
Abstract
Background:
Given the lack of established, externally validated criteria for the diagnosis of unstable hips, the Femoro-Epiphyseal Acetabular Roof (FEAR) index has been proposed as a useful tool for identifying hips with instability in the setting of borderline acetabular dysplasia.
Purposes:
To (1) determine the external performance of the FEAR index in identifying hips with a clinical diagnosis of instability in the setting of borderline dysplasia and (2) assess the performance of the FEAR index compared with acetabular inclination or physeal scar angle alone.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The authors reviewed 176 patients with borderline acetabular dysplasia (lateral center-edge angle, 20°-25°). A positive FEAR index was defined as ≥5°. An alternative threshold ≥2° was also assessed. Significant instability was determined by the senior surgeon based on the combination of patient and radiographic features; unstable hips were treated with periacetabular osteotomy (with or without hip arthroscopy), and stable hips were treated with isolated hip arthroscopy.
Results:
Only 18% of borderline hips had a positive FEAR index. The ≥5° positive FEAR index threshold had a sensitivity of 33% (23/70) and specificity of 92% (98/106) in predicting the clinical diagnosis of instability. The ≥2° FEAR index threshold had a sensitivity of 39% (27/70) and specificity of 89% (94/106) in predicting the clinical diagnosis of instability. No alternative threshold for the FEAR index resulted in high levels of sensitivity and specificity. A threshold of –5° was required to reach an adequate sensitivity of 74%. The FEAR index remained a significant predictor of hip instability even after controlling for acetabular inclination (odds ratio, 1.12; P < .001) or physeal scar angle (odds ratio, 1.6; P < .001).
Conclusion:
In the current study, a positive FEAR index was generally indicative of the presence of clinical instability, but the FEAR index alone remained inadequate to fully define the instability of a given hip, as it demonstrated low sensitivity (only 33%) in the external validation. The FEAR index is best used in the context of other clinical and radiographic features.
Patients with borderline acetabular dysplasia remain a challenging population to differentiate significant instability from impingement. 14,19,25 Borderline acetabular dysplasia is classically defined as a lateral center-edge angle (LCEA) between 20° and 25°, while values between 18° to 28° are commonly used. Thomas et al 26 demonstrated that the risk of osteoarthritis extends up to an LCEA of 28° in a female population. This risk may be partially due to instability in this population but also partially due to the femoroacetabular impingement (FAI) in this population. 22 Borderline acetabular dysplasia is extremely common; Kapron et al 10,11 demonstrated a 46% prevalence in women and 19% in men. A recent systematic review demonstrated a prevalence of borderline dysplasia of approximately 20%, which is 3.5 times more common than classic acetabular dysplasia. 7 Decision making in the patient with symptomatic borderline dysplasia between isolated hip arthroscopy (for treatment of FAI) or periacetabular osteotomy (PAO) with or without hip arthroscopy (for treatment of instability) is a common dilemma. 19 Treatment decisions in the setting of borderline acetabular dysplasia are challenging given the lack of established, externally validated criteria for the diagnosis of unstable hips. Radiographic parameters such as acetabular inclination (AI) (or Tönnis angle) have been commonly used but alone appear to be inadequate. However, investigating the utility of clinical diagnosis tools across different surgeons is an important step to improve our understanding.
The Femoro-Epiphyseal Acetabular Roof (FEAR) index has been proposed as a useful tool in identifying hips with instability in the setting of borderline acetabular dysplasia and is becoming increasingly used in multiple settings. 24,27 –29 Wyatt et al 29 defined the FEAR index as the angle between a line connecting the most medial and lateral parts of the sourcil and a line connecting the most medial and lateral parts of the straight central third of the femoral head physeal scar. In the original study, FEAR was internally validated in a mixed cohort (mean LCEA, 13.7°) of classic acetabular dysplasia (LCEA, <20°) and borderline acetabular dysplasia (LCEA, 20°-25°), which may increase its sensitivity and specificity and not reflect performance in the setting of borderline dysplasia alone. A positive FEAR index is present when the resulting angle opens laterally to ≥5°. The FEAR index, by definition, is also the difference between AI and the physeal scar angle. In this original study by Wyatt et al, the authors observed that a FEAR index of 5° threshold can accurately distinguish unstable versus stable hips with 79% accuracy, 78% sensitivity, and 80% specificity. A subsequent study by this group (Batailler et al 2 ) suggested that plain radiographs were superior to magnetic resonance imaging for assessment of FEAR and suggested that an optimal threshold of 2° had a 90% predictive ability. However, this cohort included no hips with an LCEA >20°, which likely influenced the predictive ability.
