
Abstract
Background:
Recent studies have shown that assessment of the lateral center-edge angle (LCEA) between 18° and 25° is not sufficient to adequately classify mildly dysplastic hips and that further radiological features should be considered. However, no correlation between different morphologic features and clinical outcomes has been investigated so far.
Purpose:
To analyze the clinical outcomes of patients with different subtypes of borderline dysplastic hips who underwent arthroscopic surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We examined patients with an LCEA between 18° and 25° who underwent arthroscopic treatment for femoroacetabular impingement syndrome between January 2015 and December 2016. A hierarchical cluster analysis was performed to identify hip morphologic subtypes according to radiographic parameters, including the LCEA, femoro-epiphyseal acetabular roof (FEAR) index, anterior and posterior wall indices (AWI and PWI), Tönnis angle, alpha angle, and femoral neck-shaft angle. In addition, the International Hip Outcome Tool 12 (iHOT-12) and a visual analog scale (VAS) for pain were applied preoperatively and at follow-up, and the results were compared among the different clusters. Previously reported minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) values were used to determine clinically significant improvements.
Results:
A total of 40 patients were identified. Of these, 36 patients were available for evaluation at a mean follow-up of 43.8 months. In total, 4 sex-independent clusters with different morphologic patterns of the hip were identified: cluster 1, unstable anterolateral deficiency (FEAR index >2°, AWI <0.35); cluster 2, stable anterolateral deficiency (FEAR index <2°, AWI <0.35); cluster 3, stable lateral deficiency (FEAR index >2°, normal AWI and PWI); and cluster 4, stable posterolateral deficiency (FEAR index <2°, PWI <0.85). At follow-up, clusters 1, 2, and 3 showed significantly improved iHOT-12 (P < .0001) and VAS pain (P < .0001) scores, and cluster 4 showed no significant improvements. The MCID of 15.2 points was achieved by all patients in clusters 2 and 3, by 63% of patients in cluster 1, and by 23% of patients in cluster 4. Clusters 2 and 3 differed significantly from clusters 1 and 4 (P = .02). A postoperative PASS score of 60 was achieved by all patients in cluster 3, by 86% of patients in cluster 2, by 63% of patients in cluster 1, and by 20% of patients in cluster 4. The differences between the groups were statistically significant (P = .01).
Conclusion:
Arthroscopic surgery yielded good results in the treatment of stable borderline hip dysplasia with anterolateral and lateral deficiency. In contrast, borderline hip dysplasia with acetabular retroversion showed no improvements after arthroscopic therapy. This study underlines the need for an accurate analysis of all possible radiological signs to adequately classify borderline dysplastic hips.
Keywords
Hip arthroscopy has developed rapidly in recent years and is now regarded as the gold standard for the treatment of various hip conditions, such as femoroacetabular impingement syndrome (FAIS). However, whether hip arthroscopy is a suitable therapeutic tool for borderline dysplasia of the hip remains unclear. In recent years, the conclusions about whether a borderline dysplastic hip should be treated with periacetabular osteotomy (PAO) or hip arthroscopy have been controversial. 7,11,25,26,28 –31,49
Historically, acetabular dysplasia was defined as insufficient coverage of the femoral head by the acetabulum and was quantified by the lateral center-edge angle (LCEA) introduced by Wiberg. 47 According to Wiberg, hips with an LCEA greater than 25° are normal and those with an LCEA less than 20° are pathological or dysplastic. Currently, borderline hip dysplasia is typically defined by an LCEA between 18° and 25°. 13,16,35,41 This margin is usually used by clinicians and scientists when analyzing the outcomes after treating borderline hip dysplasia.
In recent years, several studies have described significant improvements in arthroscopic capsular plication and labral preservation in patients with borderline hip dysplasia. In these studies, borderline dysplasia was defined only by the LCEA. 7,10,11,28,35 Historically, studies have shown that hips with an LCEA between 18° and 25° are not adequately classified by the LCEA alone, because this measurement addresses only 1 of several radiographic parameters. 31,48,49 Wyatt et al 48 introduced the femoro-epiphyseal acetabular roof (FEAR) index in 2017 as a decision tool to help classify borderline hips as stable or unstable. The FEAR index is formed by the angle between the central third of the femoral growth plate and the acetabular roof. This angle reveals the resultant force vector, which can predict the behavior of hips with borderline dysplasia. A laterally directed vector may lead to forces that can potentiate instability. Subsequent research revealed that a value of 2° or less predicts stability with a 90% probability. 49 The authors stated that stable hips might be better treated with hip arthroscopy and that unstable hips may be treated with PAO.
As a continuation of this idea, McClincy et al 31 postulated in 2019 that borderline hips reveal differences in terms of acetabular and femoral morphologic features. The researchers analyzed various relevant radiographic measurements, including the acetabular inclination angle of Tönnis, 44 the anterior wall index (AWI), the posterior wall index (PWI), 43 and the FEAR index. 48 The authors were able to define different sex-specific clusters. 31 For female patients, 3 clusters were identified: acetabular deficiency with cam morphology, lateral acetabular deficiency, and anterolateral acetabular deficiency. As well, 3 clusters were identified for male patients: posterolateral deficiency with global cam morphology, posterolateral acetabular deficiency with focal cam morphology, and lateral acetabular deficiency without cam morphology. However, the authors made no reference to the clinical outcomes. It is not yet clear what influence the different morphologic features have on clinical outcome.
The aim of this study was to analyze the clinical outcomes of patients with different subtypes of borderline hip dysplasia who underwent treatment with arthroscopic surgery. Our hypothesis was that patients with an LCEA between 18° and 25° can be assigned to different subtypes according to radiological measurements and that the clinical results after hip arthroscopy differ depending on the subtype.
Methods
This was a single-center retrospective study. After gaining approval from the local ethics committee, we retrospectively reviewed our hospital registry to identify all patients who underwent hip arthroscopy between January 2015 and December 2016 and had a minimum follow-up duration of 36 months. The inclusion criterion was primary hip arthroscopy to treat FAIS in a patient with an LCEA between 18° and 25°. The exclusion criteria were secondary hip conditions (eg, slipped capital femoral epiphysis), revision hip arthroscopy, reduced joint space (Tönnis grade >1), and an LCEA less than 18° or greater than 25°. At the time of the surgeries (2015 and 2016), our algorithm aimed at hip arthroscopy for all hip conditions where the LCEA was greater than 18°. PAO was recommended only for patients with an LCEA less than 18°.
The baseline demographics and clinical and radiological details were obtained through a retrospective review of the patient’s electronic medical record. The International Hip Outcome Tool–12 (iHOT-12) score and visual analog scale (VAS) pain score (0, no pain; 10, extreme pain) were recorded preoperatively and at follow-up. Beck et al 2 recently published minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) values of 15.2 and 60 points, respectively, for the iHOT-12 in patients with borderline hip dysplasia treated by arthroscopic surgery. These values were used to report clinically significant improvements in the outcome scores. All participants provided written informed consent.
Radiographic Evaluation
A standing anteroposterior pelvic radiograph (radiographic criteria: neutral tilt as determined by coccyx-symphyseal distance and neutral rotation as determined by symmetry of the obturator foramen) and a 45° Dunn lateral radiograph were acquired as standards in all patients before surgery. The anteroposterior pelvic radiograph was used to measure the Wiberg LCEA at the edge of the sourcil, 47 the Tönnis angle to describe the acetabular inclination angle, 44 the FEAR index, 48 the AWI and PWI, 43 and the femoral neck-shaft angle. In addition, the presence of the crossover sign (COS), posterior wall sign (PWS), and ischial spine sign was recorded 21,22,40 ; the presence of the these 3 signs indicates acetabular retroversion. 34,46 The alpha angle as described by Nötzli et al 37 was measured on the Dunn lateral radiographs.
Figure 1 illustrates the radiographic measurements used in this study. All measurements were performed by 2 orthopaedic surgeons (A.Z., C.S.) trained in hip arthroscopy using mediCAD (mediCAD Hectec GmbH). The data were analyzed by calculating intraclass correlation coefficients (ICCs), a measure of the proportion of variance that is attributable to individuals. 32 An ICC of 1 indicates perfect agreement. The means and standard deviations of the differences between the 2 observers were also calculated. In addition, magnetic resonance imaging (MRI) was performed to assess damage to the cartilage and labrum.

Radiographic measurements. (A) Lateral center-edge angle: calculated by drawing a best-fit circle around the inferior and medial margins of the femoral head. The angle is measured between 2 lines drawn from the center of the circle, one running vertically along the longitudinal axis of the pelvis and the other running vertically along the acetabular sourcil edge. 47 (B) Femoro-epiphyseal acetabular roof index: formed by 2 lines connecting the acetabular roof inclination and the femoral head physeal scar. 48 (C) Tönnis angle: measured by drawing a horizontal line parallel to the transverse pelvic axis, at the most medial edge of the sclerotic sourcil, and then making a second line extending from the medial edge to the most lateral aspect of the sourcil. 44 (D) Alpha angle: measured angle between the line connecting the point of no sphericity of the femoral head from the center of the femoral head and another line extending up to the center of the femoral head from the center of the femoral neck at the narrowest point. 37 (E) Anterior wall index (AWI) and posterior wall index (PWI): measured by drawing a circle to approximate the femoral head and determining the radius of the head (r). Lines from the medial edge of the circle to the anterior (a) and posterior (p) walls are drawn and measured along the femoral neck axis. The AWI and PWI are calculated as a/r and p/r, respectively. 43 (F) Femoral neck-shaft angle: the angle made by the intersection of the longitudinal axis of the neck with that of the longitudinal axis of the femoral shaft.
Surgical Technique
All procedures were performed at our institution by 2 surgeons (W.M., C.S.), each of whom performs more than 300 hip arthroscopies per year. The patients were in the supine decubitus position under general anesthesia during surgery. They were positioned on a traction table with a well-padded perineal post and were subjected to traction to distract the hip. In total, 2 or 3 standard arthroscopy portals were used during the surgery: the anterolateral portal, the midanterior portal, and the distal anterolateral accessory portal if labral repair was necessary. The landmarks established for safe portals, as described by Robertson and Kelly, 42 were used. A routine evaluation of the joint was then undertaken to evaluate the labrum and articular cartilage. The acetabular cartilage was graded through use of the acetabular labral articular disruption classification. 5 Labral lesions were classified according to the system described by Beck et al. 3 The ligamentum teres was evaluated with the Gray and Villar 18 classification.
A capsulotomy was performed between the anterolateral and midanterior regions if necessary. Labral repair was performed by use of 2.9-mm PushLock suture anchors (Arthrex) via a loop- or base-repair technique if the labrum showed acceptable consistency and quality. 15 If the labrum was no longer repairable, the surgeon performed selective labral debridement while preserving as much of the stable labrum as possible to retain a functional seal between the labrum and the femoral head. Cartilage damage was treated by chondroplasty or abrasion according to the different damage stages. In the case of focal anterior pincer morphology, the surgeon carefully trimmed the anterior rim using a round bur without decreasing the amount of anterior bony coverage. Femoroplasty was performed if cam morphology was present. At that time the capsule was not routinely closed, because little evidence for capsular closure was available during the eligibility period. Nowadays, we routinely perform a capsular closure based on the available data. 1,4,13
Rehabilitation
Physical therapy began immediately after surgery with passive exercise using an active motion device (CAMOped; OPED). The patients used crutches for 3 weeks with partial weightbearing (10-20 kg), and passive hip rotation was restricted for 4 weeks. A specific hip rehabilitation protocol was initiated (“the groin concept” 33 ). Heterotopic ossification prophylaxis with nonsteroidal anti-inflammatory drugs was recommended for 2 to 3 weeks. 24,50
Statistical Analysis
Data were analyzed by use of SPSS version 20 (IBM). Parametric comparisons were performed for continuous data through use of the 2-tailed Student t test. The threshold for statistical significance was set to .05.
Similar to McClincy et al, 31 we performed an agglomerative hierarchical clustering analysis of the continuous radiographic variables to identify clusters and subtypes of borderline hip dysplasia. Subsequently, the number of clusters was determined by evaluating the cluster dendrogram. After the grouping procedure, Kruskal-Wallis and Mann-Whitney U tests were used as post hoc tests to compare the clusters. A comparison of the iHOT-12 and the VAS pain scores through use of Student t test showed no difference between the sex-specific clusters, so these clusters were grouped together in 1 cluster.
Results
Patient Characteristics
A total of 40 patients with an LCEA between 18° and 25° who underwent primary hip arthroscopy between January 2015 and December 2016 were identified and met the inclusion criteria. Of these, 36 patients were available for the follow-up evaluation; 4 patients refused to participate. The patient characteristics are presented in Table 1.
Patient Characteristics a

a Data are presented as mean ± SD (range) unless otherwise noted.
Intraoperative Findings and Arthroscopic Procedures
In total, 89% of the patients had acetabular chondral damage. None of the hips showed femoral chondral lesions. We found that 1 (2.8%) hip had a partial ligamentum teres tear. Further, 25 (69.4%) hips had labral lesions; of these, 13 (36.1%) had unstable lesions. The arthroscopic findings are documented in Table 2.
Intraoperative Findings a

a ALAD, acetabular labral articular disruption.
A total of 13 (36.1%) hips underwent labral repair, and 12 (33.3%) underwent labral debridement. Ligamentum teres debridement was performed in 1 (2.8%) hip. We noted that 17 (47.2%) patients underwent femoroplasty, and 3 (8.3%) underwent anterior acetabuloplasty. Further, 12 (33.3%) hips needed microfracturing, and acetabular chondroplasty was performed in 20 (55.5%) hips. The arthroscopic procedures are presented in Table 3.
Arthroscopic Procedures

Radiographic Analysis
In total, 4 sex-independent clusters with different hip morphologic patterns were identified: unstable anterolateral deficiency (cluster 1); stable anterolateral deficiency (cluster 2); stable lateral deficiency (cluster 3); and stable posterolateral deficiency (cluster 4). We found very good agreement between the 2 observers in classifying the 4 subtypes and clusters (ICC, 0.98). Case examples (mean values of the measurement results of both observers) of the 4 different clusters are shown in Figure 2.
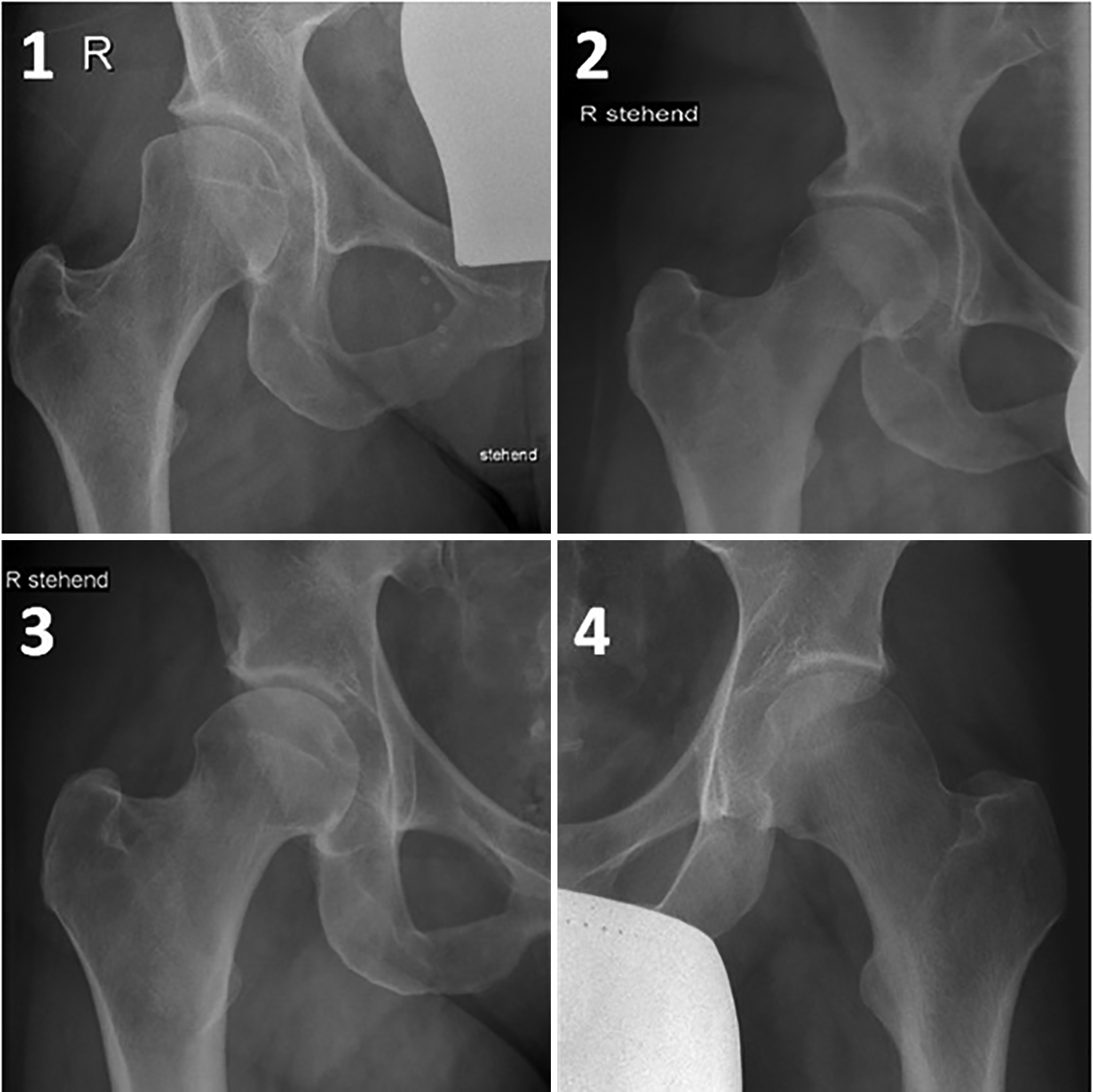
Examples of the 4 hip morphologic clusters: (1) unstable anterolateral deficiency; (2) stable anterolateral deficiency; (3) stable lateral deficiency; and (4) stable posterolateral deficiency.
The unstable anterolateral deficiency cluster was characterized by hips with a FEAR index greater than 2°, an LCEA between 18° and 25°, and a low AWI value, suggesting anterior undercoverage. Notably, only hips with anterolateral deficiency had a FEAR index greater than 2°. Only female patients (n = 8) were assigned to this cluster. The stable anterolateral deficiency cluster was characterized by a FEAR index less than 2° and radiographic parameters indicative of abnormal acetabular lateral and anterior coverage, as evidenced by an LCEA between 18° and 25° and a low AWI value. Similar to cluster 1, this cluster included only female patients (n = 7). The stable lateral deficiency cluster was noted to have relatively normal radiographic parameters, aside from an LCEA between 18° and 25°. This cluster included 1 male and 5 female patients. The stable posterolateral cluster had a FEAR index less than 2°, an LCEA between 18° and 25°, and signs of posterior acetabular deficiency, as evidenced by a low PWI value. This cluster had the most patients (n = 15), and all hips showed all 3 radiological signs of acetabular retroversion (positive COS, PWS, and ischial spine sign). Of the 15 patients, 11 were male and 4 were female. Therefore, this cluster contained the largest proportion (73.3%) of men.
Our study did not consider cam morphology regarding cluster formation, as this criterion would have reduced the group size per cluster. Two hips in cluster 1, one hip in cluster 2, one hip in cluster 3, and thirteen hips in cluster 4 showed cam morphology. However, in the cases of femoroplasty, the postoperative radiographs showed a sufficient correction of the cam morphology. The alpha angle was 48.0° ± 3.6° (range, 44°-52.5°) postoperatively. The radiographic measurements and cluster analysis findings are presented in Table 4.
Radiographic Measurements and Cluster Analysis Findings a
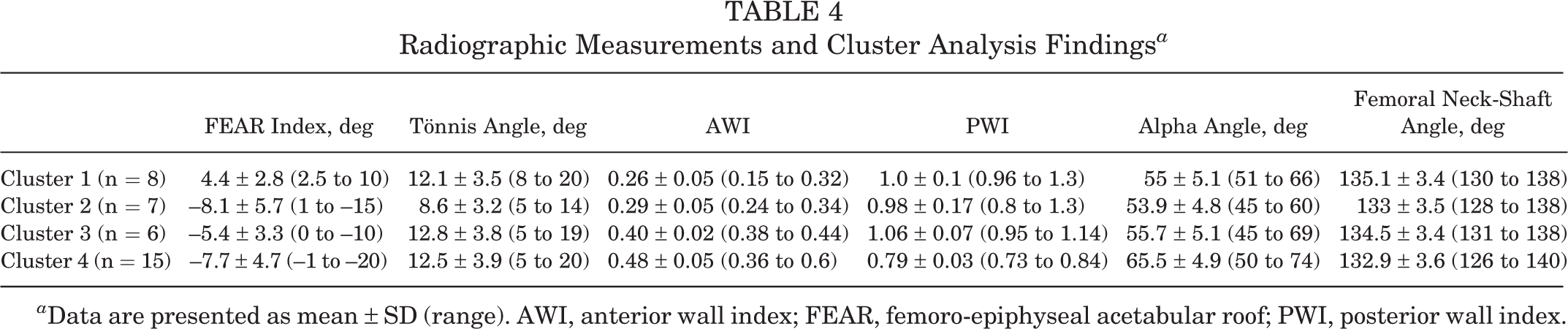
a Data are presented as mean ± SD (range). AWI, anterior wall index; FEAR, femoro-epiphyseal acetabular roof; PWI, posterior wall index.
Clinical and Patient-Reported Outcomes
At a mean follow-up of 43.8 months, clusters 1, 2, and 3 showed significant improvements, and cluster 4 showed no significant improvements from preoperative iHOT-12 and VAS scores. The scores are listed in Table 5.
iHOT-12 Scores and VAS Pain Scores a

a Data are presented as mean ± SD (range). iHOT-12, International Hip Outcome Tool–12; VAS, visual analog scale.
A significant difference in outcome scores was found among the 4 clusters on follow-up (P < .05; Kruskal-Wallis test). In the post hoc pairwise comparisons (Mann-Whitney U tests), we found statistically significant differences between clusters 1 and 2 (iHOT-12, P = .01; VAS, P = .01), clusters 1 and 3 (iHOT-12, P = .02; VAS, P = .01), clusters 2 and 4 (iHOT-12, P = .001; VAS, P < .0001), and clusters 3 and 4 (iHOT-12, P = .02; VAS, P = .01). No significant differences were found upon comparison of clusters 1 and 4 (iHOT-12, P = .2; VAS, P = .15) and clusters 2 and 3 (iHOT-12, P = .32; VAS, P = .21). Clusters 2 and 3 therefore showed superior outcome scores to clusters 1 and 4. Regarding the analysis of labral repair versus labral debridement, no difference in the failure rate with respect to the different clusters was noted.
An MCID of 15.2 points was achieved by all patients in clusters 2 and 3, by 63% of patients in cluster 1, and by 23% of patients in cluster 4. Clusters 2 and 3 differed significantly from clusters 1 and 4 (P = .02). A postoperative PASS score of 60 was achieved by all patients in cluster 3, by 86% of patients in cluster 2, by 63% of patients in cluster 1, and by 20% of patients in cluster 4. The differences between the groups were statistically significant (P = .01).
We noted that 2 patients (one from cluster 1 and one from cluster 3) required total hip arthroplasty (THA) in the follow-up period due to progressive cartilage damage, which corresponds to a conversion rate of 5.6%.
Discussion
The main findings of this study are that borderline hip dysplasia can be divided into subgroups, with different clinical results recorded for these subgroups. Similar to McClincy et al, 31 we were able to identify these different clusters based on a radiological analysis. Although patients with stable borderline hip dysplasia with lateral and anterolateral deficiency achieved highly significant improvements in terms of the iHOT-12 score and VAS pain score, patients with stable borderline hip dysplasia with posterolateral deficiency showed no significant improvements. In patients with unstable borderline hip dysplasia with anterolateral deficiency, significant improvements were observed, but these results differed from those in patients with stable borderline hip dysplasia with anterolateral deficiency, which were significantly better. The conversion rate to THA for all patients included was 5.6%, which is in line with other studies that reported conversion rates between 4.4 and 26%. 6,16,19,23
McClincy et al 31 identified sex-specific hip morphologic features and were able to assign 3 different subtypes to each sex. In their study, male hips showed either posterolateral or lateral deficiency, which was confirmed by our results. However, in contrast to McClincy et al, we also found some female patients with borderline hip morphology with a posterolateral deficiency. Nepple et al 36 analyzed 50 patients with hip dysplasia who underwent PAO. The authors determined 3 different types of dysplasia: anterosuperior deficiency, global deficiency, and posterosuperior deficiency. In that study, 80% of the male patients and 29% of the female patients exhibited posterosuperior deficiency. Peters et al 38 analyzed 30 patients with retroverted acetabula with lateral and/or posterior undercoverage who underwent PAO; the population included 11 male patients and 19 female patients. These results are in line with our findings.
In recent years, several studies have analyzed hip arthroscopy outcomes for borderline hip dysplasia and shown promising results. 10 Domb et al 11 reported the results from a minimum of 5 years after capsular plication and labral preservation. All patient-reported outcome scores increased significantly after treatment. 7,11 Cvetanovich et al 9 showed similar results after capsular plication; in their study, all outcome scores were also significantly increased. However, the presence of borderline dysplasia was predominantly defined by an LCEA between 18° and 25°. No further radiological analyses were carried out in any of the studies to determine different morphologic features. Whether subdivision into different clusters would have led to variations in clinical outcomes among the subgroups remains questionable.
The main argument for capsular plication is the hypothesis that the capsule plays a large role in providing stability to the hip, which makes the hip more amenable to arthroscopic surgery. 4,12 Recent studies, including biomechanical studies, have shown that a capsular closure restored rotational range of motion and joint translation to near-intact levels. 1,39 In our study, capsular plication was not routinely performed because little evidence was available for capsular closure during the years of the investigation (2015 and 2016). Nonetheless, in the case of stable lateral and anterolateral borderline dysplasia, we were able to achieve good and very good results, respectively. The question therefore remains whether capsular plication for unstable anterolateral borderline dysplasia can provide the necessary stability to compensate for the difference between stable and unstable anterolateral borderline hip dysplasia.
Wyatt et al 48 developed the FEAR index to distinguish between stable and unstable situations. A positive index implies a force vector that is directed laterally and can therefore cause and amplify instability. Wyatt and Beck 49 recommended the bony correction of unstable situations by PAO. McClincy et al 30 reported improvements in hip pain and function after PAO in patients with an LCEA between 18° and 25°. Those authors showed that 94% of the hips had at least 1 other radiographic feature of dysplasia. Overall, 71% presented with insufficient anterior femoral head coverage. At a 2.2-year follow-up, the patients reported significantly improved values on the modified Harris Hip Score (mHHS) and Hip Osteoarthritis and Outcome Score (HOOS). In our study, the group of unstable anterolateral borderline hips (cluster 1) had significantly inferior results compared with the group of stable anterolateral borderline hips (cluster 2). Further controlled studies will be necessary in the future to confirm the results and to evaluate the influence of capsular plication on unstable borderline hips in comparison with that of PAO in these patients.
A subgroup with posterolateral deficiency (cluster 4) did not show any significant improvements after arthroscopic therapy. These patients showed all 3 radiological signs (COS, PWS, ischial spine sign) of acetabular retroversion. In addition, 13 of the 15 patients in this cluster had cam morphology. In these patients, a femoroplasty was performed to treat this cam morphology. The preoperative alpha angle was 65.5° ± 4.9° (range, 50°-74°) and the postoperative alpha angle was 48.5° ± 3.5° (range, 45°-52°), so we believe that the correction was sufficient. The sufficient correction of the alpha angle underlines the fact that for these patients, a main problem may lie in the retroverted acetabulum. In retroverted acetabula, the posterior contact area is decreased and the anterior contact stress increases and may lead to degenerative changes for the joint cartilage. 3,8,17,27 A recent study by Vahedi et al 45 investigated the influence of isolated femoroplasty on patients with acetabular retroversion compared with those who had normal acetabular version. At the 2-year follow-up, the mean mHHS and 36-Item Short Form Health Survey scores were significantly lower in the retroversion group than in the control group. The retroversion group had a higher percentage of failure than the control group. This study shows that even without lateral deficiency (an LCEA between 18° and 25°), acetabular reorientation is necessary and, according to the authors, should be suggested. Our results underline these published data.
Peters et al 38 published an algorithm that suggested anteverting PAO for acetabula with anterior overcoverage and deficient posterior coverage, whereas acetabula with appropriate posterior and lateral coverage can be effectively treated with femoroplasty and anterior rim trimming. In the midterm follow-up, the HHS improved significantly from 72 to 91 in the hips treated with PAO and from 52 to 91 in the hips treated with femoroplasty and anterior rim trimming. McClincy et al 30 recently published the results of PAO treatment in 56 patients with an LCEA of 18° to 25°. The authors reported significant improvements in the mHHS, HOOS, and physical domain score of the 12-Item Short Form Health Survey questionnaire. Although the radiological analysis included the LCEA, Tönnis angle, AWI, PWI, and FEAR index, no correlations between possible subtypes of borderline hip dysplasia were made. Zurmühle et al 51 investigated the outcomes of hips that underwent anteverting PAO compared with those that underwent acetabular rim trimming with refixation of the labrum. The authors found increased survivorship in hips that underwent anteverting PAO compared with those that underwent acetabular rim trimming (79% [95% CI, 68%-90%] vs 23% [95% CI, 6%-40%]) at 10 years (P < .001). Those authors concluded that anteverting PAO may be the more appropriate treatment for hips with substantial acetabular retroversion. In the case of posterolateral deficiency, we would therefore not recommend isolated arthroscopic acetabular rim trimming, as resection of the anterior margin could result in global deficiency, which could cause multidirectional instability.
In recent years, clinically significant outcome parameters have been reported in addition to patient-reported outcome scores to quantify the degree of outcome improvement. These parameters include the MCID and PASS. We used the MCID (15.2 points) and PASS (60 points) established by Beck et al 2 for the iHOT-12 in patients undergoing arthroscopy for borderline hip dysplasia. In our study, all patients in clusters 2 and 3 and 63% of patients in cluster 1 reached the MCID, whereas only 23% of patients in cluster 4 exceeded the MCID. A postoperative PASS score of 60 was achieved by all patients in cluster 3, by 86% of patients in cluster 2, by 63% of patients in cluster 1, and by 20% of patients in cluster 4. These findings illustrate that patients with posterolateral deficiency in the sense of a retroverted acetabulum do not clinically improve through arthroscopic surgery. It has also been shown that almost two-thirds of patients with an unstable condition (FEAR >2°) improve clinically through arthroscopic surgery and achieve a satisfactory condition.
Our study has several limitations. First, the number of patients per cluster was small, so the results must be confirmed with larger group sizes. A post hoc power analysis using GPower 14 with power (1-β) set at .80 and α at .05 revealed that on the basis of the mean, a sample size of approximately 85 would be needed to obtain statistical power. Another limitation is the lack of a control group of patients who underwent PAO to treat borderline hip dysplasia. Controlled trials would help determine whether PAO is superior to arthroscopy for unstable borderline hip dysplasia. Our study investigated radiographic parameters without the use of advanced imaging modalities (MRI or computed tomography). However, the different radiological signs are often sufficient for recognizing the different morphologic conditions and can be used to stratify groups. Our clustering analysis considered only acetabular version. We did not consider the influence of either cam morphology or femoral version. Additionally, in the present study population, no capsular repair was performed because little evidence was available for capsular closure during the investigated period of time. Nowadays capsular closure or plication is routinely performed, and the effect on the outcome in this special patient group should be further analyzed. Finally, our study involved a minimum follow-up period of 2 years, and whether these results will persist over time is unknown, especially since dysplasia can lead to an early onset of arthrosis. 2,3,20
Conclusion
This study correlated clinical outcomes after hip arthroscopy with different types of borderline hip dysplasia. Our study underlines the need for an accurate analysis of all possible radiological signs to adequately classify borderline hip dysplasia. An analysis of the LCEA alone is not sufficient because the subgroups experience different clinical outcomes and should not be mixed. Arthroscopic surgery yielded good results in the treatment of stable borderline hip dysplasia with anterolateral and lateral deficiency. In contrast, the results were not as successful in the group with additional acetabular retroversion.
Footnotes
Final revision submitted January 23, 2020; accepted February 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.M. has received consulting fees from Arthrex and Richard Wolf. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the State Medical Association of Baden-Württemberg (ref No. F-2019-006).