
Abstract
Background:
Patient-reported outcome measures are used to evaluate the functional status and assess the results after a medical intervention. For anterior cruciate ligament (ACL) reconstruction, the Lysholm scale is one of the most commonly used scales. The Patient Acceptable Symptom State (PASS) defines cutoff values for any patient-reported outcome measure, beyond which patients consider they have achieved an acceptable result. The PASS threshold for the Lysholm scale in patients undergoing ACL reconstruction has not yet been defined in the literature.
Purpose:
To define the thresholds of the PASS for the Lysholm scale in patients who have undergone ACL reconstruction with a follow-up of 2 to 5 years.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Patients who underwent isolated ACL reconstruction completed a survey during their last follow-up visit that included the Lysholm scale. All patients were asked to rate their satisfaction with their current health state by answering the following question: “Considering all the activities you perform as part of your normal daily life, your level of pain, and your degree of difficulty, if you were to remain in your current condition over the next few months, would you consider your current health state satisfactory?” Pre-, intra-, and postoperative variables were evaluated, and cutoff points for the Lysholm scale were established to discriminate the PASS using receiver operating characteristic (ROC) curves.
Results:
In total, 378 patients who underwent isolated ACL reconstruction with a mean follow-up of 35.8 ± 12.6 months were evaluated. Of these patients, 43 (11.4%) reported not being satisfied (PASS-No), while 335 patients (88.6%) reported being satisfied (PASS-Yes) after the procedure. The ROC curve identified a cutoff point of 85.0 points on the Lysholm scale (79.1% sensitivity, 90.7% specificity). Factors associated with failure to achieve the PASS threshold included greater preoperative knee hyperextension, postoperative residual pivot shift, new injuries, and subsequent ACL revision or meniscal surgeries on the operated knee.
Conclusion:
The PASS threshold for the Lysholm scale was 85.0 points for patients who had undergone ACL reconstruction, with a mean follow-up of 3 years. By establishing threshold values for the PASS, this study provides valuable insight to aid in the interpretation of the Lysholm scale in the clinical practice of ACL surgeons.
Keywords
Anterior cruciate ligament (ACL) injury is among the most common knee ligament injuries. 44 Approximately 200,000 ACL reconstruction surgeries are performed annually in the United States.14,44 The high interest in this injury arises from its frequent occurrence, particularly in sports. Anatomic ACL reconstruction is the most widely accepted treatment, especially for young and active populations. Although most patients experience satisfactory results, reconstruction failures and poor outcomes can still occur. A comprehensive assessment after ACL reconstruction should include clinical and instrumented joint laxity examination, functional performance tests, and subjective evaluation using patient-reported outcome measures (PROMs), providing a complete overview of the treatment outcome. 46 Clinical and instrumented measures of laxity indicate whether normal knee biomechanics have been reestablished. 4 Functional performance tests, such as isokinetic and hop tests, assess whether proprioception, muscle strength, and balance control are sufficient for a safe return to sport. 40 PROMs, in turn, reflect the patient's self-perceived functional condition. 28
Currently, the most commonly used functional scales for the subjective evaluation of ACL reconstruction outcomes are the Lysholm,6,36,48 International Knee Documentation Committee (IKDC), 2 and Knee injury and Osteoarthritis Outcome Score (KOOS) 41 scales. Although these are validated and standardized instruments for assessing patient function, it remains unclear whether a good postoperative score on a subjective scale accurately reflects the patient's overall satisfaction. To improve the assessment of subjective scales, alternatives such as measures of clinical relevance are increasingly being used. Among these are the minimal clinically important difference (MCID)/minimal clinically important improvement (MCII) and the Patient Acceptable Symptom State (PASS), which are key in evaluating changes in scores over the course of treatment and determining satisfaction thresholds.31,37,49
The Lysholm scale, widely used for the subjective assessment of ACL reconstructions, was created in 1985 by Lysholm and Tegner as an adaptation of other scales.36,48 The scale ranges from 0 to 100 points and is divided into 4 categories: 0 to 64 is considered poor, 65 to 83 is considered fair, 84 to 94 is considered good, and 95 to 100 is considered excellent. These score ranges were established empirically by the authors. A good surgical outcome is often associated with patient satisfaction, but this response is rarely recorded systematically. The PASS assessment addresses this gap by providing a standardized method of evaluation.29,37,49 The thresholds of the PASS for ACL reconstructions have already been validated for the IKDC and KOOS scales,5,34,53 but they have not yet been validated for the Lysholm scale.
