is a set of symptoms caused by dynamic compression of the brachial plexus and subclavian vessels in the scalene triangle interval. 17 Patients with TOS typically experience various symptoms, including upper extremity pain, paresthesia, numbness, tingling, weakness, fatigability, swelling, and discoloration. 14,18,22,33
Prior studies have noted TOS to be more common in overhead athletes. 7,11,21 Repetitive overhead motion, such as that seen in baseball, may lead to hypertrophy or imbalance of the anterior scalene or middle scalene muscle, resulting in the development of TOS. 7 In addition, muscle fatigue after physical exercise, including repetitive throwing, can lead to stiffness and a high elastic modulus. 27,35 Both hypertrophy and stiffness of the anterior scalene muscle have been reported during surgery in patients with TOS. 3,26,30 Therefore, high elastic modulus values in the scalene muscles could be linked to the development of TOS.
Shear wave elastography (SWE) is a relatively new, real-time, diagnostic ultrasound imaging technique. The elastic modulus of tissue is calculated by measuring the velocity of shear waves as they travel through tissue. 1 This technology has been applied to musculoskeletal tissue and other parts of the body, such as the thyroid, breast, and abdominal organs. 1,2,8,13,20,25,28,32,36 Prior studies have shown a positive correlation between a change in the elastic modulus and muscle stiffness. 20 The elastic modulus can be an important parameter in assessing the condition of muscles, and more recently, SWE has been used to quantitatively assess the elastic moduli of the rotator cuff muscles as well as the shoulder capsule and labrum. 19,29,31 Thus, SWE has been shown to be a valid imaging modality to elucidate which stretch maneuver is effective for each muscle. 19,20,31,35
Bedewi et al 5 used SWE to evaluate the elastic moduli of the anterior and middle scalene muscles during shoulder adduction and neutral rotation. In the current study, we aimed to use SWE to quantitatively measure the elastic moduli of the anterior and middle scalene muscles in baseball players during simulated throwing positions. We hypothesized that both muscles would demonstrate high elastic modulus values.
Methods
Enrolled in this study were 33 male collegiate baseball players who underwent medical checkups in January and February 2020. These players were recruited from 2 college baseball teams: 1 belonged to the first division, and the other belonged to the second division. Because pitchers tend to throw more than other fielders, only pitchers were included. The protocol of the present study received institutional review board approval, and informed consent was obtained from all the participants.
All included pitchers were older than 18 years. Participants were excluded if they had a history of surgical treatment for TOS or cervical or first rib fractures. During the medical checkup, the Roos test 23 and Wright test 34 were performed on all participants to diagnose TOS. If a player had pain, paresthesia, heaviness, or weakness within 30 seconds of his arm at 90° of shoulder abduction and external rotation (ABER), he was determined to have a positive Roos test finding. If a player showed a decrease in his radial pulse with the arm at ABER, he was determined to have a positive Wright test finding. Players who had both positive Roos and positive Wright test results on their throwing side were diagnosed with TOS and excluded, while players who had only 1 positive test result were included.
Ultrasound Evaluation
The elastic moduli of the scalene muscles were evaluated using an SL 15-4 linear ultrasound transducer (Aixplorer; Supersonic Imagine). All of the sonographic examinations and elastic modulus measurements were performed by a single orthopaedic surgeon (K.T.) with 10 years of experience in shoulder ultrasonography. The participants sat on a chair, and the transducer was placed superior to the clavicle bone on the throwing side and parallel to its axis (Figure 1). The anterior and middle scalene muscles and brachial plexus were visualized in the short-axis view with ultrasound. To determine the height of the scalene muscle, the fifth cervical nerve was identified, and the anterior and middle scalene muscles were scanned along the long axis of the fifth cervical nerve. The superior surfaces of the anterior and middle scalene muscles were simultaneously visualized parallel to the surface of the fifth cervical nerve. In this view, the elastic moduli of both muscles on the throwing side were measured (Figure 2A). Measurements were taken at the end of exhalation to avoid the effects of breathing.

Arm, neck, and probe positions during the sonographic evaluation of the anterior and middle scalene muscles. (A) Neutral position: arm adducted and in neutral rotation. (B) ABER position: arm abducted and in external rotation. (C) ABER+NR position: arm abducted and in external rotation with neck rotation toward the nonthrowing side. For all 3 positions, the transducer was placed superior to the clavicle bone and parallel to its axis.
