
Abstract
Background:
The Patient Acceptable Symptom State (PASS) cutoff is the value on a patient-reported outcome measure beyond which patients consider themselves to be “feeling well.” There are limited data regarding the PASS threshold for non-English versions of the International Knee Documentation Committee–Subjective Knee Form (IKDC-SKF).
Purpose:
To establish the PASS cutoff for the Thai version of the IKDC-SKF for patients undergoing primary anterior cruciate ligament reconstruction (ACLR) and to identify factors to achieve PASS after surgery.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Included in this study were patients aged 18 to 50 years who had undergone primary unilateral ACLR between January 2016 and February 2020. After enrollment, patients completed the Thai IKDC-SKF and answered the anchor question for determining the PASS.
Results:
Questionnaires were sent to 321 patients, of whom 173 (53.9%) responded. The vast majority (156 patients; 90.2%) considered themselves to have achieved the PASS. This group of patients had significantly higher IKDC scores than did those who did not have an acceptable symptom state (79.6 ± 14.2 vs 60.7 ± 16.5; P < .001). The receiver operating characteristic curve of the IKDC score for predicting the PASS had an area under the curve of 0.82 (95% CI, 0.72-0.91). The optimum PASS cutoff of the Thai IKDC-SKF was a score of 74.2 (sensitivity, 0.72; specificity, 0.82). Factors that provided favorable odds for achieving the PASS were the use of a hamstring tendon autograft (odds ratio, 4.1; 95% CI, 1.5-20.6) and the absence of a patellofemoral chondral lesion (odds ratio, 3.8; 95% CI, 1.03-14.1).
Conclusion:
For patients undergoing ACLR, the cutoff for the PASS of the Thai version of the IKDC-SKF was a score of 74.2. Two surgery-related factors provided favorable odds for achieving the PASS: the use of a hamstring tendon autograft and the absence of a patellofemoral chondral lesion.
Keywords
Clinical outcome assessments after anterior cruciate ligament (ACL) reconstruction (ACLR) can be divided into 4 categories: early adverse events, clinical measures of knee structure and function, ACL failure/recurrent disruption, and patient-reported outcomes (PROs). 20 The International Knee Documentation Committee–Subjective Knee Form (IKDC-SKF) is a knee-specific PRO measure used to evaluate patient perception of symptoms, function, and symptom-free sports activities. 8,12 It is commonly used to assess treatment outcomes after ACLR. 20,23 The IKDC-SKF has good psychometric properties and has been translated into other languages, including Thai. 7,8,13
The Patient Acceptable Symptom State (PASS) cutoff is the value for the global state on a PRO measure beyond which patients consider themselves to be “feeling well.” 22 The PASS cutoff signifies the score that denotes therapeutic success for individuals in a clinical setting. In research settings, it also demonstrates group results via the proportion of responders in each treatment arm. 6 Muller and associates 15 reported that the PASS threshold of the original version of the IKDC-SKF for patients who had undergone ACLR was a score of 75.9, with a sensitivity and specificity of 0.83 and 0.96, respectively. However, threshold values for the PASS assessed via different PRO measures vary, depending on patients’ general health, expectations, sociodemographic characteristics, and severity of injuries. 3,5
There are limited data regarding the PASS threshold for the non-English versions of the IKDC-SKF. The primary objective of the present study was to establish the PASS cutoff of the Thai version of the IKDC-SKF in patients who had undergone primary ACLR. The secondary objective was to identify the factors associated with an acceptable level of knee function after ACLR. It was hypothesized that the PASS cutoff for the Thai version of the IKDC-SKF in these patients could be identified using an anchor-based approach. Moreover, it was expected that the values for the Thai and the original English versions would be similar.
Methods
Study Design and Data Collection
This cohort study was performed at Siriraj Hospital, Bangkok, Thailand. The study protocol was approved by the hospital’s institutional review board, and all study participants provided written informed consent. We reviewed the hospital medical records to identify patients who had undergone primary unilateral ACLR between January 2016 and February 2020. Patients aged between 18 and 50 years at index surgery were included. The exclusion criteria were multiligament knee injuries; a history of ipsilateral knee surgery before the primary ACLR, fracture at the lower extremities, or contralateral knee injury; and an inability to communicate in Thai.