The PASS assessment was created at Outcome Measures in Rheumatology (OMERACT) 6 in 2002. The MCID or MCII assessments were described at OMERACT 5 in 2000. These were compared in articles presented at OMERACT 7 in 2004 51 and OMERACT 8 in 2006, 50 evaluating patients with hip and knee osteoarthritis. These studies highlighted that, for patients, feeling good (PASS concept) is more important than feeling better (MCID/MCII concept). Thus, the objective of this study was to establish the PASS cutoff for the Lysholm scale for patients who underwent ACL reconstruction with a follow-up of 2 to 5 years. The secondary objective was to identify factors associated with patients who did not reach the PASS cutoff points. We hypothesized that the PASS cutoff values for the Lysholm scale would be higher than those previously established for the IKDC, which was 75.9.
Methods
This study was approved by the institutional review board of our institution, and informed consent form was obtained from all patients. This study was designed to establish the PASS cutoff value for the Lysholm Knee Scoring Scale in patients who underwent ACL reconstruction. Patients who underwent anatomic ACL reconstruction at our institution from 2018 to 2022 were evaluated. All surgeries were performed by 4 knee surgeons. Inclusion criteria included patients who underwent ACL surgery using the anatomic technique with independent femoral and tibial tunnels and patients aged 17 years or older with a closed growth plate, with no upper age limit. Patients with associated meniscal injuries were included in the study. Exclusion criteria included associated procedures such as osteotomies, peripheral ligament reconstructions, or cartilage procedures, and other previous surgeries on the ipsilateral or contralateral knee. Patients with <24 months of follow-up and those lost to follow-up were excluded.
All patients followed the same rehabilitation protocol. For patients who did not undergo meniscal repair, immediate partial weightbearing with 2 crutches was allowed and progressed as tolerated. Range of motion and quadriceps strengthening exercises were also initiated during the early postoperative period. For patients who underwent meniscal repair, an immobilizer was used for 4 weeks. Range of motion was restricted to 90° for 4 weeks and was then gradually progressed. Return to sport was allowed only after at least 8 months, provided the patients had a complete range of motion, a stable knee, no joint effusion, and good muscle strength.
Patients were always evaluated by knee surgeons or knee fellows from our institution. The preoperative physical examination was performed in the operating room with the patient under anesthesia, while the postoperative evaluation was conducted during regular follow-up visits, with the examiner blinded to the previous findings. Return visits for ACL reconstructions at our institution occur at 1 week, 3 weeks, 6 weeks, 3 months, 6 months, 12 months, and annually thereafter. Patients completed questionnaires containing their demographic data and preoperative and postoperative information. At the last follow-up visit, questionnaires included the Lysholm Knee Scoring Scale and the PASS question. Details related to the surgical procedure were collected from medical records.
The Lysholm Knee Scoring Scale consists of an assessment of 8 items: limping, support, locking, instability, pain, edema, stair climbing, and squatting, with closed-response alternatives. The final result is expressed both nominally and ordinally: 95 to 100 points is excellent, 84 to 94 points is good, 65 to 83 points is fair, and 64 or fewer points is considered poor.
The PASS assessment is based on the response to a single yes/no question: “Considering all the activities you perform as part of your normal daily life, your level of pain, and your degree of difficulty, if you were to remain in your current condition over the next few months, would you consider your current health state satisfactory?” Those patients who answered “yes” were named the PASS-Yes group, and those who answered “no” were named the PASS-No group.
Statistical Analysis
Qualitative parameters are described for all patients using absolute and relative frequencies, while quantitative parameters are described using measures of dispersion (mean, standard deviation, median, and quartiles). The PASS cutoff value for the Lysholm scale was determined using the receiver operating characteristic (ROC) curve. The association between the PASS categories and other qualitative characteristics was assessed using chi-square or exact tests (Fisher’s exact test or likelihood ratio test). Quantitative characteristics are described according to PASS categories and were compared using the unpaired Student t test. 26 The unadjusted odds ratios were estimated with their respective 95% confidence intervals for each variable of interest in the PASS category using bivariate logistic regression. 21
The test-retest reliability of the PASS question was determined in a separate cohort of 100 patients after 2 months of initial testing using the kappa correlation test.