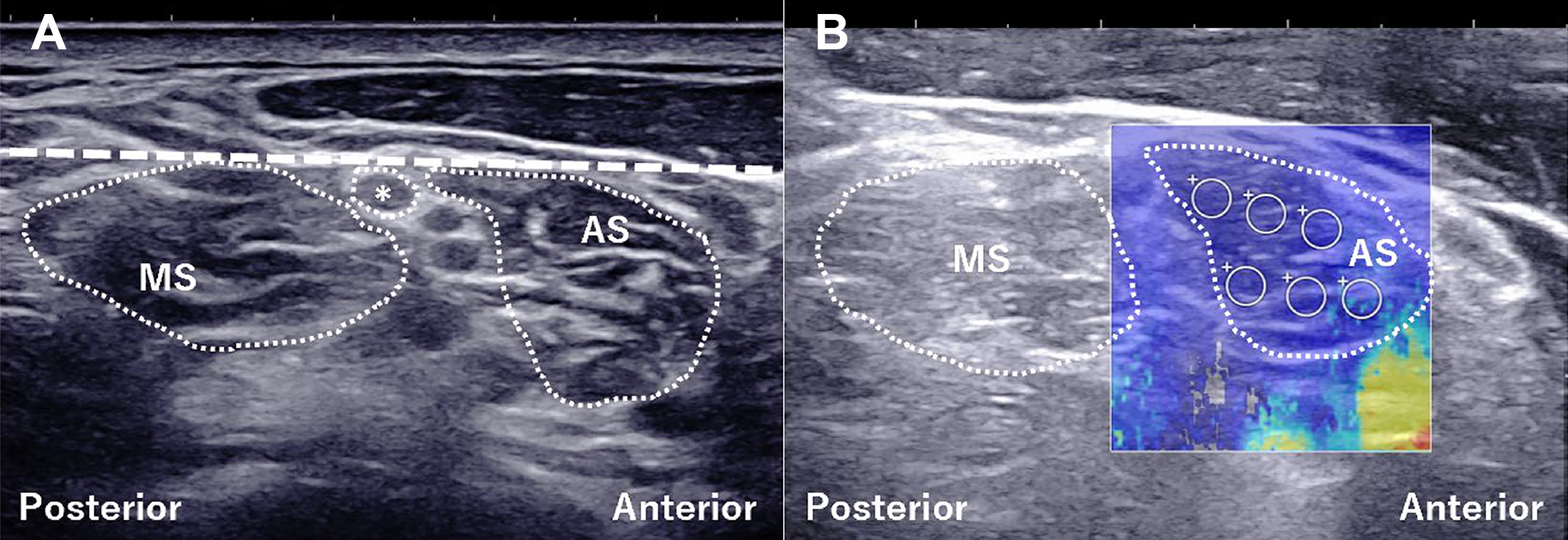
Ultrasound images of the anterior and middle scalene muscles (AS and MS, respectively). (A) B-mode ultrasound. The short-axis view of the AS, MS, and fifth cervical nerve (asterisk) were visualized (white dotted area). The superior surfaces of the AS and MS were simultaneously visualized parallel to the surface of the fifth cervical nerve (white dashed line). (B) Shear wave elastography. A color-coded box showing the elastic modulus was superimposed on the B-mode ultrasound image. The progression from blue to red indicates an increasing elastic modulus. The region of interest with a diameter of 2.0 mm (white circle) was set in 6 different points for the AS.
The elastic moduli were evaluated in the following 3 arm and neck positions: (1) adduction and neutral rotation of the shoulder (neutral) (Figure 1A), (2) ABER (Figure 1B), and (3) ABER with neck rotation toward the nonthrowing side (ABER+NR) (Figure 1C). The ABER position was used to simulate a throwing position and during the clinical examination to diagnose TOS. 23 The ABER+NR position simulated the early cocking phase of the throwing motion. 6,9 The region of interest (diameter: 2.0 mm) was set in 6 different points for each scalene muscle (Figure 2B). Finally, mean elastic modulus values were calculated.