The eligible patients were contacted via telephone and invited to participate in the study. Three attempts were made to contact each patient. Potential participants were interviewed to assess their current Tegner activity level and history of reinjury in the same knee requiring medical attention or leading to an absence from sports participation exceeding 1 week. 19 Questionnaires, a consent form, and a stamped addressed return envelope were then dispatched to each potential participant. The questionnaires consisted of the Thai versions of the IKDC-SKF and the European Quality of Life–5 Dimensions–5 Levels (EQ-5D-5 L) Health Questionnaire. There was also an anchor question to determine the PASS. A reminder telephone call was made to each participant to improve the response rate.
All included patients had undergone anatomic single-bundle ACLR using either a bone–patellar tendon–bone (BPTB) or a hamstring tendon autograft. The surgeons counseled the patients regarding the risks and benefits of each graft type. The patients then selected their preferred graft choice. Details of the graft types, the associated intra-articular pathology, and the concomitant procedures for cartilage and meniscal lesions were collected, as were patient descriptive data, surgery data of the index surgery, repeat surgery on the knee, and ACL graft failure. Graft failure was defined as recurrent or persistent instability, pathological anterior or rotatory laxity, or failure evidenced via magnetic resonance imaging (MRI) scans. 20
PRO Measures
The Thai version of the IKDC-SKF is a knee-specific questionnaire with 18 items. 12,13 The summation of the scores for the individual items transforms into a final score ranging from 0 to 100. Higher scores represent higher levels of knee function and lower levels of symptoms.
The anchor question used to determine the PASS was: “Taking into account all the activities you have during your daily life, your level of pain, your activity limitations, and your participation restrictions, do you consider the current state of your knee satisfactory?” 6,15,21 The response could be either yes or no. The question was translated into Thai and pilot tested on 20 patients of the sports clinic of the hospital. It was found to be clear, with no pilot patient reporting any difficulty understanding it.
The Thai version of the EQ-5D-5 L is a generic, health-related, quality-of-life assessment tool. 11,16 It comprises 5 items that assess 5 aspects: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The calculated utility score ranges from 0 to 1. Higher scores indicate a better, health-related quality of life.
Statistical Analysis
Descriptive statistics were used to summarize the descriptive data. Categorical data were reported as frequencies and percentages. Normally distributed continuous data were presented as means and standard deviations, while nonnormally distributed continuous data were reported as medians and ranges. Differences among the 3 groups of eligible study participants (those with no contact details, nonresponders, and responders) were compared using 1-way analysis of variance, followed by the Bonferroni test or the Kruskal-Wallis test then the Mann-Whitney U test, as appropriate.
Differences between the participants who achieved the PASS (PASS-Y group) and those who did not achieve the PASS (PASS-N group) were analyzed using Student t test or the Mann-Whitney U test for continuous data and the chi-square test or Fisher exact test for categorical data. The Cochran-Mantel-Haenszel test was used to evaluate the overall ordered differences in the proportions of the Tegner activity levels of the groups.
A receiver operating characteristic curve was created to determine the cutoff that best distinguished PASS-Y from PASS-N. The optimum cutoff was estimated using the Youden index that created the maximal product of sensitivity and specificity.
Multiple logistic regression using the bootstrapping method was used to evaluate the associations between factors and the PASS achievement in patients who underwent ACLR. The statistical analyses were performed using PASW Statistics for Windows Version 18.0 (SPSS Inc). P < .05 was deemed statistically significant.
Results
Overall, 436 patients were eligible for this study after medical record review. Of these patients, 110 had no contact details. There were 5 patients who declined to participate; therefore, the questionnaires were sent to 321 participants. A total of 173 participants (53.9%) returned the questionnaires and were included in the study (Figure 1). The descriptive data of patients with no contact details, the nonresponders, and the responders are summarized in Table 1. The responders were significantly older than both the nonresponders (P < .001) and the patients with no contact details (P = .002). There was also a smaller proportion of men among the responders than the nonresponders (P = .004).

Study flowchart. PASS-Y, participants who achieved PASS; PASS-N, participants who did not achieve PASS. PASS, Patient Acceptable Symptom State.
