
Abstract
Background:
Independent transtibial pullout repair is a common surgical technique for repairing lateral meniscus posterior root tears (LMPRTs). The shared anterior cruciate ligament (ACL) bone tunnel technique is an alternative technique for LMPRT repair combined with ACL reconstruction (ACLR) to avoid the establishment of additional bone tunnels.
Purpose:
To compare the clinical outcomes of the shared ACL bone tunnel versus the independent transtibial pullout techniques for LMPRT repair combined with ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between March 2014 and February 2018, a total of 48 patients were diagnosed with ACL injury with concomitant LMPRT; 22 patients underwent independent transtibial pullout repair (group T), and 26 patients underwent the shared ACL bone tunnel technique (group S). At a follow-up of >2 years, we compared knee functional recovery using the Lysholm, Tegner, and International Knee Documentation Committee scores and the pivot-shift test. Lateral meniscal extrusion, and cartilage degeneration on magnetic resonance imaging (MRI) scans were also compared. The healing status of the lateral meniscus posterior root was compared using second-look arthroscopy and MRI.
Results:
The duration of surgery was significantly shorter in group S compared with group T (98.3 ± 11.1 vs 127.9 ± 17.5 min; P = .001). At final follow-up, there were no significant differences between the 2 groups in knee functional scores, pivot shift, or grade of cartilage degeneration. Lateral meniscal extrusion was decreased in group S compared with group T (2.41 ± 0.61 vs 1.59 ± 1.35 mm; P = .014). Second-look arthroscopy revealed stable healing in 16 of 18 patients (88.9%) in group S and 10 of 15 patients (66.7%) in group T (P = .38).
Conclusion:
Both the shared ACL bone tunnel and the independent transtibial pullout techniques led to satisfactory clinical outcomes. The shared ACL bone tunnel technique is the simpler of the 2 procedures for combined LMPRT repair with ACLR.
Keywords
Lateral meniscus posterior root (LMPR) tears (LMPRTs) are defined as radial tears within 10 mm of the posterior root tibial attachment or posterior root avulsions of the lateral meniscus. 15 The incidence of LMPRT can be as high as 7% to 14% in patients with anterior cruciate ligament (ACL) injury. 14 However, the incidence of LMPRT alone is only 3.5% in all types of meniscal tears. 14,15 Perez-Blanca et al 23 found that the average pressure of the lateral compartment increased by 49% and the maximum contact area decreased by 33% after LMPRT. This may cause degeneration of the articular cartilage and accelerated progression of osteoarthritis. Recently, Zheng et al 29 showed that ACL injury with concomitant LMPRT causes anterolateral rotational instability of the knee, further increasing anterior tibial subluxation of the lateral compartment in knee extension.
Independent transtibial pullout repair is a common surgical technique for LMPRT 14,19,30 and contributes to positive biomechanical outcomes. 6,16,21,24 However, if this technique is used for patients who require both LMPRT repair and ACL reconstruction (ACLR), an additional tibial tunnel is required. An anatomic study performed by Johannsen et al 11 showed that the LMPR attachment center is located 6.2 to 11.0 mm outside the tibial attachment of the ACL posterolateral bundle. Because of the close distance, accurate control of the location of the 2 tibial bone tunnels is required to avoid interference. The establishment of an additional tibial tunnel also increases surgical difficulty and prolongs the duration of surgery, and multiple bone tunnels may increase the probability of iatrogenic injury to the normal structure of the knee.
Anderson et al 2 and Petersen 7 introduced an alternative transtibial pullout repair technique for combined LMPRT repair with ACLR. Since the tibial attachment of the LMPR is close to the tibial footprint area of the ACL, 8,11 a shared ACL bone tunnel is established. The shared ACL bone tunnel allows ACL grafts and pullout suture of the LMPR to pass. This technique not only avoids the establishment of an additional tibial tunnel but simplifies the surgical procedure. Only 2 previous studies have reported the clinical outcomes of the new surgical technique, labeled here as the “shared ACL bone tunnel technique,” 2,22 and no study has compared the clinical outcomes with those of the independent transtibial pullout technique.