Statistical Analysis
To determine the intratester intraclass correlation coefficient (ICC[1, 1]) of each measurement, a single orthopaedic surgeon (K.T.) performed the measurements with an interval of 1 day. To determine the intertester reliability (ICC[2, 1]), an additional orthopaedic surgeon (M.Y.) independently performed a sufficient number of sonographic examinations and elastic modulus measurements. ICC values were interpreted as poor (<0.50), moderate (0.50 ≤ ICC <0.75), good (0.75 ≤ ICC <0.90), and excellent (≥0.90). Both intratester and intertester ICCs were calculated using SPSS Statistics 23.0 (IBM).
At the beginning of the present study, an a priori power analysis was performed to determine the appropriate sample size using G*Power 3.1 software (Heinrich Heine University Dusseldorf). The results indicated that a sample size of 20 was required to achieve a statistical significance of .05 with 80% power (1 – β = 0.8; α = .05).
The data were analyzed using repeated-measures analysis of variance to compare the elastic moduli among the 3 positions. When significant differences were observed on repeated-measures analysis of variance, the post hoc Bonferroni test was performed. For statistical comparison of the elastic moduli between the anterior and middle scalene muscles, a paired t test was used to evaluate the differences. Statistical analyses were performed using EZR software (Saitama Medical Center; Jichi Medical University), and statistical significance was set at P < .05.
Results
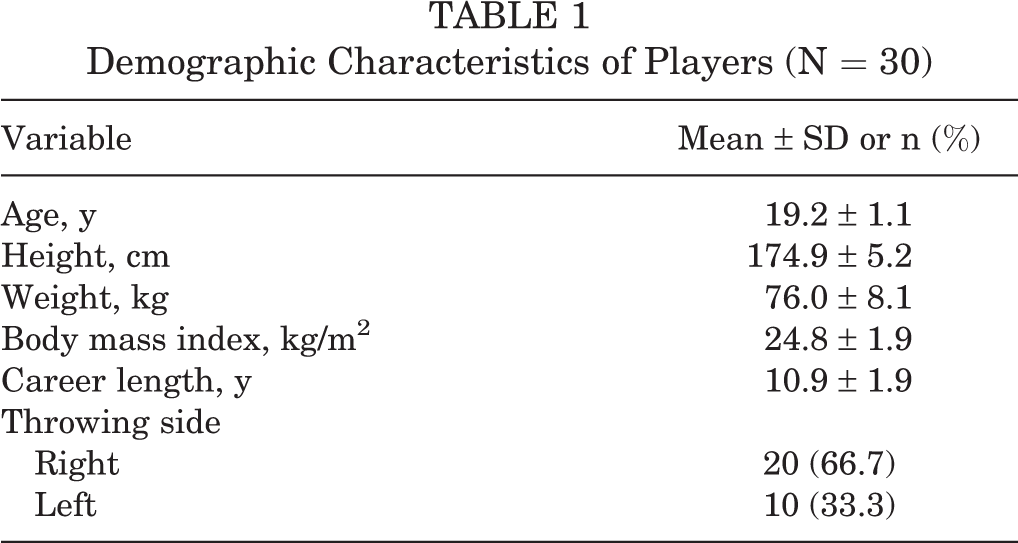
A total of 3 players had positive Roos and Wright test results on the throwing side and were excluded from the study; thus, our final sample size was 30 male collegiate baseball pitchers. Table 1 summarizes the demographic characteristics of the study participants. Regarding the ultrasound measurements, the intratester (ICC[1, 1]) and intertester (ICC[2, 1]) reliabilities were 0.867 (95% CI, 0.647-0.955) and 0.762 (95% CI, 0.390-0.918), respectively, indicating good agreement.
Demographic Characteristics of Players (N = 30)
The elastic moduli in the neutral, ABER, and ABER+NR positions were 9.4 ± 2.0, 14.4 ± 3.8, and 15.8 ± 2.6 kPa for the anterior scalene, respectively, and 10.9 ± 3.4, 15.8 ± 5.0, and 18.1 ± 4.6 kPa for the middle scalene, respectively. For the anterior scalene, significant differences in the elastic modulus were observed between the neutral and ABER positions and between the neutral and ABER+NR positions (P < .001 for both) but not between the ABER and ABER+NR positions (P = .10). Similarly, for the middle scalene, significant differences in the elastic modulus were identified between the neutral and ABER positions and between the neutral and ABER+NR positions (P < .001 for both) but not between the ABER and ABER+NR positions (P = .09) (Figure 3).