Descriptive Data of Patients With no Contact Details, Nonresponders, and Responders

a Significantly different from the responders (P < .05).
b Significantly different from the nonresponders (P < .05).
c Significantly different from the patients with no contact details (P < .05).
Most of the respondents (156 patients; 90.2%) considered that they were in an acceptable symptom state (PASS-Y group). The descriptive data of the PASS-Y and PASS-N groups are detailed in Table 2. The average IKDC score of the 173 participants who responded to the questionnaire was 77.7 ± 15.4. The PASS-Y group had a significantly higher score than the PASS-N group had (79.6 ± 14.2 vs 60.7 ± 16.5; P < .001). In addition, the PASS-Y group had a higher EQ-5D-5 L score (0.98 ± 0.04 vs 0.91 ± 0.09; P = .007). Two patients had an ACL graft failure confirmed via MRI scans. Both subsequently elected to have conservative treatment, and they were satisfied with the current condition of their knees. Another 3 patients had repeat surgery on the index knee (a partial meniscectomy, debridement of soft tissue impingement, or debridement of chondral lesions). Surgery data by graft type, as well as associated injuries and concomitant procedures, are listed in Table 3.
Descriptive Data of Participants a
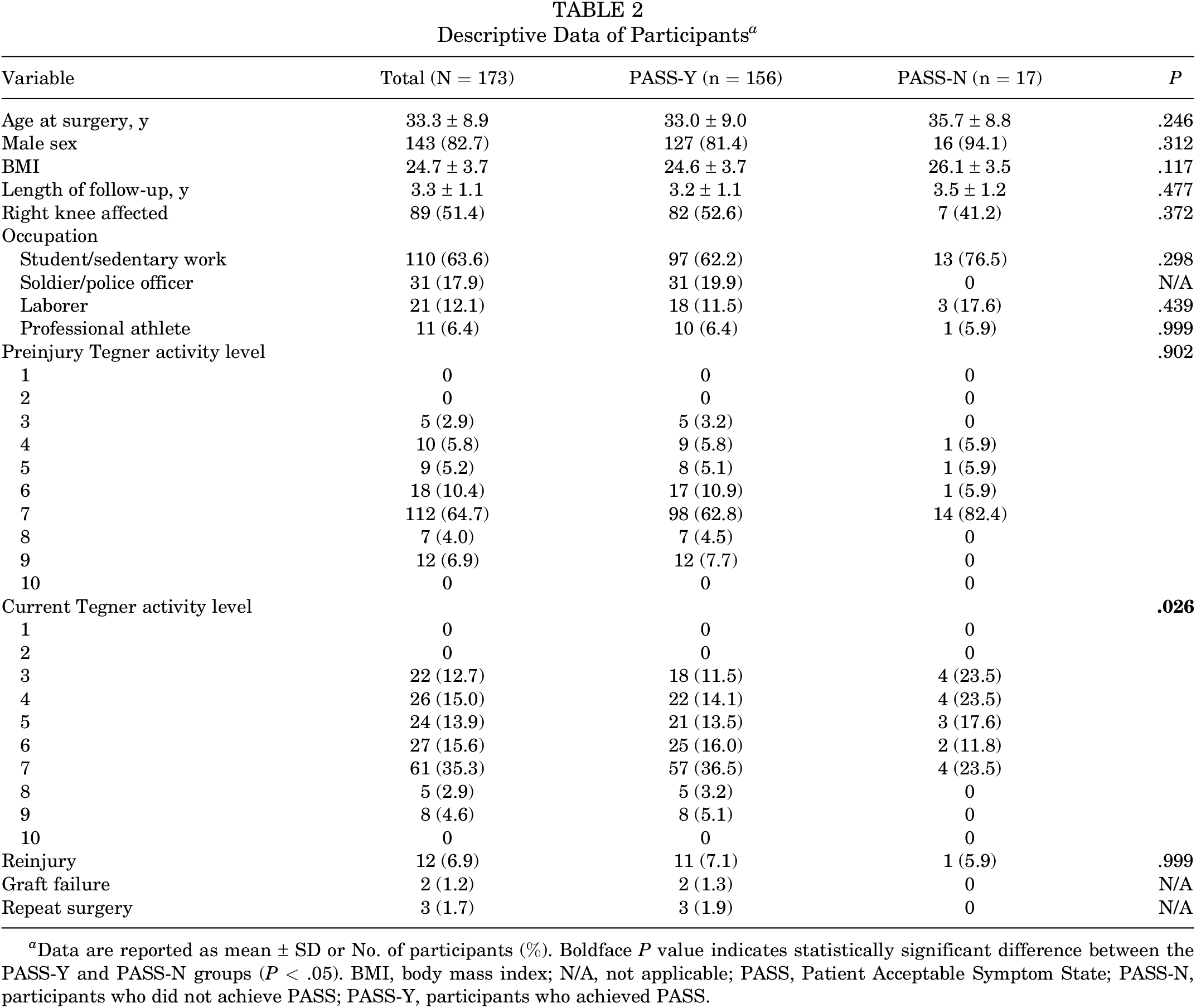
a Data are reported as mean ± SD or No. of participants (%). Boldface P value indicates statistically significant difference between the PASS-Y and PASS-N groups (P < .05). BMI, body mass index; N/A, not applicable; PASS, Patient Acceptable Symptom State; PASS-N, participants who did not achieve PASS; PASS-Y, participants who achieved PASS.