It is important to note that, given no validated criteria for the gold standard diagnosis, the assessments in the studies of Wyatt et al 29 and Batailler et al 2 used the surgeon diagnosis using nonvalidated radiographic criteria: increased distance from the femoral head to the ilioischial line, recentering on the anteroposterior abduction view, break in the Shenton line, or crescent-shaped accumulation of gadolinium in the posteroinferior joint space on magnetic resonance angiography (MRA) scans. However, given the lack of validated criteria, the entire literature on borderline dysplasia is similarly limited by single-surgeon diagnosis or nonvalidated criteria. Further evaluation of the external validity of the FEAR index in a cohort with only borderline acetabular dysplasia is needed.
The purposes of the current study were to (1) determine the external performance of the FEAR index in identifying hips with a clinical diagnosis of instability in the setting of borderline dysplasia and (2) assess the performance of the FEAR index compared with AI and the physeal scar angle alone.
Methods
The current study was a retrospective review of patients who underwent surgical treatment of hip disorders in the setting of borderline acetabular dysplasia by a single surgeon (J.C.C.) between January 2008 and April 2017. The study protocol was approved by our institutional review board and included consent of eligible patients. We initially identified 386 patients via prospectively collected radiographic measurements in a hip preservation database. Standing anteroposterior pelvis radiographs were taken with the feet placed a shoulder width apart according to previously described standardized protocols. 5 Inclusion criteria were an LCEA of 20° to 25° and age between 14 and 40 years. Patients were excluded for the following reasons: age >40 or <14 years (n = 62); hip osteoarthritis of Tönnis grade ≥2 (n = 4); prior ipsilateral hip surgery (n = 64); and residual deformities from slipped capital femoral epiphysis, Legg-Calve-Perthes disease, or other conditions (n = 70). After exclusion criteria were applied, 186 remained in the cohort.