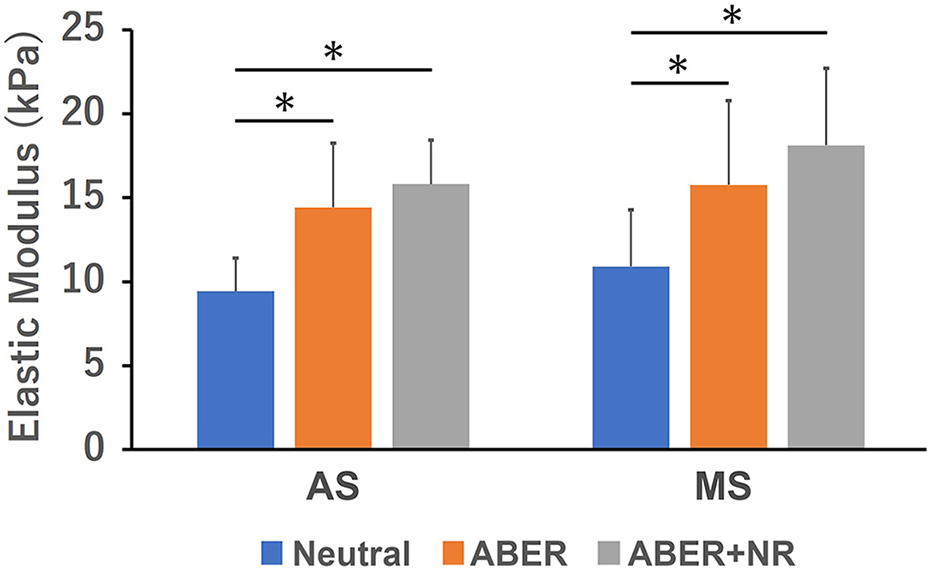
Comparison of elastic moduli among positions for the anterior and middle scalene muscles (AS and MS, respectively). *Significant difference between positions (P < .001). Neutral, adduction and neutral rotation of the shoulder; ABER, 90° of abduction and external rotation of the shoulder; ABER+NR, ABER with neck rotation toward the nonthrowing side.
In the neutral position, the elastic modulus was significantly greater for the middle scalene compared with the anterior scalene (P = .03). In the ABER position, no significant difference was observed between the muscles (P = .12). In the ABER+NR position, the elastic modulus of the middle scalene was significantly greater compared with that of the anterior scalene (P = .03) (Figure 4).

Comparison of elastic moduli between the anterior and middle scalene muscles (AS and MS, respectively) in each position. *Significant difference between the AS and MS (P < .05). Neutral, adduction and neutral rotation of the shoulder; ABER, 90° of abduction and external rotation of the shoulder; ABER+NR, ABER with neck rotation toward the nonthrowing side.
Discussion
The notable finding in this study was that the elastic moduli of the anterior and middle scalene muscles were significantly greater in the ABER position than in the neutral position (anterior scalene: 14.4 ± 3.8 vs 9.4 ± 2.0 kPa [P < .001]; middle scalene: 15.8 ± 5.0 vs 10.9 ± 3.4 kPa [P < .001]). Another important finding of this study was that the elastic modulus of the middle scalene muscle was higher than that of the anterior scalene muscle in the neutral position (10.9 ± 3.4 vs 9.4 ± 2.0 kPa, respectively; P = .03) and the ABER+NR position (18.1 ± 4.6 vs 15.8 ± 2.6 kPa, respectively; P = .03). This is the first study to quantitatively evaluate the elastic moduli of the anterior and middle scalene muscles in simulated throwing positions using SWE.