Surgical Data of Participants a
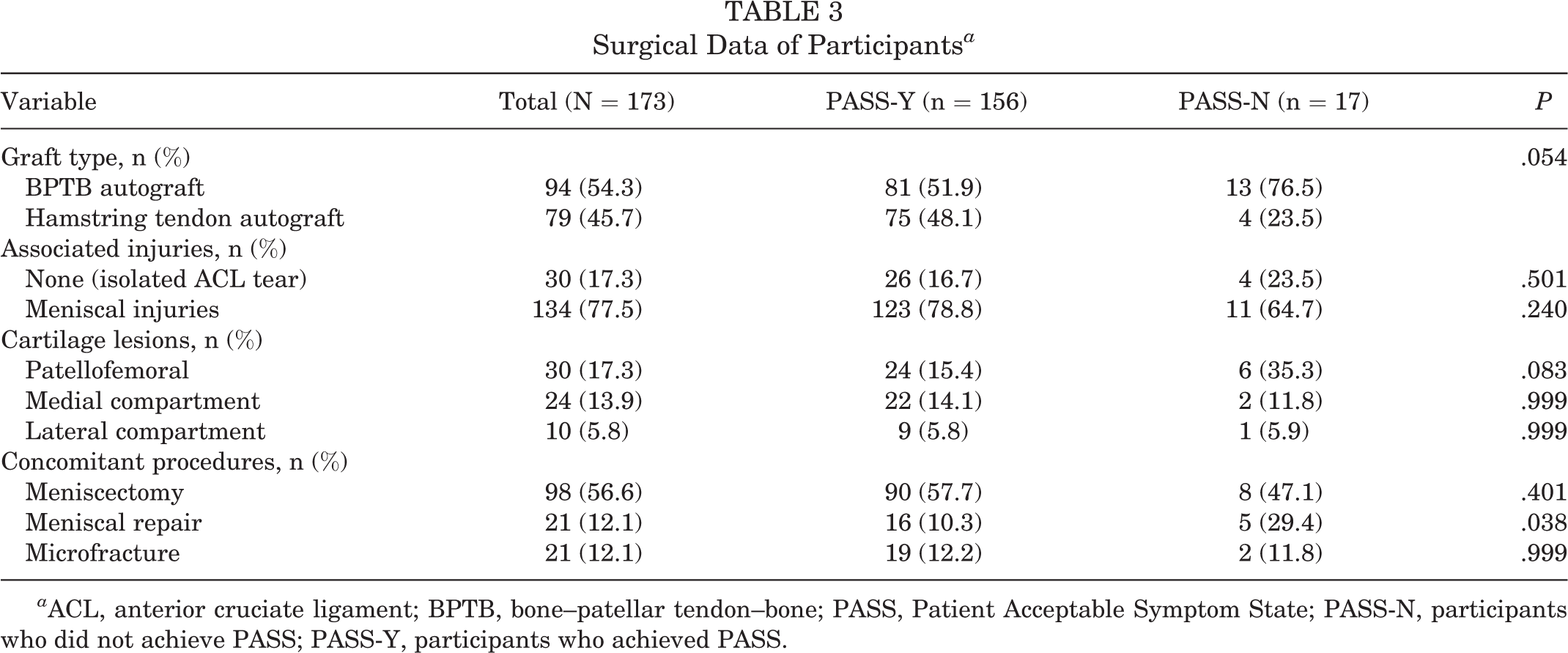
a ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; PASS, Patient Acceptable Symptom State; PASS-N, participants who did not achieve PASS; PASS-Y, participants who achieved PASS.