This study aimed to compare the clinical outcomes of the shared ACL bone tunnel technique with those of the independent transtibial pullout technique for combined LMPRT repair with ACLR. We evaluated knee function recovery, magnetic resonance imaging (MRI) changes, and second-look arthroscopic findings.
Methods
Patient Enrollment
The protocol for this study was approved by our hospital, and patients provided written informed consent. We retrospectively reviewed the medical records of 516 patients with ACL injury who underwent ACLR between March 2014 and February 2018; the LMPRT was repaired concomitantly in 67 of these patients. The study inclusion criteria were (1) ACL injury with concomitant LMPRT under arthroscopy (LaPrade types 2-4), 15 (2) ACLR with autogenous hamstring tendon, (3) use of the shared ACL bone tunnel or the independent transtibial pullout technique for LMPRT repair, (4) complete preoperative and final follow-up MRI scans and knee functional assessment, and (5) a minimum follow-up of 24 months. The exclusion criteria were (1) concomitant injury of the posterior cruciate ligament or lateral collateral ligament, (2) concomitant meniscal injury other than LMPRT, and (3) degree of cartilage degeneration of grade >2 according to the International Cartilage Regeneration & Joint Preservation Society scale. 3
After application of the inclusion and exclusion criteria, 48 patients with ACL injuries with concomitant LMPRT were enrolled. Of these, 22 patients underwent the independent transtibial pullout repair (group T), and 26 underwent the shared ACL bone tunnel technique (group S) (Figure 1).

Flow diagram of this study. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; LMPRT, lateral meniscus posterior root tear.
Surgical Techniques
All surgeries were performed by 2 senior arthroscopic surgeons. Via inspection under arthroscopy, we confirmed all 48 patients had ACL injuries with concomitant LMPRT without other types of meniscal lesions (Figure 2, A and B). The independent transtibial pullout repair technique is diagrammed in Figure 2C, and the shared ACL bone tunnel technique is diagrammed in Figure 2D and demonstrated in a Video Supplement to this article.

Diagnosed ACL injury with LMPR tear under arthroscopy and schematic diagram of the surgical techniques. (A) LMPR tear (black arrow). (B) ACL injury (black arrow). (C) Independent transtibial pullout repair technique. (D) Shared ACL bone tunnel technique; the inner portal of the shared ACL tunnel was located at the midpoint of tibial footprint area of the ACL (red arrow). ACL, anterior cruciate ligament; LM, lateral meniscus; LMPR, lateral meniscus posterior root; LTP, lateral tibial plateau; MM, medial meniscus; PCL, posterior cruciate ligament.
Independent Transtibial Pullout Technique
An arthroscope was introduced into the knee compartment via a routine anterolateral portal. A meniscal rasp was used to remove the articular cartilage of the tibial attachment of the LMPR. Our technique of suturing was similar to the technique of the Chinese knot. 28 First, the suture (ORTHOCORD; DePuy Mitek Inc) was first passed through the LMPR from the tibial to the femoral side (Figure 3A). Second, the other free end of the suture was also passed through the LMPR from the tibial to the femoral side, and the middle part of the suture formed a loop under the LMPR (Figure 3B). Third, the LMPR was perforated vertically using a suture hook anterior to the midpoint between the previous 2 stitches (Figure 3C), then the loop was passed through the LMPR from the tibial to the femoral side using a suture shuttling device (Smith & Nephew). Fourth, the free ends of the sutures were passed through the loop (Figure 3D).

The independent transtibial pullout repair technique. (A) The first step of suturing. (B) The second step of suturing in which the loop was formed. (C) The LMPR was passed vertically using a suture hook anterior to the midpoint between the previous 2 stitches (black arrow). (D) The free ends of the suture were passed through the loop. (E) The ACL tibial guide was positioned at the tibial attachment of the LMPR (black arrow). (F) A guide pin was drilled at a 45° angle to establish the independent transtibial pullout tunnel. (G) The LMPR was reattached. (H) Reconstructed ACL (black arrow). ACL, anterior cruciate ligament; LFC, lateral femoral condyle; LMPR, lateral meniscus posterior root; LTP, lateral tibial plateau.