While electromyography and magnetic resonance elastography can also assess the elastic modulus of muscles, there are some disadvantages when compared with SWE. 4,12 Electromyography requires an invasive process such as needle insertion. Moreover, magnetic resonance elastography is expensive, time-consuming, and affected by the measurement environment, such as place, space, and participant positioning. In contrast, SWE is noninvasive, cost-effective, and less time-consuming. In addition, it offers real-time in vivo measurements with patients in less restricted positions. Thus, SWE is more suitable to assess the elastic moduli of the scalene muscles in simulated throwing positions. Athletes who play with the arm abducted, including baseball players, are overrepresented among patients with symptoms of TOS. 7 TOS in overhead athletes has been hypothesized to be caused by greater muscle development secondary to repetitive cycles of injury and repair of the scalene muscles. 7,24 Meanwhile, no previous studies have assessed the anterior and middle scalene muscles in different positions. This study showed that the elastic moduli of the anterior and middle scalene muscles in the ABER position were higher than those in the neutral position. However, no significant differences were observed between the ABER and ABER+NR positions. Therefore, our study quantitatively showed that the ABER position, as a simulated throwing position, was attributed to the high elastic moduli of the scalene muscles. Furthermore, the arm position was more associated with an increase in the scalene muscles’ elastic moduli than the neck position. During the throwing motion, especially between the cocking and acceleration phases, an overhead position is required on the throwing side. Moreover, in the early cocking phase, neck rotation toward the nonthrowing side is added. 6,9 Thus, during the throwing motion, the arm’s overhead position, especially shoulder abduction, may contribute to the high elastic moduli of the scalene muscles.
One of the initial treatment options for TOS is physical therapy to stretch and relax the scalene muscles. 10,16 However, nonoperative treatment methods for overhead athletes with TOS often fail to improve symptoms. 30 Effective stretching maneuvers and key muscles to TOS should be identified. SWE shows the muscle’s elastic modulus, has been used as a quantitative tool to demonstrate the stretching effect, and indicates which muscle should be targeted for treatment. 19,20,31,35 As a notable muscle in TOS, in a prior study, moderate to severe hypertrophy of the anterior scalene muscle was found in professional athletes with TOS who underwent surgical treatment, 3,30 and similar findings on magnetic resonance imaging were also seen in a baseball player with TOS. 15 In addition, anterior scalene muscle stiffness was discovered, with the brachial plexus compressed, at the time of surgery in a patient with TOS. 26 Thus, we focused on only the anterior scalene muscle, as prior studies termed this syndrome as scalenus anticus syndrome. In our study, the elastic modulus significantly increased in the middle scalene muscle. Although the anterior scalene muscle is significant, this result may suggest that both the anterior scalene muscle and the middle scalene muscle are important to understand their relationship to overhead athletes.
Limitations
This study has several limitations that should be acknowledged. First, the positions examined were static. During the throwing motion, the movement is dynamic. However, because of the acquisition time, it was difficult to measure the elastic modulus in dynamic motion using SWE. Therefore, our results may be slightly different from the actual dynamic throwing motion. Second, throwing and nonthrowing sides were not compared in this study. However, so far, only the throwing side has been reported to be associated with TOS. Hence, future studies are required to compare the nonthrowing side with the throwing side. Third, only pitchers were enrolled, and other fielders were not assessed. Fourth, there was no control group. Fifth, because only 9.1% of the participants had positive signs on both the Roos test and the Wright test, symptomatic participants were excluded, and only asymptomatic participants were included in this study. Performing these tests during the preseason may have contributed to this small proportion. Thus, the relationship between symptoms in patients with TOS and the scalene muscles’ high elastic moduli should be elucidated in future studies.
Conclusion
Abduction and external rotation of the shoulder in a simulated throwing position, showed high elastic moduli of the anterior and middle scalene muscles, while no significant differences were observed when adding neck rotation toward the nonthrowing side. The elastic modulus of the middle scalene muscle was higher than that of the anterior scalene muscle in the neutral and ABER+NR positions. These results suggest that the shoulder position should be prioritized over the neck position, and the middle scalene muscle should be considered with the anterior scalene muscle when undergoing physical therapy.
Footnotes
Acknowledgment
The authors thank staff at the Department of Orthopaedic Surgery, Nagoya City University Graduate School of Medical Sciences, and at Nagoya Sports Clinic for supporting the medical checkups.
Final revision submitted March 26, 2022; accepted May 17, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Nagoya City University Graduate School of Medical Sciences (No. 764).