IBM SPSS for Windows software Version 22.0 (IBM) was used to perform the analyses, and for data tabulation and graphing, Microsoft Excel 2013 software was used. The tests were performed with a significance level of 5%.
Results
A total of 776 patients were initially eligible, but 372 were excluded based on the exclusion criteria. Of these, 22 had previous surgery on the contralateral or ipsilateral knee and 350 required surgery alongside ACL reconstruction (anterolateral, posterolateral, or medial peripheral reconstructions, osteotomies, or cartilage procedures), leaving 404 patients. In total, 26 patients were lost to follow-up or had incomplete data, leaving 378 patients for the final analysis (Figure 1). The mean time from injury to ACL reconstruction was 5.8 ± 5 months, and the mean follow-up time was 35.8 ± 12.6 months.

Flowchart of the study sample.
Among the patients who answered the questionnaire, 100 were subject to a reliability test by answering the questionnaires again after 2 months. Of these 100 patients, only 1 changed their answer, resulting in a 99% agreement and a kappa of 0.6622. The characteristics of patients included in the study are detailed in Tables 1 and 2.
Demographic Characteristics and Preoperative Information of Patients Included in the Study (N = 378) a

Data are presented as n (%) unless otherwise indicated. p25, 25th percentile; p75, 75th percentile.
Pre-, Intra-, and Postoperative Characteristics of Patients Included in the Study (N = 378) a
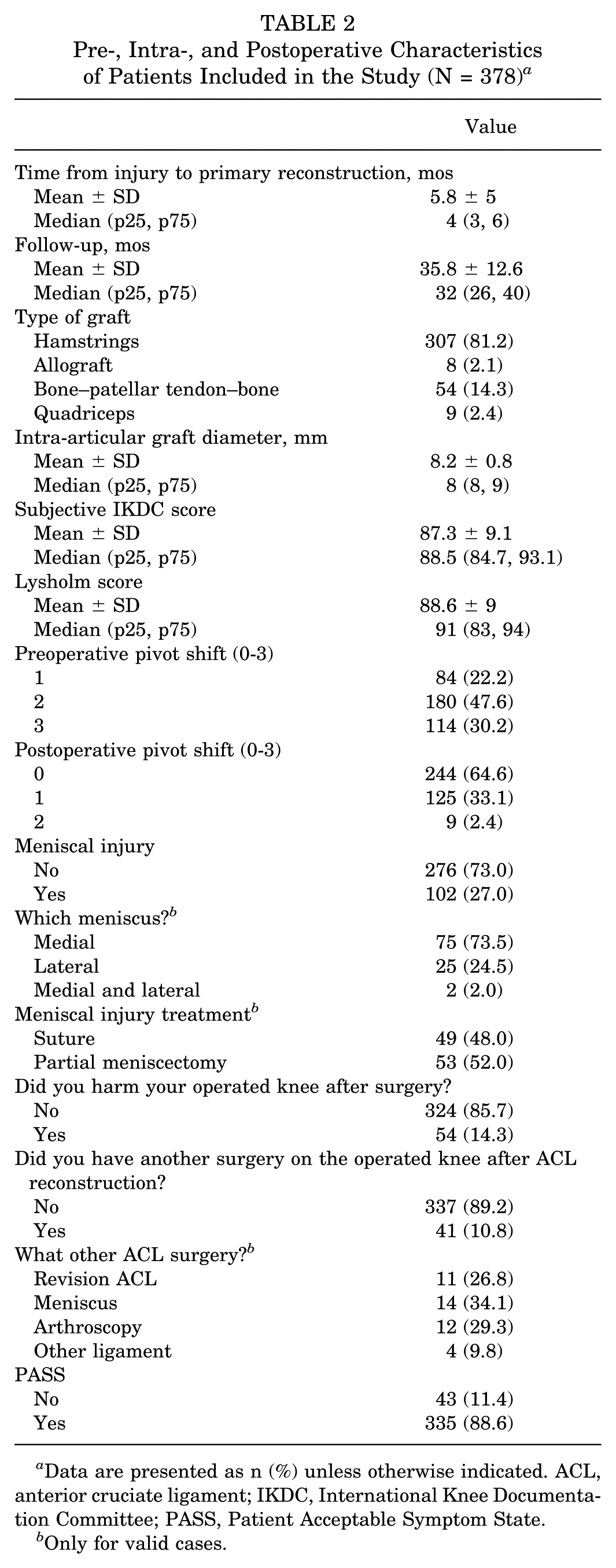
Data are presented as n (%) unless otherwise indicated. ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; PASS, Patient Acceptable Symptom State.