The receiver operating characteristic curve of the IKDC score for predicting the PASS in patients who underwent primary ACLR is illustrated in Figure 2. The area under the curve was 0.82 (95% CI, 0.72-0.91). Analysis of the curve indicated that the optimal cutoff for the Thai IKDC-SKF was a score of 74.2 (sensitivity, 0.72; specificity, 0.82). Table 4 displays the results of multiple logistic regression to determine the factors associated with achieving the PASS; 2 were identified. One was using a hamstring tendon autograft (odds ratio, 4.1; 95% CI, 1.5-20.6). The other was the absence of a patellofemoral chondral lesion (odds ratio, 3.8; 95% CI, 1.03-14.1).

Receiver operating characteristic curve of the International Knee Documentation Committee score for predicting Patient Acceptable Symptom State. AUC, area under the curve.
Factors Associated With PASS Achievement a
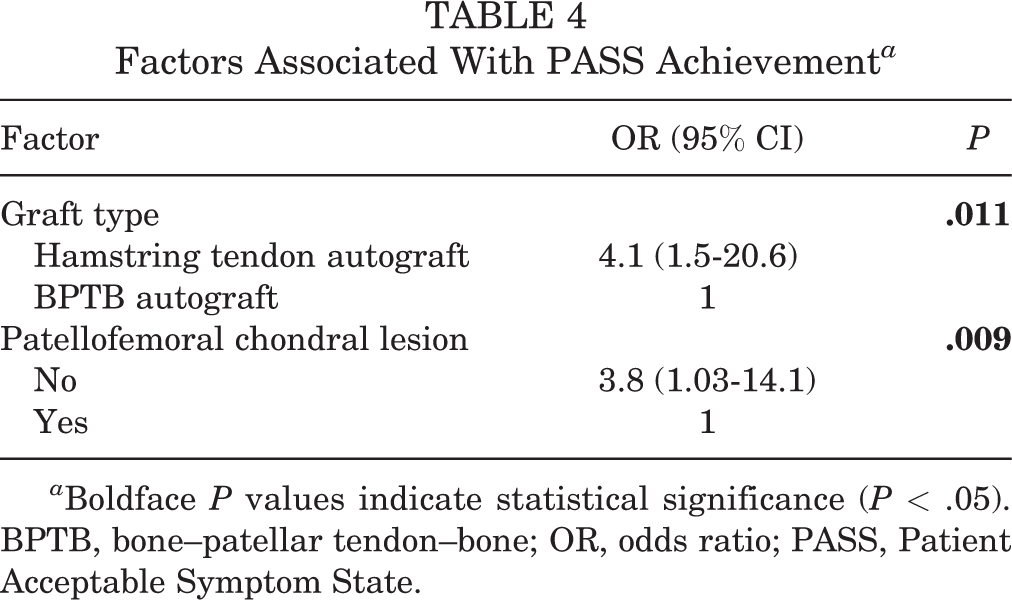
a Boldface P values indicate statistical significance (P < .05). BPTB, bone–patellar tendon–bone; OR, odds ratio; PASS, Patient Acceptable Symptom State.
Discussion
In this study, the PASS-Y group had higher mean IKDC and EQ-5D-5 L scores than the PASS-N group had. Therefore, the PASS question could distinguish patients with ACLR in terms of their level of satisfaction with their knee function and quality of life. A score of 74.2 was determined to be the optimal cutoff for the Thai IKDC-SKF in patients who had undergone primary ACLR, signifying the achievement of the acceptable symptom state. Two surgery-related factors were associated with the achievement of the PASS: the use of a hamstring tendon autograft and the absence of a patellofemoral chondral lesion.
The response rate in the present study was 53.9%. This proportion was very similar to the reported average response rate of 52.7% for survey data collected from individuals. 2 The mean age of the responders was older than that of the nonresponders. In addition, women represented 17.3% of the responders versus 6.8% of the nonresponders. A nonresponse analysis of 2-year data held by the Swedish National Knee Ligament Registry (which had a response rate of 52.0%) also found that older age and female sex improved the level of response. 17
The PASS was initially used to assess patients with rheumatological diseases. 21,22 The concept has recently been adopted to determine the clinical significance of PRO measures in patients with various knee conditions, such as ACL injuries, 15 meniscal tears, 6 and articular cartilage defects. 4 The PASS threshold values of the same PRO measure differ with the type of injury or disease condition being evaluated. 5 To illustrate, for patients with meniscal tears treated with arthroscopic partial meniscectomy, the PASS value of the IKDC-SKF was 58.5. 6 However, for patients who had undergone cartilage restoration procedures, the PASS threshold of the IKDC-SKF was 62.1. 4 The current study found that the PASS threshold of the Thai version of the IKDC-SKF for patients with ACLR was marginally lower than that of the original IKDC-SKF (74.2 vs 75.9, respectively). 15 With a cutoff of 75.9, the sensitivity decreased from 0.72 to 0.67, but the specificity was maintained at 0.82.
The proportion of participants who indicated that they had achieved the PASS was 90.2%. This level was very close to the 89.2% reported by Muller and coauthors. 15 Their research focused on patients who had undergone ACLR during the preceding 1 to 5 years, as did the current work. The proportion of patients achieving the acceptable symptom state could change over time. In an exploratory analysis of data from 2 randomized controlled trials with a mean follow-up of 16.4 years, one-half of the patients who underwent unilateral ACLR reported an IKDC score above the PASS cutoff. 9 Of those, 35% had radiographic osteoarthritis, with a Kellgren-Lawrence grade of 2 or more.
Awareness of the patient-related and surgery-related factors contributing to treatment outcomes after ACLR is beneficial for shared decision making by clinicians and patients. 10 A systematic review of the Scandinavian knee ligament registries demonstrated that younger age, male sex, nonsmoking, and receiving a hamstring tendon autograft were associated with superior PROs after ACLR. 10 In contrast, patients with concomitant meniscal and articular cartilage injuries reported inferior knee function compared with patients with isolated ACL tears. 10 In the present study, multiple logistic regression revealed that patients with a hamstring tendon autograft and those without a patellofemoral cartilage lesion had higher odds ratios for achieving the acceptable symptom state. A systematic review of overlapping meta-analyses revealed that, although BPTB autograft provided superior static knee stability, it produced a higher rate of anterior knee pain. 18 A systematic review of 7 prospective outcome studies with minimum 5-year follow-up comparing BPTB and hamstring autograft ACLR demonstrated no difference in clinical assessment, instrumented laxity, and PROs between these 2 graft choices. 14 However, a higher incidence of anterior knee pain or kneeling pain was reported in the group of patients who had ACLR with BPTB autograft. 14
Limitations
One limitation of this study was that its response rate of 53.9% was relatively low. There were also differences in the mean ages and sex distributions of the responders and nonresponders. These issues were encountered in other survey-based studies. 15,17 The original IKDC-SKF study by Muller et al 15 reported a similar response rate. This potential selection bias might have affected the findings of the present study. In addition, most participants were men. The male sex has been reported to have favorable odds for functional recovery after ACLR. 1 Last, there were no preoperative IKDC scores for the participants. Patients with a higher baseline score might be more likely to achieve an acceptable symptom state after treatment. This outcome has previously been found when using the IKDC-SKF to identify the acceptable symptom state in patients who underwent an arthroscopic partial meniscectomy. 6
Conclusion
For patients undergoing ACLR, the PASS cutoff for the Thai version of the IKDC-SKF was a score of 74.2. Two surgery-related factors provided favorable odds for achieving the PASS: using a hamstring tendon autograft and the absence of a patellofemoral chondral lesion.
Footnotes
ACKNOWLEDGEMENT
The authors gratefully acknowledge Miss Natthida Wisitwaranyu for data collection and Miss Narumol Sudjai for data collection and statistical analysis. They also thank David Park for his careful proofreading and professional English editing of this article.
Final revision submitted April 20, 2022; accepted May 17, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Siriraj Hospital (protocol No. 899/2563).