Demographic and radiographic measurements were recorded. The primary clinical diagnosis (and treatment decision) of a single experienced surgeon (J.C.C., based on combined patient and radiographic factors) was used to determine the presence or absence of significant instability (Table 1). The surgeon had >20 years of experience in hip preservation surgery, including hip arthroscopy and PAO. The primary clinical diagnosis without instability (generally associated with FAI) led to treatment with hip arthroscopy, while the clinical diagnosis with instability led to treatment with PAO with or without hip arthroscopy. No specific criteria were used for diagnosis given the lack of any validated criteria existing.
Patient and Imaging Factors Influencing Decision Making in Patients With Borderline Acetabular Dysplasia a
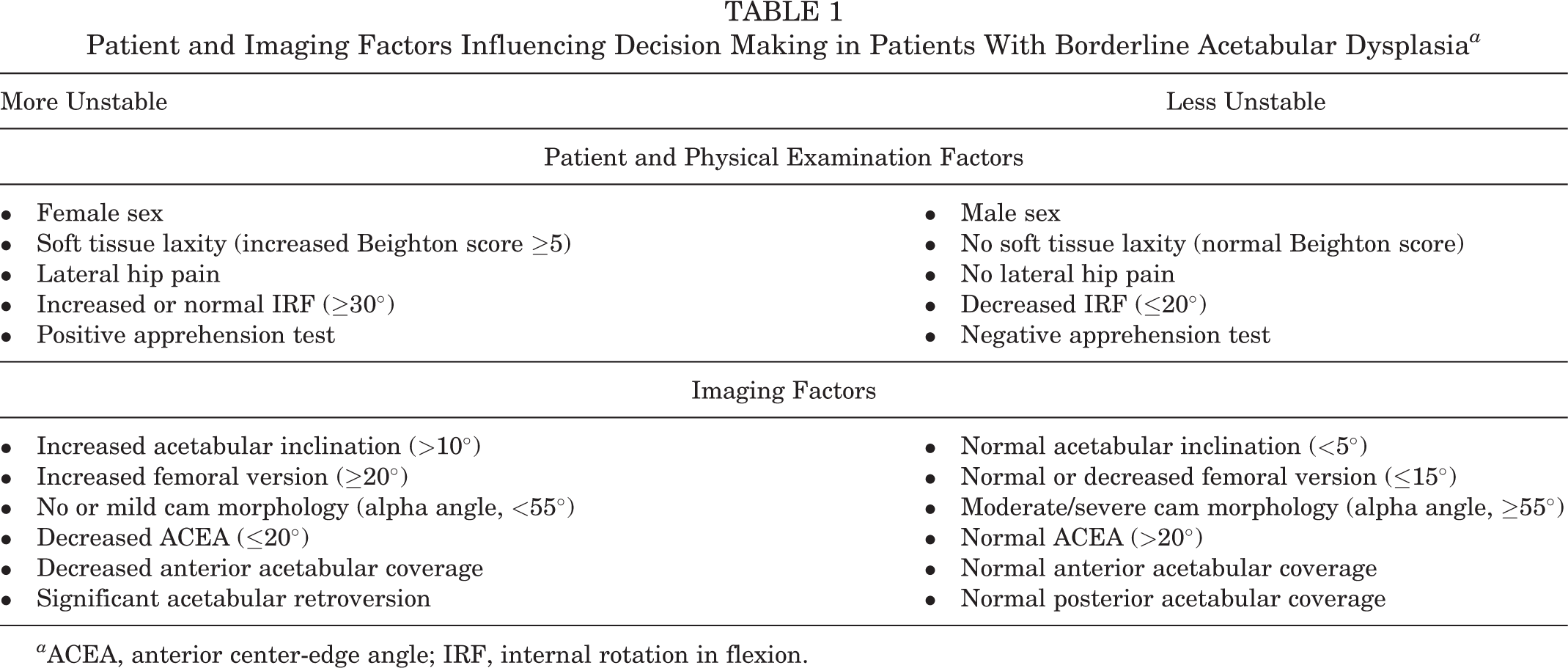
a ACEA, anterior center-edge angle; IRF, internal rotation in flexion.
Radiographic analysis was performed by a single experienced research fellow (M.T.S.) with established reliability and included measurement of the FEAR index, as well as the LCEA, AI, physeal scar angle (measured relative to horizontal), 20 and anterior center-edge angle (ACEA). The FEAR index is equivalent to AI minus the physeal scar angle (FEAR = AI – Physeal scar angle) (Figure 1). A value ≥5° was used to indicate a positive FEAR index, and <5° indicated a negative FEAR index, as described by Wyatt et al. 29 In addition to the 5° threshold for positive FEAR index, we assessed alternate threshold values of the FEAR index from –5° to 10°, including the 2° threshold. 2
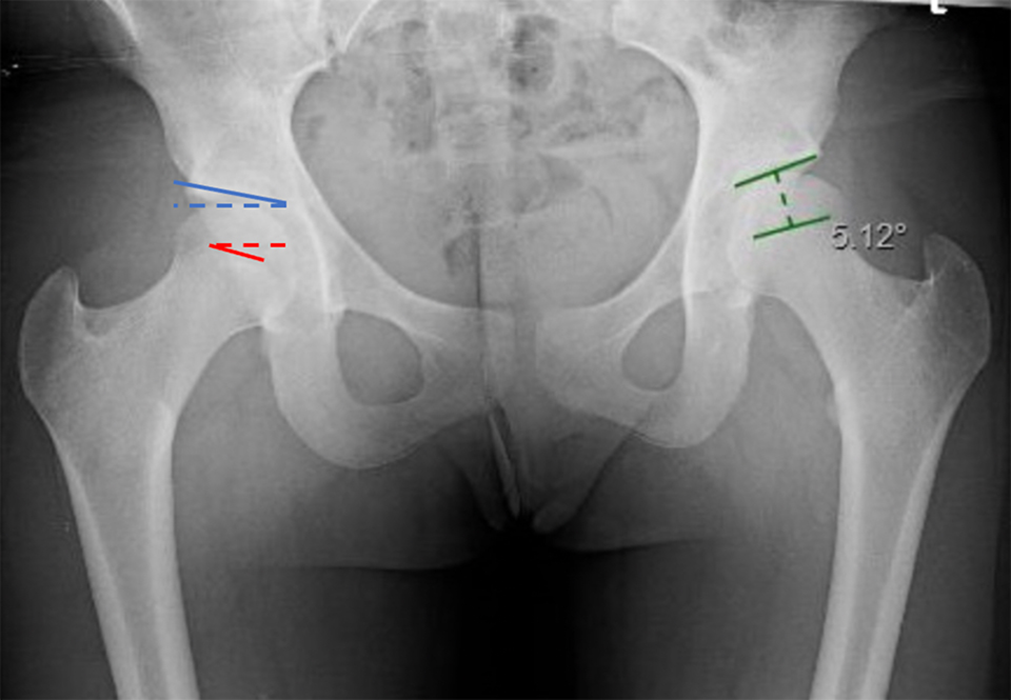
Case example of Femoro-Epiphyseal Acetabular Roof index (green lines) of 5.12° in a left hip. The FEAR index is the angle formed between the acetabular sourcil (acetabular inclination, blue lines) and physeal scar angle (red lines) shown in the right hip.
The intra- and interobserver reliabilities of the FEAR index have been previously established but were also assessed in our study in a subset of 20 patients using the intraclass correlation coefficient (ICC). Intraobserver reliability was assessed by the primary reader (M.T.S.), with 2 reads separated by >2 weeks, and interobserver reliability was assessed relative to a second experienced radiographic reader.
Statistical Analysis
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the various threshold values of the FEAR index to predict the primary clinical diagnosis of instability. A t test was used to assess the association of the LCEA, AI, and physeal scar angle with the FEAR index. Additionally, the Pearson correlation coefficient (r) was calculated for the association between the AI, physeal scar angle, and FEAR index. A bivariate analysis was used to assess the significance of the FEAR index relative to AI and the physeal scar angle in predicting instability. The threshold for statistical significance was set at P < .05. All analyses were performed using SAS Version 9.4 (SAS Institute Inc., Cary, NC).
Results
Of the 186 patients who were included, the FEAR index was unable to be assessed in 5.4% (10/186) of hips because of the inability to visualize the proximal femoral physeal scar; thus, the remaining 176 patients were included in the remainder of the study. Of this cohort, 74% (131/176) were women, the mean age was 24.8 ± 7.9 years, and the mean body mass index was 23.3 ± 3.5. The reliability of measurement of the FEAR index was assessed with an intraobserver reliability of ICC = 0.97 and interobserver reliability of ICC = 0.88, indicating good to excellent agreement. The reliability of the threshold used to define the FEAR index (≥5° vs <5°) was ICC = 0.79, indicating good agreement.
Of the final cohort of 176 hips, 40% (70/176) were diagnosed as unstable (treated with PAO with or without hip arthroscopy), and 60% (106/176) were diagnosed as stable (treated with isolated hip arthroscopy). The mean FEAR index in the entire cohort was –4.3° ± 8.1° (range, –29.4° to 17.5°). Overall, 18% (n = 31) of hips were FEAR-positive (FEAR index, ≥5°), while 82% (n = 145) were FEAR-negative (FEAR index, <5°). For FEAR-positive hips, the mean FEAR index was 7.6° ± 2.8° (range, 5.1°-17.5°), compared with –6.9° ± 6.4° (range, –29.4° to 3.7°) for FEAR-negative hips. No significant difference in the mean LCEA was seen between FEAR-positive and FEAR-negative hips (21.9° ± 1.5° vs 22.4° ± 1.4°; P = .068). Similarly, no significant difference in the mean ACEA was seen between FEAR-positive and FEAR-negative hips (23.3° ± 5.7° vs 25.3° ± 6.5°; P = .122). The mean AI was significantly higher in FEAR-positive (AI mean, 11.2° ± 3.6°) compared with FEAR-negative (AI mean, 9.5° ± 2.9°) hips (P = .005). The mean physeal scar angle was decreased in FEAR-positive (3.6° ± 4.3°) compared with FEAR-negative (16.4° ± 6.5°) hips (P < .001).
Using the 5° threshold, we observed that the FEAR index had a sensitivity of only 33% (23/70) but a specificity of 92% (98/106) (PPV, 74% [23/31]; NPV, 68% [98/145]) (Figure 2). Thus, 47 of the 70 (67%) hips diagnosed as unstable were FEAR-negative. Figure 3 shows examples of unstable hips with a positive and a negative FEAR index using this threshold. Similarly, the 2° FEAR index threshold had a sensitivity of only 39% (27/70), specificity of 89% (94/106), PPV of 69% (27/39), and NPV of 69% (94/137) in predicting the clinical diagnosis of instability. For both the 2° and 5° thresholds, the overall predictive ability in this cohort was 65%. No alternative threshold for the FEAR index resulted in high levels of sensitivity and specificity. A threshold of –5° was required to reach an adequate sensitivity of 74%.
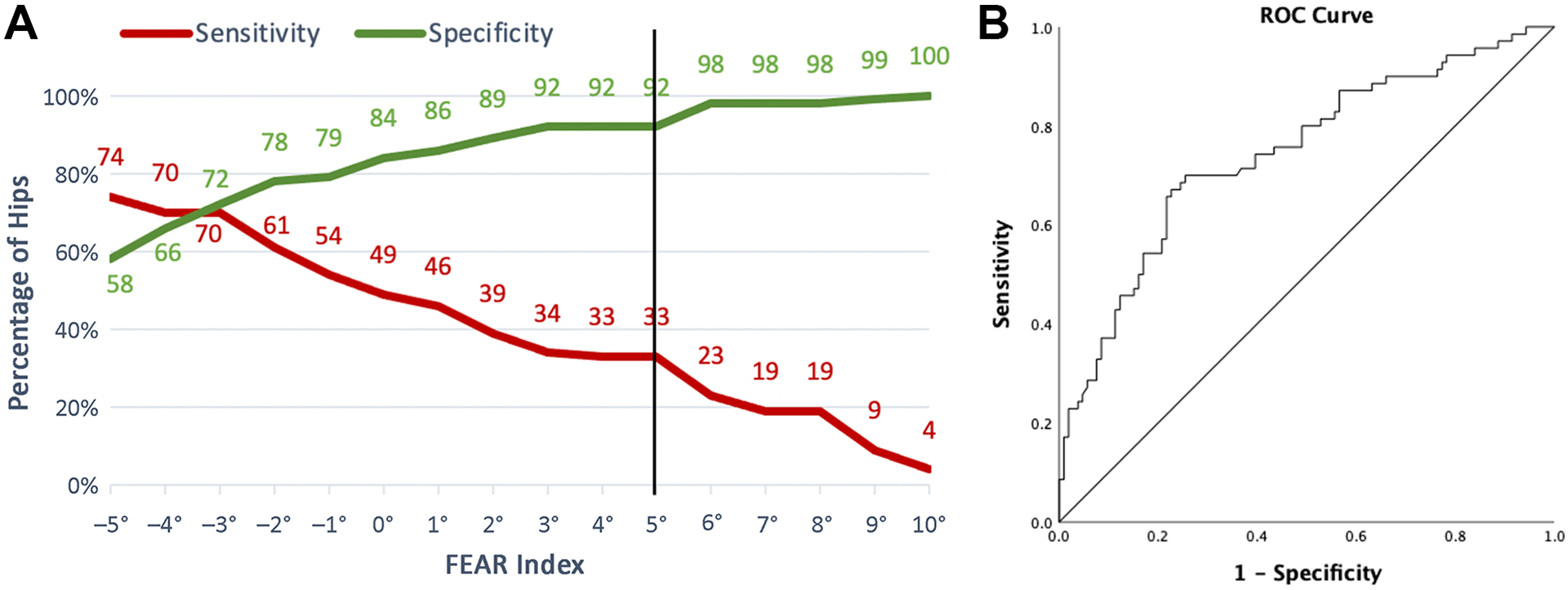
(A) Sensitivity and specificity of different threshold values for the Femoro-Epiphyseal Acetabular Roof (FEAR) index and (B) associated receiver operating characteristic (ROC) curve.
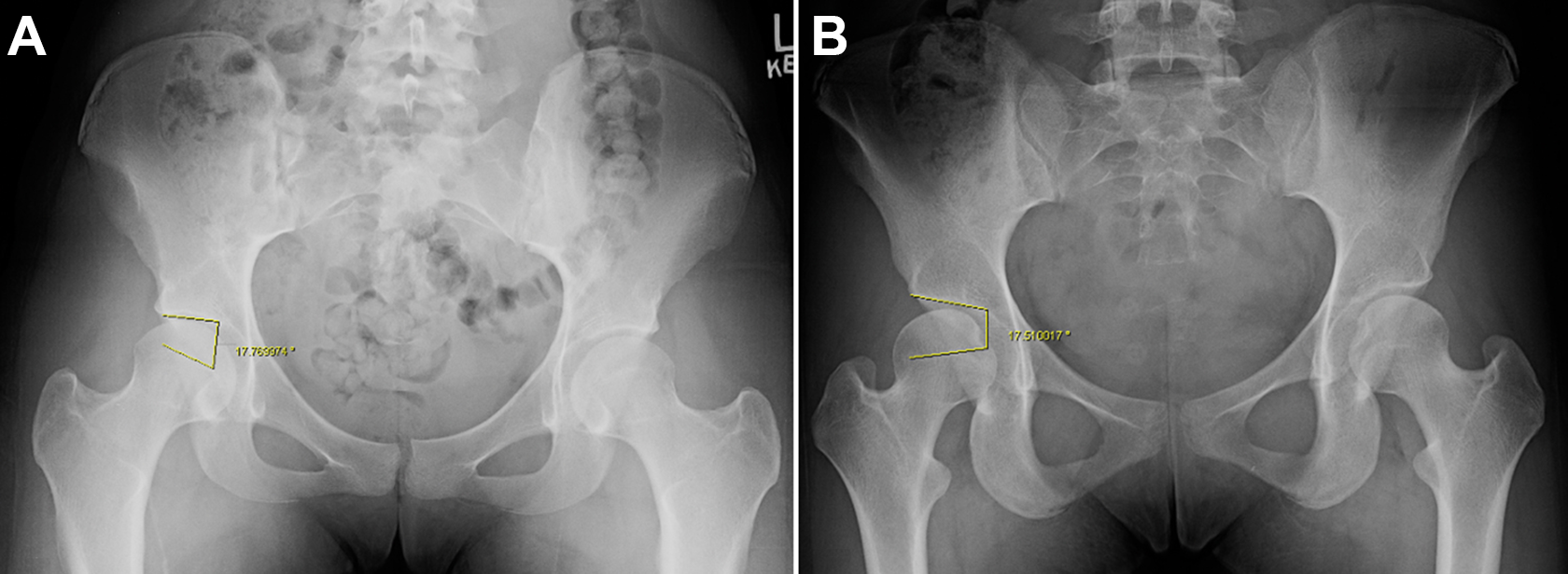
Two case examples of hips with clinical diagnosis of instability: (A) Femoro-Epiphyseal Acetabular Roof (FEAR) index <5° (FEAR-negative) and (B) FEAR index ≥5° (FEAR-positive).
Of the entire cohort, 45% (80/176) had a FEAR index <–5°, 26% (45/176) had a FEAR index from –5° to 0°, 11% (20/176) had a FEAR index from 0° to 5°, and 18% (31/176) had a FEAR index ≥5°. The predictive ability of different FEAR index thresholds is shown in Figure 2. The sensitivity decreased greatly at 10° to 4%, and the specificity increased to 100%. At the 0° threshold, the sensitivity increased to 49%, and the specificity decreased somewhat to 84%. A threshold of –5° was required to reach an adequate sensitivity of 74% but had an associated specificity of only 58%. The area under the receiver operating characteristic curve was 0.74.
The mean AI in the group was 9.8° ± 3.1° (range, 2.5°-18.8°). Of the entire cohort, 0% (0/176) had an AI <0°, 57% (101/176) had an AI from 0° to 10°, and 43% (75/176) had an AI ≥10°. Comparatively, looking at AI using a 10° threshold, we found that AI alone had a sensitivity of 68% and a specificity of 72%. Using a 15° threshold, we observed that the sensitivity of AI decreased to 11% and the specificity increased to 100%.
There was a strong negative correlation between the FEAR index and the physeal scar angle (r = –0.93; P < .0001) and a weak positive correlation to AI (r = 0.26; P < .001) (Figure 4). A bivariate predictive model was used to determine the significance of predictors after controlling for other parameters. After controlling for AI, we observed that the FEAR index remained a significant predictor of hip instability (Odds Ratio, 1.12; P < .001). Similarly, after controlling for the physeal scar angle, we observed that the FEAR index remained a significant predictor of hip instability (Odds Ratio, 1.6; P < .001). Thus, the FEAR index remained a significant predictor beyond the role of AI or the physeal scar angle alone.

Correlation of the Femoro-Epiphyseal Acetabular Roof (FEAR) index with acetabular inclination (AI) and physeal scar angle.
Discussion
Decision making in the population of patients with borderline acetabular dysplasia between isolated hip arthroscopy (stable hips) and PAO with or without hip arthroscopy (unstable hips) is a common dilemma given the 20% prevalence of borderline acetabular dysplasia in the general population. 7 In the current study, we assessed the external validity of the FEAR index in a large cohort of patients (n = 186) with borderline acetabular dysplasia who underwent surgical treatment. In our study, a positive FEAR index (5° threshold) was generally indicative of the presence of clinical instability (PPV, 74%), but the FEAR index was poorly sensitive (33%) to hip instability (with 67% hips diagnosed with instability being FEAR-negative). At the 2° FEAR index threshold, similar limitations in predictive ability were seen. The overall predictive ability of either the 2° or 5° FEAR threshold was only 65% in the current study, compared with the 90% predictive ability reported in previous studies that include classic acetabular dysplasia. 2,29 This 65% value is only marginally better than chance alone (50%) or predicting no instability in all patients (60%). Additionally, we demonstrated that the FEAR index does still have predictive ability in identifying instability in this population beyond that of AI but is best used in combination with other radiographic parameters rather than in isolation.
The optimal treatment strategy for borderline hip dysplasia is a major controversy in hip preservation. The results of surgical treatment of borderline dysplasia are good, but up to 30% to 50% of patients have had suboptimal outcomes in some studies. 1,6,8,12,18 Similarly, the results of PAO in this population have more recently demonstrated good outcomes in a well-selected subgroup of patients. 4,13,21 Thus, the diagnosis of significant instability that may require a PAO is a critical determination to optimize patient outcomes. Zimmerer et al 30 reported outcomes of arthroscopic treatment of 36 hips with borderline acetabular dysplasia and found poor outcomes in the setting of 2 of 4 radiographic subgroups. Poor outcomes were seen in the “stable posterolateral deficiency” cluster (FEAR, <2°; posterior wall index, <0.85), with nearly 80% having a suboptimal outcome. This group was the largest of the 4 subgroups. Additionally, marginal outcomes were seen in the “unstable anterolateral deficiency” cluster (FEAR, >2°; anterior wall index, <0.35), with nearly 40% having suboptimal outcomes. This study highlighted how the use of the FEAR index in isolation may not be adequate. Similarly, Wong et al 28 found that the FEAR index alone (2° threshold) was not predictive of the outcome of isolated arthroscopic treatment. However, 46% and 41% of the FEAR-positive and -negative hips failed to reach Patient Acceptable Symptom State for the modified Harris Hip Score, respectively. McQuivey et al 15 –17 found an AI >10° to be highly predictive of failure of arthroscopic treatment (84% reoperation rate) in a multicenter cohort of 373 hips. However, this study included many hips not labeled as “borderline” by most definitions (mean LCEA, 30°) by including hips with LCEA <25° or AI >10° (commonly used) or ACEA <25° (not commonly used). Similarly, the presence of increased femoral anteversion in the setting of borderline acetabular dysplasia demonstrated higher rates of reoperation and inferior clinical outcomes. 3
The FEAR index has been reported to have utility in this assessment and is increasingly used. 24,27,28 However, the original report assessed the parameter in the single-surgeon cohort (n = 39) in which it was developed, as well as included both classic acetabular dysplasia and borderline dysplasia, which may have affected its performance. 29 In the original description, the sensitivity and specificity of the FEAR index with a 5° threshold were 78% and 80%, respectively. 29 A subsequent study by the same group reported a 90% predictive ability of a FEAR threshold of 2° but included only hips with LCEA ≤20°. 2 Therefore, the FEAR index remains to be assessed in an isolated population with borderline dysplasia in which its main clinical application would exist. Also, the external validity of the FEAR index in an isolated population with borderline dysplasia remains important to understand before clinical use. An ideal screening test would have high sensitivity, thus identifying most patients with the finding of interest. On the other hand, an ideal confirmatory test would have a high specificity. In this external validation limited only to borderline dysplasia, the FEAR index (using the originally described threshold of 5°) appeared to be specific (92%) but poorly sensitive (33%). Thus, many hips diagnosed with instability and treated with PAO by the senior author (J.C.C.) were FEAR-negative. On the other hand, FEAR-positive status was highly predictive of the clinical diagnosis of instability. Similarly, limitations were seen with the more recently proposed 2° FEAR threshold. This external validation would support FEAR-positive status as being consistent with instability, but FEAR-negative status does not rule out instability and should be combined with the assessment of other radiographic and clinical factors.
This study assessed the performance of different FEAR index threshold values, in addition to the previously described 5° and 2° thresholds. Truntzer et al 27 recently performed an external assessment of the FEAR index, but only 13 of the 167 hips in their study had borderline acetabular dysplasia (92% had an LCEA >25°), which limited the value of this comparison. Truntzer et al proposed a threshold of –5° in identifying microinstability with a sensitivity of 28.9% and specificity of 92.4% but in a patient population mostly without dysplasia. Smith et al 24 externally evaluated the FEAR index in a population of skeletally immature patients with dysplasia (compared with controls and patients with FAI) and suggested that a FEAR index >–1.2° was most predictive of instability. The current study investigated alternative thresholds for the FEAR index and found no single threshold successfully achieving high sensitivity and specificity. A threshold of 5° achieved high specificity (92%), a PPV (74%), but low sensitivity (33%). A threshold of –5° was required to reach an adequate sensitivity of 74%. This defines 3 categories of FEAR index: (1) ≤–5, (2) –5 to 5, and (3) ≥5. Thus, hips of patients with a FEAR index ≥5° are likely unstable (specificity, 92%; PPV, 74%), and hips of patients with a FEAR index <–5° are likely stable (no instability [sensitivity, 74%]. These thresholds are in general useful, but those of more than one-fourth of patients are counter to this trend. Patients with a FEAR index between –5° and 5° are commonly diagnosed with or without instability and require careful assessment of all radiographic, 3-dimensional imaging, and clinical and physical examination factors.
The current study also established that the FEAR index provides additional information beyond AI or the physeal scar angle alone. AI is an important parameter in the setting of borderline dysplasia and also plays an important role in the FEAR index. The FEAR index is the difference between AI and the physeal scar angle. The FEAR index remained statistically significant even after controlling for AI or the physeal scar angle (P < .001). Bivariate modeling with both AI and physeal scar angle, in addition to the FEAR index, is not possible because of the mathematical relationship present, in which knowing 2 values determines the third. Safran, 22 in a cohort of primarily nondysplastic and nonborderline dysplastic hips, similarly found the FEAR index to provide predictive ability beyond AI or the physeal scar angle. However, in this study, instability was defined as meeting at least 1 intraoperative definition of microinstability, as has previously been described in the literature. 9,23 Furthermore, McClincy et al 14 observed several radiographic variables to determine instability in the borderline group. They also used a FEAR index threshold of 5° and found that the FEAR index average was a statistically significant difference in female patients with borderline dysplasia who had arthroscopic surgery (FEAR index, –7.8 ± 10.7) versus a PAO (FEAR index, 4.6 ± 6.5). Again, this is similar to the 5° threshold, but there is some overlap between groups. This reinforces the idea that the FEAR index alone remains inadequate to fully define the instability in many hips.
Limitations
One limitation of the current study was the use of a single-surgeon diagnosis as the gold standard. However, given that no established, externally validated criteria exist for the differentiation of unstable and stable hips, the current literature is limited to expert opinion and similarly holds this limitation. Wyatt et al 29 used radiographic criteria combined with plain radiographs and MRA scans to define instability in their cohort with mixed borderline and classic dysplasia. Some of these factors are unlikely to be present in the setting of borderline dysplasia, such as a broken Shenton line. Additionally, these criteria have no established validity and ignore other patient and physical examination factors that likely play a role in decision making. In the current study, we chose to use a single experienced surgeon’s clinical diagnosis, which took into account a larger number of patient and radiographic factors than are typically used in a clinical setting. We hope future research will help to establish standardized criteria that can be validly applied in the clinical setting. Until further research allows for development of such criteria, this limitation is unavoidable in the setting of borderline dysplasia and must be acknowledged, but it should not discredit further research on the topic.
There were several additional limitations. Outcomes were not analyzed in this study. Therefore, the predictability of the FEAR index on surgical outcomes could not be addressed but will be the focus of future investigation. Wong et al 28 recently reported no difference in the arthroscopic outcomes in the setting of borderline dysplasia relative to a FEAR threshold of 2°. Additionally, the current study included a cohort that underwent surgery over a 10-year period in which decision making likely evolved gradually. However, we believe that the large cohort (4 times the size of that of Wyatt et al 29 ) offset this limitation by improving its generalizability. A final limitation was that the current analysis was based on the radiographic readings of a single reader. However, we did demonstrate excellent intraobserver and interobserver reliability of the assessment of the FEAR index in a subgroup of patients in our study.
Conclusion
The current study demonstrated the external validity of the role of the FEAR index in identifying instability in the setting of borderline acetabular dysplasia but also demonstrated that the FEAR index alone is not a sensitive and specific marker of hip instability. In this external cohort, the proposed 5° or 2° cutoffs showed high specificity but poor sensitivity. Thus, the FEAR index alone remains inadequate to fully define the instability of most hips and is best used in the context of other clinical and radiographic features.
Footnotes
Final revision submitted April 3, 2022; accepted April 20, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded in part by the Curing Hip Disease Fund (to J.C.C.) and the Jacqueline and W. Randolph Baker Fund (to J.C.C.). J.C.C. has received research support from Zimmer; education payments from Elite Orthopedics; consulting fees from MicroPort, Smith & Nephew, and Zimmer; nonconsulting fees from MicroPort and Synthes; and royalties from MicroPort and Wolters Kluwer Health–Lippincott Williams & Wilkins. E.G. has received education payments from Elite Orthopedics. C.P.-G. has received research support from AOSSM/Sanofi and Zimmer, education payments from Elite Orthopedics and Zimmer, consulting fees from ARVIS, and hospitality payments from Stryker. J.J.N. has received research support from Smith & Nephew and Zimmer; education payments from Arthrex; consulting fees from Ceterix, Responsive Arthroscopy, and Smith & Nephew; nonconsulting fees from Smith & Nephew; and royalties from Responsive Arthroscopy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Washington University School of Medicine (reference No. 201406131).