Only for valid cases.
PASS Assessment
A total of 335 (88.62%) answered “yes” (PASS-Yes), and 43 patients (11.4%) answered “no” (PASS-No). No statistically significant differences were found between groups with regard to age, sex, type of sport practiced, intensity of sports, or mechanism of trauma. Regarding the surgical procedure, the time from injury to surgery, type and diameter of the graft, presence of meniscal injury, and its treatment also did not differ between groups. The PASS-Yes group had lower mean knee hyperextension than the PASS-No group (3.9 ± 4.2 vs 6.0 ± 4.9; P = .008). In total, 294 patients were evaluated with pivot-shift grades 2 and 3 preoperatively. Postoperatively, no patients had grade 3, but 20.9% of patients in the PASS-No group had a grade 2 residual pivot shift, while none of the 335 patients in the PASS-Yes group had grade 2 or 3 residual pivot shift. The PASS-No group also had higher rates of subsequent injuries to the operated knee (PASS-Yes 9.6% vs PASS-No 51.2%; P < .001). Regarding subsequent surgical procedures, all 11 patients who underwent revision ACL reconstruction were in the PASS-No group, which also showed significantly higher rates of additional surgeries for meniscal injury treatment (PASS-Yes 2.7% vs PASS-No 11.6%; P = .001). No significant differences were observed between the PASS-Yes and PASS-No groups in terms of subsequent arthroscopies or other ligament reconstructions (Table 3). The mean Lysholm score was statistically higher in the PASS-Yes group compared with the PASS-No group (90.9 ± 5.3 vs 71.1 ± 12.2; P < .001). Finally, the ROC curve analysis established a cutoff point of 85.0 on the Lysholm scale for the PASS question, with a sensitivity of 79.1% and specificity of 90.7% (Table 4, Figure 2).
Pre-, Intra-, and Postoperative Characteristics of Patients According to PASS and Results of Unadjusted Analysis a

Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; PASS, Patient Acceptable Symptom State.
Only for valid cases.
Chi-square test unless otherwise indicated.
Unpaired Student t test.
Likelihood ratio test.
Fisher exact test.
AUC and Cutoff Point Established for PASS on the Lysholm Knee Scoring Scale a

AUC, area under the curve; PASS, Patient Acceptable Symptom State.
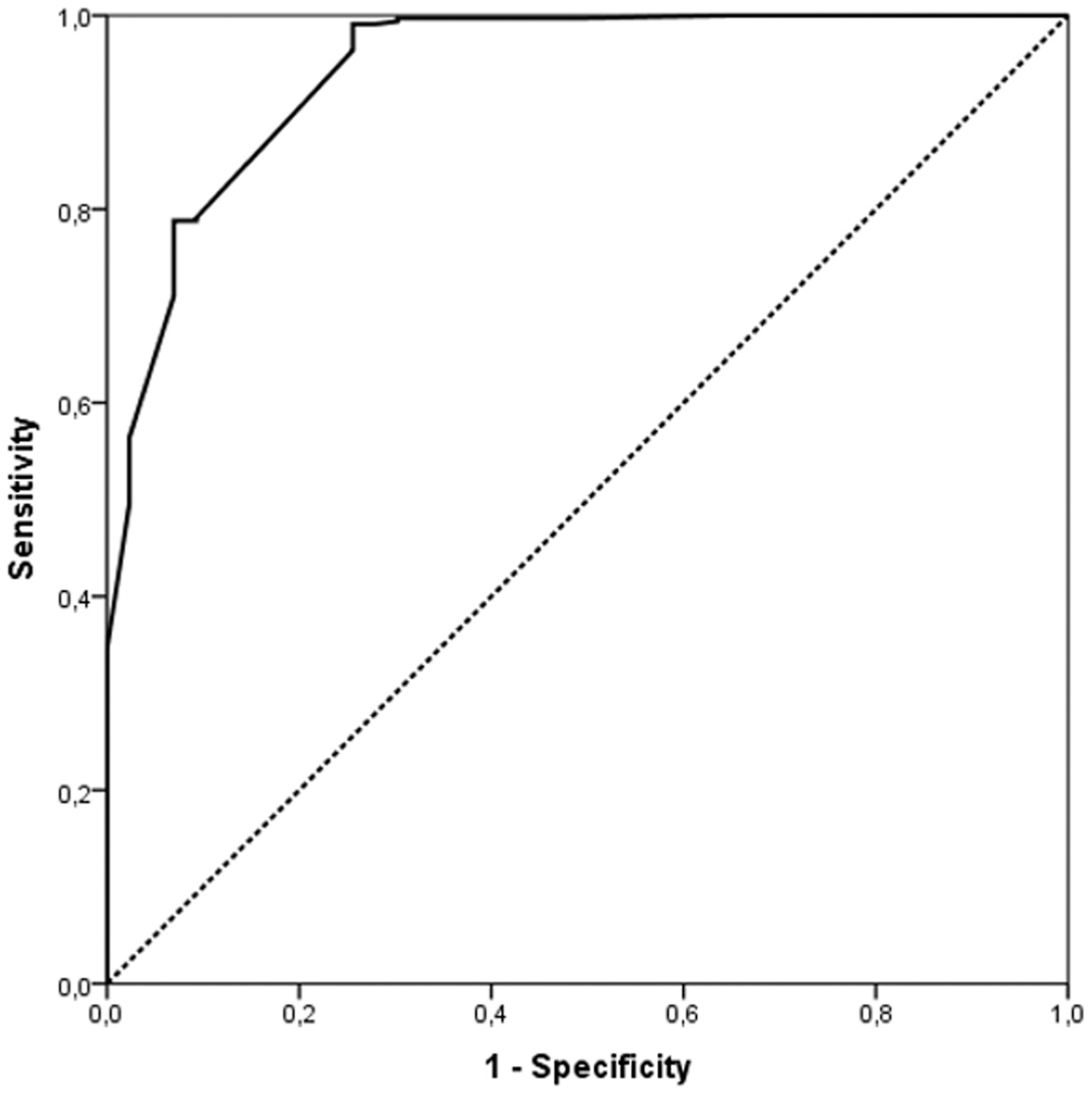