Next, the ACL tibial guide (Smith & Nephew) was introduced and positioned at the tibial attachment site of the LMPR (Figure 3E). A 2.0-mm guide pin was drilled at a 45° angle to establish the independent transtibial tunnel using the ACL tibial guide (Figure 3F). The outer portal of the tunnel was the tibial anteromedial cortex, and the inner portal was located at the tibial attachment site of the LMPR. The transtibial tunnel was reamed using a 4.5-mm cannulated drill, the free ends of the suture were pulled through the transtibial pullout tunnel using a suture manipulator (Smith & Nephew), and then the LMPR was reattached to its tibial attachment site by maintaining proper tension on the sutures (Figure 3G). The free ends of the suture were tied over a cortical button (Smith & Nephew) on the tibial anteromedial cortex in full extension of the knee. Then, single-bundle ACLR was performed. The transtibial pullout tunnel and ACL tibial tunnels were independent of each other.
Shared ACL Bone Tunnel Technique
After the LMPR tear was confirmed under arthroscopy (Figure 4A), the midpoint of the tibial footprint area of the ACL and the anatomic attachment of the LMPR were confirmed. A meniscal rasp was used to remove the articular cartilage of the tibial attachment of the LMPR. The LMPR was stitched using the same method as that for the independent transtibial pullout technique (Figure 4B). Next, the suture of the LMPR was tightened. The femoral ACL bone tunnel was established at the midpoint of the ACL femoral footprint area using the ACL femoral guide (Smith & Nephew) (Figure 4C). The ACL tibial guide (Smith & Nephew) was positioned at the midpoint of the tibial footprint area of the ACL. In the case of the ACL stump reservation, the anchor point was located at the ACL stump center (Figure 4D).

Shared ACL bone tunnel technique. (A) LMPR tear (black arrow). (B) The LMPR was sutured and tightened (black arrow). (C) The ACL femoral guide was positioned at the midpoint of the ACL femoral footprint area (black arrow). (D) The ACL tibial guide was positioned at the ACL stump center (black arrow). (E) The shared ACL bone tunnel was widened using a cannulated drill (black arrow). (F) The LMPR was reattached (black arrow). (G) ACL graft was passed through the shared ACL bone tunnel (black arrow). (H) The length of the suture from the tibial attachment of the LMPR to the shared ACL tunnel could be flexibly adjusted to ensure anatomic reattachment of the LMPR (black arrow). ACL, anterior cruciate ligament; LMPR, lateral meniscus posterior root; PCL, posterior cruciate ligament; LFC, lateral femoral condyle; LTP, lateral tibial plateau.
A 2.0-mm guide pin was drilled at a 45° angle, then the shared ACL bone tunnel was reamed using a cannulated drill (Smith & Nephew) (Figure 4E). The diameter of the shared bone tunnel was adjusted to ensure that the ACL graft and the free ends of the LMPR suture could pass smoothly. The diameters of the shared bone tunnel ranged from 7 to 9 mm, and in most cases, the diameter of the tunnel was 8 mm. The diameter of the suture was negligible. The free ends of the suture were pulled through the shared bone tunnel using a suture manipulator (Smith & Nephew). The LMPR was reattached to its tibial footprint area by pulling down on the suture and maintaining proper tension on the suture (Figure 4F). Then, the ACL graft was passed through the shared ACL bone tunnel for the single-bundle ACLR (Figure 4G).
It was necessary to maintain proper tension on the LMPR suture to prevent the LMPR from deviating from its tibial footprint area due to ACL graft implantation. The length of the suture from the tibial attachment of the LMPR to the shared ACL tunnel could be adjusted to ensure anatomic reattachment of the LMPR (Figure 4H). The ACL graft was fixed using an interference screw with sheath (Bio-INTRAFIX; DePuy Mitek Inc) at the distal end of the shared ACL tunnel in full extension of the knee. The free ends of the suture were then tied over a cortical button (Smith & Nephew) on the tibial anteromedial cortex.
Postoperative Rehabilitation
Postoperative rehabilitation was the same in both groups. Patients wore a hinged knee brace after surgery, and the knee was fixed in full extension. Active knee flexion between 0° and 90° was allowed within 4 weeks postoperatively then was allowed to reach 90°, 120°, and 150° at postoperative weeks 4, 8, and 12, respectively. Partial weightbearing was initiated at 4 weeks postoperatively; full weightbearing took place at 8 weeks postoperatively. Squatting and low-intensity running and jumping exercises were allowed at 6 months postoperatively. A full return to a competitive level of sports activities was allowed at 12 months.
Knee Function
Knee function was evaluated using the Lysholm score, 18 International Knee Documentation Committee (IKDC) score, 17 Tegner score, 25 and pivot-shift test preoperatively and at the final follow-up. 9 The preoperative pivot-shift test was performed and recorded by the 2 senior arthroscopic surgeons in the operating room before surgery. The degree of pivot shift was classified according to IKDC criteria (grades 0-3). 10
MRI Scan Evaluation
Preoperative and follow-up MRI scans were performed on a 3.0-T MRI scanner (MAGNETOM Skyra; Siemens). The MRI protocol included coronal, sagittal, and axial planes. Each sequence included T1- and T2-weighted imaging. Lateral meniscal extrusion (LME) was measured according to the method of Choi et al 5 (Figure 5A). We inspected the MFL to determine whether it was intact or impaired. According to the method of Zheng et al, 29 an intact meniscofemoral ligament (MFL) is a straight-lined hypointense band superjacent to the posterior cruciate ligament, extending from the posterior horn of the lateral meniscus to the medial wall of the intercondylar fossa (Figure 5B). A hyperintense signal indicates impaired MFL. If an MFL was not seen clearly on MRI scans due to slice position, we would look for it at arthroscopy. Articular cartilage degeneration was evaluated according to the method of Brittberg and Winalski. 3 The healing status of LMPR on the coronal and sagittal planes of T2-weighted images was classified into 3 types according to Kim et al 13 : (1) complete healing (LMPR structure is normal and a high-intensity signal is absent), (2) partial healing (more than one-third of the normal low-intensity signal of the LMPR is replaced by a high-intensity signal), and (3) failed healing (complete high-intensity signal of the LMPR).

Measurement of LME and inspection of the MFL on MRI scans. (A) LME was measured on a midcoronal image that corresponds to the midpoint of the lateral femoral condyle on the sagittal image; the LME was the distance from the lateral edge of the lateral tibial plateau to the outermost edge of the lateral meniscus. Here, an LME of 3.0 mm was observed (red lines and arrow). (B) An intact MFL on coronal MRI scan (yellow arrows). LME, lateral meniscal extrusion; MFL, meniscofemoral ligament; MRI, magnetic resonance imaging.
Two researchers measured LME independently, with the same 2 researchers repeating the measurement 2 weeks later. The intraclass correlation coefficients were computed by randomly selecting 15 patients in each group. The intra- and interobserver intraclass correlation coefficients were 0.90 (95% CI, 0.806-0.952) and 0.89 (95% CI, 0.773-0.944), respectively, indicating excellent observer and test-retest reliability.
Second-Look Arthroscopy
Second-look arthroscopies were performed for patients who wanted to remove the tibial cortical button because of its irritation and agreed to undergo second-look arthroscopic surgery. All the patients signed written informed consent forms. Healing status was divided into 3 types according to Kim et al 12 : (1) stable healing (complete connection between the LMPR and its tibial attachment with normal meniscal tension), (2) lax healing (a connection is present between the LMPR and its tibial attachment with maintenance tension to a certain extent), and (3) failed healing (a connection of fiber tissue is present between the LMPR and its attachment without tension).
Statistical Analysis
The power of this study was calculated based on the reduction of LME in groups T and S (1.59 ± 1.35 and 2.41 ± 0.61 mm, respectively); using a 1-sided alpha error of .05, we calculated the power to be 0.82. According to the assumptions of normality, the Student t test or Mann-Whitney U test was used to compare continuous variables, and the Pearson chi-square test or Fisher exact test was used to compare categorical variables. Statistical significance was set as P < .05. The data were analyzed using SPSS (Version 26.0; IBM Corp).
Results
Descriptive Data
Table 1 shows the general characteristics of the study groups. The duration of surgery was significantly different between groups T and S (127.9 ± 17.5 vs 98.3 ± 11.1 min, respectively; P = .001). All other patient and surgery characteristics were similar between groups.
Characteristics of the Study Patients (N = 48) a

a Data are presented as mean ± SD unless otherwise indicated. Boldface P value indicates statistically significant difference between groups compared (P < .05). BMI, body mass index; MFL, meniscofemoral ligament.
Functional Outcomes
In both groups, patients had significant improvement on all functional outcome measures between preoperatively and final follow-up (P = .001 for Lysholm score, IKDC score, Tegner score, and pivot shift). None of the scores were significantly different between the groups (Table 2).
Functional Outcomes a

a Data are presented as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between preoperatively and final follow-up compared (P < .05). IKDC, International Knee Documentation Committee.
MRI Outcomes
In both groups, LME was significantly decreased at final follow-up compared with preoperative values (P = .001), and LME was significantly different between groups T and S at final follow-up (1.89 ± 0.62 vs 0.96 ± 0.44 mm, respectively; P = .001) (Table 3). The amount of LME reduction from preoperatively to the final follow-up was also significantly different between groups T and S (1.59 ± 1.35 vs 2.41 ± 0.61 mm, respectively; P = .014) (Table 3 and Figure 6). The grade of cartilage degeneration did not differ between preoperatively and the final follow-up in both groups. Moreover, the healing status of the LMPR at the final follow-up was similar between the 2 groups (Figure 7).
MRI Outcomes a
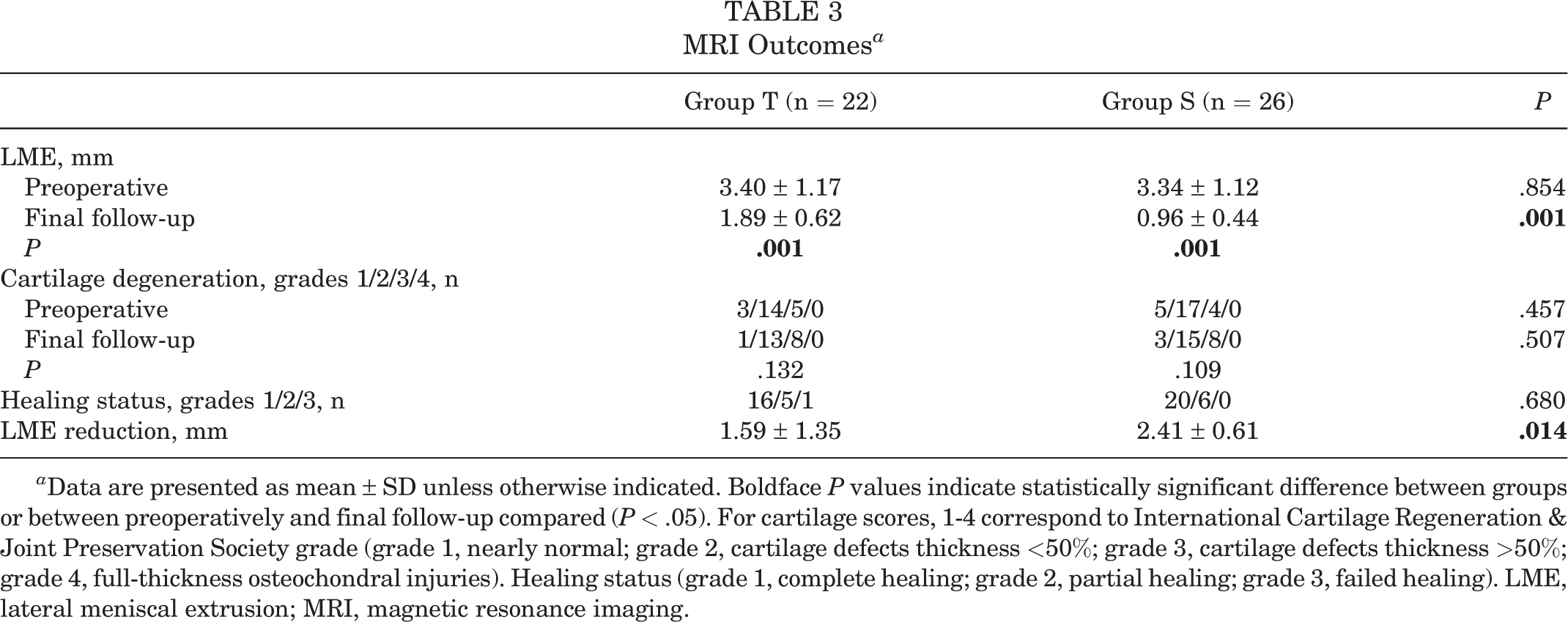
a Data are presented as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups or between preoperatively and final follow-up compared (P < .05). For cartilage scores, 1-4 correspond to International Cartilage Regeneration & Joint Preservation Society grade (grade 1, nearly normal; grade 2, cartilage defects thickness <50%; grade 3, cartilage defects thickness >50%; grade 4, full-thickness osteochondral injuries). Healing status (grade 1, complete healing; grade 2, partial healing; grade 3, failed healing). LME, lateral meniscal extrusion; MRI, magnetic resonance imaging.

LME between groups S and T. Error bars indicate SDs. *Statistically significant difference (P < .05). LME, lateral meniscal extrusion.

MRI scans at final follow-up and second-look arthroscopy. (A, E) Sensible placement of the ACL graft and sensible position of the tunnel after ACL reconstruction (yellow arrow). (B-C) Coronal and sagittal T2-weighted images showing partial healing of the LMPR indicated by partial high-intensity signal (yellow arrow). (D) Second-look arthroscopy showing lax healing of the LMPR and LMPR suture still visible (yellow arrow). (F-G) Coronal and sagittal T2-weighted images showing complete healing of the LMPR indicated by normal low-intensity signal (yellow arrow). (H) Second-look arthroscopy showing stable healing of the LMPR (yellow arrow). ACL, anterior cruciate ligament; LMPR, lateral meniscus posterior root; MRI, magnetic resonance imaging.
Second-Look Arthroscopy Outcomes
Table 4 shows the outcomes at second-look arthroscopy, performed for 15 patients in group T and 18 patients in group S. Stable healing occurred in 10 (66.7%) and 16 patients (88.9%), respectively. Lax healing occurred in 4 (26.7%) and 2 patients (11.1%), respectively. Failed healing occurred in 1 (6.6%) and 0 patients (0.0%), respectively. However, there was no significant difference in healing between the 2 groups (P = .38).
Second-Look Arthroscopy Outcomes a

a Evaluated according to Kim et al. 12 Data are reported as n (%). Percentages are rounded and may not equal 100%.
Discussion
The main findings of this study were that (1) both surgical techniques led to satisfactory clinical outcomes in patients with ACL injury concomitant with LMPRT but this study did not show that repair was superior to no repair or resection, as there was no corresponding comparison group, and (2) the shared ACL bone tunnel technique had shorter duration of surgery and resulted in simplified surgical procedures by avoiding the establishment of additional bone tunnels compared with the independent transtibial pullout repair.
In the clinical study performed by Pan et al, 22 the shared ACL bone tunnel technique was used to repair LMPRT in ACLR; final follow-up Lysholm and IKDC scores were 92.34 ± 6.32 (preoperatively, 59.03 ± 19.17) and 90.06 ± 8.59 (preoperatively, 58.35 ± 18.14), respectively. In a meta-analysis by Zheng et al 30 including 56 patients who underwent the shared ACL bone tunnel technique and 36 who underwent the independent transtibial pullout repair, the mean Lysholm score (58.3 ± 12.21 preoperatively to 91.4 ± 7.15 at follow-up) and mean IKDC score (61.1 ± 10.15 preoperatively to 87.2 ± 9.48 at follow-up) were consistent with our study. Furthermore, high-grade pivot shift did not occur in either group at the final follow-up. This suggested that both techniques lead to satisfactory outcomes of knee functional recovery and that there was no significant difference between the outcomes of the 2 techniques in our study.
Teichtahl et al 26 demonstrated that meniscal extrusion is an independent risk factor related to the progression of knee osteoarthritis. LMPRT may cause pathological extrusion of the lateral meniscus. 2 Meniscal extrusion is also a common and objective indicator with which to measure the recovery effect of the meniscus after surgery. 4 However, whether surgical repair of LMPRT can reduce LME remains controversial. In a clinical case report by Tsujii et al, 27 all-inside sutures were used to repair LMPRT. The average follow-up time was >40 months, and these authors found that LME progressed significantly. In contrast, a clinical study by Okazaki et al 21 demonstrated that tibial pullout repair had a greater effect on reducing LME compared with other surgical techniques. This was consistent with the present study, in which both surgical techniques reduced LME.
Both techniques contribute to the anatomic reattachment of the LMPR by maintaining tension on the sutures. Thus, an LMPRT repair could potentially restore joint contact biomechanics to the normal state so that balanced distribution of articular stress could reduce LME. Notably, in the current study, we found that LME was reduced to a greater extent in group S than in group T. The reason might be as follows: an anatomic study performed by Abigail et al 1 showed that there was a certain degree of difference in the location of the tibial pullout tunnel. The tibial pullout tunnel is located approximately 5.09 to 13.38 mm outside the ACL tunnel for LMPRT repair in ACLR, in some cases even farther outside to avoid mutual interference between the 2 tunnels. This may lead to outward location of the tibial reattachment of LMPR and further increase the possibility of lateral meniscal extrusion. In contrast, owing to the presence of the shared ACL tunnel, the length of the suture from the tibial attachment of LMPR to the shared ACL tunnel can be flexibly adjusted to ensure anatomic reattachment of the LMPR. Anatomic reattachment of the LMPR aids in reducing LME in the shared ACL bone tunnel technique. However, it is worth noting that, although the LME difference was significant between the 2 groups, an LME difference of approximately 1 mm may not have much clinical significance. 20
The healing rate of LMPRT after surgical repair has been the focus of research. Tsujii et al 27 used the side-to-side suture technique for LMPRT in ACLR. The average follow-up was 42.4 months; the complete healing rate was only 60.0%. In contrast, Zhuo et al 31 used the independent transtibial pullout repair for LMPRT in ACLR. They reported a higher healing rate: 31 patients were included, with an average follow-up of 29.87 months. In this latter study, stable healing occurred in 18 patients (78.3%) and lax healing in 5 patients (21.7%) under second-look arthroscopy. A meta-analysis by Zheng et al 30 found an average complete healing rate of 72.8% using several surgical techniques for the repair of LMPRT in ACLR. However, to our knowledge, there is currently no study regarding the healing rate after the shared ACL bone tunnel technique repair for LMPRT in ACLR based on second-look arthroscopic inspection. In the present study, complete healing occurred in 66.7% (10/18 patients) in group T and 88.9% (16/18 patients) in group S; no failed healing occurred in group S. This did not reach significance, as the sample size was small. However, this may suggest that both the techniques lead to satisfactory healing of the LMPR.
Limitations
This study had some limitations. First, different types of LMPR lesions may influence healing even if identical surgical repair techniques are used. However, we did not analyze subgroups of different types of LMPR injury. Second, we measured LME during nonweightbearing of the knee. However, LME may increase under weightbearing, which may have decreased our measurements. Third, this study lacked a control group without repair. Therefore, it was not clear whether both surgical techniques had a positive effect on the clinical surgical outcomes compared with nonrepaired knees. Last, the retrospective and nonrandomized design of this study should be regarded as an important limitation.
Conclusion
Both the shared ACL bone tunnel and the independent transtibial pullout techniques led to satisfactory clinical outcomes in the current study. The shared ACL bone tunnel technique is the simpler of the 2 procedures for combined LMPRT repair with ACLR.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221114319.
Footnotes
Acknowledgment
The authors acknowledge Ling Yan, MD, for assistance with this study.
Final revision submitted April 19, 2022; accepted May 17, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Third Affiliated Hospital of Zunyi Medical University (study No. 2018-029).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.