Receiver operating characteristic curve illustrating sensitivity versus 1 − specificity for the Lysholm Knee Scoring Scale in predicting the Patient Acceptable Symptom State, with an optimal cutoff value determined at 85.0 points.
Discussion
The main finding of this study was that the PASS cutoff point on the Lysholm scale for patients who underwent ACL reconstruction was 85.0, with a sensitivity of 79.1% and a specificity of 90.7%. Factors associated with failure to achieve this score included higher preoperative knee hyperextension, the presence of residual postoperative pivot shift, the occurrence of subsequent injuries to the operated knee, undergoing additional meniscal surgery on the operated knee, or undergoing revision ACL reconstruction.
PROMs are an important tool for assessing health outcomes, as they reflect the patient's perspective on the effect of treatment on their overall health and well-being. Abed et al 1 systematically reviewed randomized controlled trials studying patients with ACL reconstruction that utilized PROMs and found that the most commonly used were the IKDC (63.0%), Lysholm (60.2%), and Tegner (43.5%) scores. Muller et al 34 defined the PASS thresholds for the IKDC and KOOS scales in patients with ACL reconstruction, identifying a cutoff point of 75.9 for the IKDC scale (83% sensitivity and 96% specificity) and cutoff points for the KOOS subscales ranging from 57.1 (KOOS Symptoms) to 100 (KOOS Activities of Daily Living) after a mean follow-up of 40.8 months. In turn, Beletsky et al 5 studied an ACL reconstruction cohort at 6-month, 1-year, and 2-year follow-up points and found a PASS threshold of 75 points on the IKDC scale, with threshold values for the KOOS subscales ranging from 50 (KOOS Quality of Life) to 92.28 (KOOS Activities of Daily Living). In the long term, Urhausen et al 52 defined PASS thresholds for the IKDC and KOOS subscales at the 10-year follow-up after an ACL injury (including both nonoperative treatment and patients with ACL reconstruction), reporting a cutoff value of 76.2 points on the IKDC scale and cutoff values for the KOOS subscales ranging from 59.0 (KOOS Quality of Life) to 93.8 (KOOS Activities of Daily Living). To our knowledge, the present study is the first to define thresholds for the Lysholm Knee Scoring Scale, the second most commonly used PROM in patients undergoing ACL reconstruction, thus providing valuable insights for interpreting the Lysholm score in daily practice and clinical research on ACL reconstruction.
Compared with the PASS cutoff value for the IKDC score for patients with ACL reconstruction, 34 and considering that both scales range from 0 to 100 points, the threshold for the Lysholm scale was 9.1 points higher (75.9 and 85.0, respectively). Chahal et al 11 studied patients who underwent knee cartilage repair and found PASS cutoff values of 62.1 for the IKDC score and 70.0 for the Lysholm score (the Lysholm value was 7.9 points higher). Qiao et al, 38 in turn, studied recurrent patellar stability in patients who underwent medial patellofemoral ligament reconstruction and anterior tibial tubercle transfer and found PASS cutoff values of 73.2 for the IKDC scale and 75.5 for the Lysholm scale (the Lysholm value was 2.3 points higher). Liu et al 30 studied patients who underwent meniscal allograft transplantation and identified PASS cutoff values of 36.0 for the IKDC score and 66.5 for the Lysholm score (the Lysholm value was an impressive 30.5 points higher). Although there is variability among the values, which is likely related to differences in patient expectations for each procedure, the cutoff value for the Lysholm score was higher than that of the IKDC score across all previously studied knee procedures, consistent with the findings of our study.
Regarding our sample, the population of the present study had a mean age of 30 years and consisted of 73.8% men. However, age and sex were not significantly associated with a higher satisfaction index (PASS-Yes/No). Although the increased relative risk of ACL rupture in female patients is well established, the association between patient sex and subjective outcomes after ACL reconstruction presents conflicting data in the literature, with some studies showing worse subjective outcomes in females13,33,47 and others finding no differences.35,42 In a recent review, Branche et al 8 concluded that, overall, female patients exhibit worse self-reported outcomes, an increased risk of contralateral injury, and poorer results with hamstring grafts compared with bone–patellar tendon–bone and quadriceps tendon autografts. With regard to age, most studies that have investigated the outcomes of ACL reconstruction in younger and older patients, although showing lower postoperative levels of activity31,54 and poor quadriceps muscle strength recovery 18 in the older group, demonstrated no differences in subjective outcomes between groups.12,15,31,54 Saito et al, 43 however, showed inferior results on the IKDC scale in patients >40 years of age, although the other scores presented no differences. In turn, Cristiani et al, 13 with a large sample of 2335 primary ACL reconstructions, demonstrated that age <30 years and female sex consistently reduced the odds of achieving the PASS threshold in the KOOS subscales. Our study sample, however, may not have had the power to demonstrate those differences.
Factors associated with failing to achieve the PASS threshold in our study included greater preoperative hyperextension, higher postoperative residual pivot shift, sustaining new injuries to the operated knee, and undergoing subsequent meniscal surgeries on the operated knee. Revision ACL reconstruction appears to be a strong factor associated with failure to reach the PASS cutoff score, although statistical significance could not be evaluated, as all patients who underwent revision surgery were in the PASS-No group, with none in the PASS-Yes group. Beletsky et al 5 evaluated different parameters in their ACL reconstruction cohort and identified other factors influencing the odds of PASS achievement, including preoperative exercises, better preoperative scores, the association of iliotibial band tenodesis, and an anteromedial portal approach (instead of the transtibial approach) as positive factors, and workers’ compensation status as a negative factor.
Regarding the factors related to not achieving the PASS threshold in our study, patients who sustained new injuries or underwent revision ACL reconstruction or additional meniscal surgeries on the operated knee required prolonged rehabilitation, which may lead to worsened muscle condition and an increased risk of further meniscal and cartilage injuries. These factors may contribute to functional impairment and help explain the lower levels of patient satisfaction. Furthermore, revision ACL surgery alone is associated with worse outcomes compared with primary surgery.16,32
The residual pivot shift was another important factor related to patient dissatisfaction after ACL reconstruction. In our series, 33.1% of patients had a grade 1 residual pivot shift and 2.4% had a grade 2 residual pivot shift. Although this is a high rate, it is consistent with previous literature, considering that only isolated ACL reconstructions were performed (without the addition of a lateral extra-articular procedure such as anterolateral ligament reconstruction 39 or a modified Lemaire-type tenodesis 23 ) and that surgery was performed, on average, 5.8 months after the injury. Hurley et al, 22 in their meta-analysis, reported a residual pivot shift in 33.3% of patients who underwent isolated ACL reconstruction. Residual pivot shift is associated with poorer subjective functional outcomes3,27 and a higher likelihood of progression to osteoarthritis in the midterm. 24 Kawanishi et al 25 studied the factors related to residual pivot shift after primary ACL reconstruction and identified greater preoperative pivot shift, younger age, higher lateral posterior tibial slope, and concomitant ramp lesions as significant predictors of residual pivot shift. Dealing with patients who have these risk factors, the decision to add an extra-articular procedure may minimize the risk of residual pivot shift 22 and enhance patient satisfaction with the procedure.
Preoperative knee hyperextension was also a factor associated with lower satisfaction levels after ACL reconstruction. Sundemo et al, 45 in their systematic review, reported that generalized joint hypermobility leads to greater postoperative knee laxity and inferior PROMs after ACL reconstruction. Guimarães et al, 17 in turn, reported that patients who underwent ACL reconstruction with >5° of contralateral knee hyperextension had a higher failure rate and slight worsening in the Lysholm scale compared with those with <5° of hyperextension. Helito et al, 19 evaluating isolated ACL reconstructions using hamstring tendon graft, found that patients with >6.5° of hyperextension were 14.6 times more likely to experience reconstruction failure than patients with lower hyperextension. Additionally, Helito et al 20 reported that patients with knee hyperextension who do not fully recover their preoperative physiological knee hyperextension after ACL reconstruction, although presenting less residual knee laxity, show worse subjective functional scores and are less likely to achieve the PASS threshold for the IKDC score. Although postoperative hyperextension status was not deeply evaluated in the present study, this should be taken into consideration for future studies.
Finally, the Lysholm scale is a validated tool for evaluating and monitoring patients who have undergone ACL reconstruction, 9 and it is widely used in clinical practice and research on this topic.1,7 However, a high cutoff point on a functional scale raises some questions about whether it is suitable for patient assessment. The cutoff point for the PASS on the IKDC scale is 75.9, while the result obtained in this study for the Lysholm scale was 85.0, which is considerably higher. According to the Lysholm scale, a score ranging from 84 to 94 is considered good; however, a score of 84 is associated with PASS-No, based on the findings of the present study. Briggs et al 10 conducted a study with 488 healthy individuals with normal knee function (mean age, 41 years; range, 18-85 years) and found a mean Lysholm score of 94 points, instead of the maximal value of 100. Considering that the minimum detectable change for the Lysholm scale is 8.9 points, 9 the mean score of 94 points in individuals with normal knee function 10 is very close to the PASS cutoff value of 85.0 points found in our study. Given the factors mentioned above, a question arises as to whether the scale is sensitive enough to detect the changes that lead a patient to feel satisfied after ACL reconstruction surgery.
Limitations
This study has some limitations. First, the heterogeneity of our sample, including the male-to-female ratio (73.8%/26.2%), the inclusion of both acute and chronic injuries, and potential differences in rehabilitation among patients who underwent meniscal repair, could have impacted the overall results and patient satisfaction. In addition, some risk factors related to failure, such as bone morphology, intercondylar size, limb axis, and posterior tibial slope, were not evaluated and may serve as confounding factors, as could the patients’ preoperative body mass index, which was not reported and may differ between groups. Additionally, although the same technique (outside-in with interference screw fixation for the femur and tibia) was used, the fact that surgeries were performed by 4 different knee surgeons, each with potentially slight differences in technique, may have introduced some bias. Lastly, some patients were lost to follow-up, and their missing data could also affect the cutoff point.
Conclusion
The PASS threshold for the Lysholm scale was 85.0 points for patients who had undergone ACL reconstruction, with a mean follow-up of 3 years. Factors associated with failure to achieve the PASS cutoff value include greater preoperative knee hyperextension, presence of residual postoperative pivot shift, occurrence of new injuries to the operated knee, and subsequent revision ACL or meniscal surgeries on the operated knee.
Footnotes
Final revision submitted July 16, 2025; accepted August 1, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Institutional Review Board of the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo.