
Abstract
Background:
Proper anatomic restoration is an important consideration for meniscal allograft transplantation (MAT), even with the different anatomica characteristics between the medial meniscus and lateral meniscus.
Purpose/Hypothesis:
The purpose of this study was to assess the accuracy of anatomic restoration in medial and lateral MAT (MMAT and LMAT) procedures and to compare their outcomes. We hypothesized that (1) the anatomic differences between the medial and lateral menisci will mean a less accurate anatomic restoration for MMAT and (2) clinical outcomes after MMAT will be inferior compared with LMAT.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively evaluated 20 patients who underwent MMAT using the bone plug technique and 21 patients who underwent LMAT using the keyhole technique at a single institution from July 2014 to June 2019. Demographic data, previous surgeries, and concomitant procedures were recorded, as were lower limb alignment and osteoarthritis grade on radiographs. Using preoperative and follow-up magnetic resonance imaging, the meniscal position, rotation, extrusion, and intrameniscal signal intensity were evaluated. Clinical outcomes were evaluated using the International Knee Documentation Committee and Lysholm scores.
Results:
The mean follow-up was 41.15 ± 18.86 and 45.43 ± 21.32 months for the MMAT and LMAT patients, respectively. Concomitant procedures were performed in 90% of MMATs and 15% of LMATs. There was no significant difference between the native and postoperative root positions after LMAT; however, for MMAT, the position of the anterior root was located significantly posteriorly (P = .002) and medially (P = .007) compared with preoperatively. In addition, the allograft medial meniscus was restored in a more internally rotated position (P = .029). MMATs also exhibited significantly increased meniscal extrusion compared with LMATs (posterior horn, P < .001; midbody, P = .027; anterior horn, P = .006). However, there was no significant difference between the 2 groups at final follow-up in intrameniscal signal intensity or clinical scores.
Conclusion:
LMAT showed higher accuracy than MMAT in restoring meniscal position and rotation, and there was less meniscal extrusion. However, clinical scores improved after both LMAT and MMAT compared with preoperative values, and midterm clinical outcomes were similar. The small anatomical errors seen in the MMAT technique were not clinically relevant at midterm follow-up.
The medial and lateral menisci are typically thought of as important shock absorbers in the knee joint. 25 However, the medial and lateral menisci have different anatomical and biomechanical characteristics. The medial meniscus covers 64% of the medial tibial plateau and transmits approximately 50% of the load. 30 Degenerative lesions mainly occur on the medial side, and the medial meniscus acts as a secondary stabilizer for anterior translation together with the anterior cruciate ligament (ACL). 29 The lateral meniscus covers 84% of the lateral tibial plateau and transmits approximately 70% of the load. 30 Compared with the medial meniscus, the lateral meniscus is more mobile, and acute traumatic lesions predominantly occur there. 22
Recognizing the role of the menisci in maintaining knee homoeostasis has led to a trend toward meniscus-preserving surgery; however, some cases are irreparable, such as avascular tears, unsalvageable tear types, and previous repair failure. Young, active patients who have lost meniscal function receive a meniscal allograft transplantation (MAT). MAT has been shown to provide superior long-term benefits with consideration of concomitant articular cartilage lesions, joint alignment, and knee stability. 2
Accurate sizing and positioning are thought to be necessary for a successful outcome after MAT. 3,6 The medial meniscus has a greater distance between the anterior and posterior horn and a downward slope from the anterior to the posterior horn on the sagittal plane. On the contrary, the lateral meniscus has a very short distance between the anterior and posterior horn and an upward slope from the anterior to the posterior horn. In the midbody regions, both the medial and lateral menisci have a posterior slope, although the degree of slope is larger for the medial side. 7 In addition, different rotation angles on the axial plane are important. 16,20
The different geometries of the medial and lateral menisci make the MAT technique different for each. 4,10,21 Medial MAT (MMAT) is generally performed using the bone plug technique, whereas lateral MAT (LMAT) is performed with a keyhole or trough technique, based on geometric characteristics. The nonanatomical transplantation in LMAT procedures increases the contact pressure and may eventually adversely affect the chondral surface. 23 Therefore, in the keyhole technique, 3-dimensionally accurate positioning should be concomitantly considered for anatomic positioning. In the bone plug method, proper meniscal size and exact visualization of the native meniscal insertion is a key factor for the chondroprotective effect, but passing the graft through a tight medial joint with a cylindrical bone plug can be difficult. 9,14 These different surgical techniques may lead to different results, including meniscal extrusion, meniscal tear, progression of degenerative change, and clinical outcomes. 18
The purpose of this study was to assess the accuracy of anatomic restoration in the MMAT and LMAT procedures and compare the clinical and imaging outcomes, including postoperative follow-up magnetic resonance imaging (MRI). Our hypotheses were that (1) the anatomic differences between the medial and lateral menisci MMAT will signify a less accurate anatomic restoration for MMAT and (2) clinical outcomes after MMAT will be inferior compared with LMAT.
Methods
Patients
Patients who underwent MAT between July 2014 and June 2019 were retrospectively enrolled. All patients had undergone partial or total meniscectomy during previous surgeries. The indications for MAT were (1) persistent medial or lateral knee pain attributed to previous partial/total meniscectomy despite nonoperative treatment and (2) patients aged younger than 45 years. The contraindications were as follows: (1) asymptomatic patients, (2) severe osteoarthritis (Kellgren-Lawrence grade 3 or 4), (3) uncorrected malalignment or instability, (4) active infection, or (5) inflammatory arthropathy. Combined malalignment and instability were restored by osteotomy or ligament reconstruction at the time of MAT. A total of 41 patients were enrolled, of which 20 were in the MMAT group and 21 were in the LMAT group. Institutional review board approval was obtained before performing any analyses.
Surgical Technique
All operations were performed by a single experienced surgeon (Y.S.L.) in patients who had persistent pain after partial or total meniscectomy. It required waiting for approval 12 months before MMAT and 6 months before LMAT according to the national insurance policy. Fresh-frozen allografts were used in all the cases. The graft was sized using MRI on the axial cut of the tibial plateau before surgery. The width of the medial or lateral tibial plateau from the tibial spine to the edge of the tibial condyle was matched to the allograft width. For both the medial and lateral menisci, the length between the anterior and posterior roots was measured as the allograft length. 10,30
The bone plug technique, in which the graft contains separate bone plugs attached to the horns, was used to perform MMAT. LMAT was performed using the keyhole technique, in which the graft contained a bone trough attached to the anterior and posterior horn. Meniscal peripheral remnant preservation was done arthroscopically to ensure adequate graft stability and healing. For MMAT, an ACL tibial guide was inserted, and the position of the native posterior horn of the medial meniscus (MMPH) was confirmed from the anterior and posterior through the transseptal portal. After the posterior tunnel was created using a reamer of 10 mm (Flipcutter; Arthrex®), the cartilage around the tunnel was removed for firm fixation and good healing of the graft. After that, the location of the anterior root of the medial meniscus (MMAR) was confirmed by using the anterior portal to confirm the native MMAR, and a tunnel was made using the 10-mm reamer. After graft passage, the anterior and posterior bone plug leading sutures were firmly tied. For LMAT, the transpatellar tendon approach was used for accurate restoration of the anterior horn of the lateral meniscus. A guide pin was inserted while considering the upslope of the meniscal insertion. A bone tunnel for the trough was created using a reamer to confirm the accurate position from the anterior and posterior through the transseptal portal (Figure 1).

(A-C) Identification and formation of the MMPH using the transseptal portal and (D) the MMAH near the ACL tibial tunnel. (A) PCL and deficient MMPH seen through the posteromedial portal. (B) Guide positioned on the native MMPH using the posterior transseptal portal. (C) Creating a tunnel with the Flipcutter using ACL guide. (D) Anterior horn position near the ACL tibial tunnel. Compared with the location of the tunnel, the allograft bone plug is pulled more medially. (E-H) Identification and creation of a keyhole using a transseptal portal during LMAT. (E) Posterior insertion is identified using posterior portals. (F) A guide pin was inserted while considering the upslope of meniscal insertion. (G) Accurate position from the anterior and posterior is confirmed through the transseptal portal. (H) Exact hole formation is confirmed via arthroscope into the hole, and clearing of the posterior cortex is also confirmed for the insertion of the LMAT. ACL, anterior cruciate ligament; LFC, lateral femoral condyle; LMAT, lateral meniscal allograft transplantation; LMPH, lateral meniscal posterior horn; MMAH, medial meniscal posterior horn; MMPH, medial meniscal posterior horn; MTP, medial tibial plateau; PCL, posterior cruciate ligament.
In an all-inside manner, the posterior aspect of the graft was sutured with the meniscal peripheral remnant using 2 to 3 stitches. Using inside-out meniscal repair techniques, 6 to 8 sutures were placed from the posteromedial or posterolateral parts of the meniscal allograft to the anteromedial or anterolateral part of the meniscal allografts. In the anterior aspect, the graft was fixed through 2 to 4 stitches using the outside-in technique. All sutures were performed using absorbable polydioxanone suture material (Figure 2). By pulling the sutures, the graft was adjusted precisely again on the tibial plateau, and the correct position of the graft was confirmed.

(A) The posterior aspect of the graft was sutured with the meniscal peripheral remnant using 2 to 3 stitches of all-inside sutures and a suture hook. (B) Using the inside-out meniscal repair technique, 6 to 8 sutures were placed from the posteromedial or posterolateral corner to the anteromedial or anterolateral corner. (C) In the anterior aspect, the graft was fixed through 2 to 4 stitches of the outside-in technique. All sutures were performed using absorbable polydioxanone suture material.
Postoperative Rehabilitation
Weightbearing as tolerated with crutches was permitted immediately after surgery, with subsequent gradual weaning of the crutches until 6 weeks after. Patients were encouraged to achieve 90° of flexion within 4 weeks for MMAT and within 6 weeks for LMAT. Full flexion was allowed at 3 months. Full return to active daily living was allowed 3 months after surgery, and light sports activity was permitted 6 months postoperatively.
Evaluation
Demographic data, previous surgery, and combined procedures were recorded. Radiographic evaluation was performed to assess lower limb alignment and osteoarthritis grade. To evaluate the degree of meniscal anatomic restoration, preoperative and postoperative MRI scans were compared. Two orthopedic surgeons (H.W.J. and J.S.K.) independently assessed the MRIs with an interval of 6 weeks to reduce intraobserver and interobserver bias.
Radiologic Evaluation
Preoperative whole-leg weightbearing anteroposterior radiographs were used to evaluate the weightbearing line (WBL) ratio and hip-knee-ankle (HKA) angle. The WBL was drawn from the center of the femoral head to the center of the talar joint surface. The WBL ratio was calculated as the percentage of the distance from the medial edge of the tibial plateau to the crossing point made by the mechanical axis and proximal tibial plateau and the entire width of the tibial plateau (the medial tibial edge at 0% and the lateral tibial edge at 100%). The HKA angle was defined as the angle between the line from the center of the femoral head to the center of the proximal tibia and the line from the center of the proximal tibia to the center of the tibial plafond on the weightbearing whole-leg radiograph. An INFINITT Version 5.0.9.2 picture archiving and communication system (PACS) was used for the quantitative measurements.
MRI Evaluation
MRI images were obtained preoperatively and at the follow-up assessment >1 year after MAT using a 3-T magnetic resonance scanner (Achieva; Philips Medical Systems). Images were acquired with the patient in the standard position and the affected knee fixed with an immobilizing device on the lower limb. MRI Digital Imaging and Communications in Medicine (DICOM) data were extracted from the INFINITT PACS and imported into a DICOM viewer (RadiAnt DICOM Viewer 2020.2.2; Medixant Company; open-source software available at http://www.radiantviewer.com). The imported MRI scan was transformed into an arbitrary plane aligned with the direction of the meniscal insertion axis using a 3-dimensional multiplanar reconstruction tool. The yellow line surrounding the meniscus is the ROI.
Meniscal Position
To determine the position of the menisci, we used the percentage reference method described by Wilmes et al 28 and modified for MRI by Kim et al. 11,12 First, the midpoints of the anterior root and posterior root of the menisci were identified. Then, the relative distance between the lateral edge of the tibial plateau and the anterior and posterior root of the menisci was calculated on coronal MRI, as described in Figure 3. At the midpoint of the anterior-to-posterior width of the proximal tibia, 2 tangential lines were drawn to the medial (M) and lateral (L) borders of the tibial plateau. The broadest tibial attachment of the horns was determined as the tibial insertion on another coronal MRI scan. These images were then merged using Adobe Photoshop CS6 software Version 13.0.1 (Adobe Systems Inc). The distance between the tibial insertion (X or Y) and lateral border (L) was divided by the distance of the tibial plateau width (line ML) on the merged image (Figure 3, D and H).

(A-D) Measurement of the distance between the lateral edge of the tibial plateau and the MMAR or MMPR on coronal MRI. (A) M and L are tangential to the medial and lateral tibial plateau at the midpoint of the anterior-to-posterior width of the proximal tibia, (B) X indicates the MMAR midpoint, (C) Y indicates the MMPR midpoint, and (D) line ML defines the tibial width. The distance from L to X and L to Y were measured. (E-H) Measurement of the distance between the lateral edge of the tibial plateau and the LMAR or LMPR on coronal MRI. (E) M and L are tangential to the medial and lateral tibial plateau at the midpoint of the anterior-to-posterior width of the proximal tibia, (F) X indicates the LMAR midpoint, (G) Y indicates the LMPR midpoint, and (F) line ML defines the tibial width. The distance from L to X and L to Y were measured. LMAR, lateral meniscal anterior root; LMPR, lateral meniscal posterior root; MMAR, medial meniscal anterior root; MMPR, medial meniscal posterior root; MRI, magnetic resonance imaging.
The relative distance between the anterior edge of the tibial plateau and the anterior and posterior root of the menisci was calculated on sagittal MRI, as described in Figure 4. On the sagittal plane crossing the midline of the knee, an anterior line parallel to the anterior border of the tibial plateau (A) and a posterior line tangent to the bony ridge of the posterior intercondylar area and parallel to the tibial shaft (P) were drawn. Line AP was drawn perpendicular to the posterior line and tangential to the intercondylar spine. The broadest tibial attachment of the horns was determined as a tibial insertion on another sagittal MRI scan, and the images were then merged. The root position in the sagittal plane was calculated by dividing the distance between the tibial insertion (X or Y) and the anterior border (A) by the distance of the tibial plateau width (line AP) on the merged image (Figure 4, D and H).

(A-D) Measurement of the distance between the anterior edge of the tibial plateau and the MMAR or MMPR on sagittal MRI. (A) P is parallel to the posterior cortex of the tibial shaft, tangential from the posterior intercondylar area into the tibial shaft. A is parallel to the anterior border of the tibial plateau. (B) X indicates the MMAR midpoint, while (C) Y indicates the MMPR midpoint. (D) Line AP was drawn perpendicular to the posterior line and tangential to the intercondylar spine. The distance from A to X and A to Y were measured. (E-H) Measurement of the distance between the anterior edge of the tibial plateau and the LMAR or LMPR on sagittal MRI. (E) P is parallel to the posterior cortex of the tibial shaft, tangential from the posterior intercondylar area into the tibial shaft. A is parallel to the anterior border of the tibial plateau. (F) X indicates the LMAR midpoint, and (G) Y indicates the LMPR midpoint. (H) Line AP was drawn perpendicular to the posterior line and tangential to the intercondylar spine. The distance from A to X and A to Y were measured. LMAR, lateral meniscal anterior root; LMPR, lateral meniscal posterior root; MMAR, medial meniscal anterior root; MMPR, medial meniscal posterior root; MRI, magnetic resonance imaging.
Meniscal Rotation, Insertion, and Slope
The 0° rotation line was defined as a line perpendicular to the posterior tibial condylar tangential line at the level just below the meniscus. The angle between the 0° rotation line and the line connecting the centers of the anterior root and posterior root was determined as the rotation angle (Figure 5, A-C).

(A) The 0° rotation line is defined as a line perpendicular to a posterior tibial condylar tangential line at the level just below the meniscus; compared with the initial angle, external rotation was denoted with positive values (+) and internal rotation was denoted with negative values (–). (B and C) The angle between the 0° rotation line and the line connecting the centers of the anterior root and posterior root (red lines) was determined as the rotation angle. (D and E) MRI of a 41-year-old male patient who underwent MMAT on his left knee. Compared to the preoperative value (D), the medial meniscus was more internally rotated (E). (F) Meniscal extrusion was defined as the distance from the tibial plateau to the outer edge of the meniscus on coronal MRI. MMAT, medial meniscal allograft transplantation; MRI, magnetic resonance imaging.
To assess the meniscal insertion and slope, the sagittal anatomical axis of the tibia was first determined. The line connecting 2 points located at the middle of the proximal tibial shaft was chosen as the axis in a sagittal scan in proximity to the posterior cruciate ligament insertion. 5,16 The meniscal insertion angle was measured between the line connecting the center of the anterior and posterior horns at the tibial insertion of the meniscus and perpendicular line of the anatomical axis of the tibia on sagittal MRI. The meniscal slope was measured as the angle between the line perpendicular to the tibial anatomical axis and the line connecting the superior border of the anterior and posterior horns of the meniscus. The angle between the line perpendicular to the anatomical axis of the tibia and the line of the tibial bony surface was measured for the bony slope. Because the bony surface of the tibial plateau has a curved configuration, the line connecting the inferior borders between the anterior and posterior horn was used as the line of tibial bony surface. 16 Downward slope was reported using positive values, and upward slope was reported using negative values.
Meniscal Extrusion and Intrameniscal Signal Intensity
Extrusion of the meniscus, defined as the largest distance from the peripheral aspect of the meniscus to the border of the tibial plateau, was measured according to the method described by Verdonk et al 26 excluding any osteophytes on coronal MRI (Figure 5F). 4 The extruded distance of the meniscus beyond the outer margin of the tibial plateau was measured as the absolute value of extrusion. For standardization of individual knee size, the relative ratio of extrusion was calculated as the absolute value of extrusion divided by the entire width of the meniscus. 19
The intrameniscal signal intensity of the transplanted graft was measured using a region-of-interest (ROI) tool on the INFINITT PACS. The ROI area was marked by arbitrary fixed points bordering the maximum area of the anterior horn and posterior horn of the allograft. The ROI of the transplanted meniscal allograft compared to that of the control normal meniscus was used to standardize the signal intensity (Figure 6). To quantify the normalized signal intensity of the ACL graft, the signal-to-noise ratios of each graft site were calculated using the ROI technique (circular markings 3.3 mm in diameter).

Magnetic resonance imaging scan shows the ROI method used to determine mean signal intensity for transplanted grafts. ROI is a circle formed by setting the maximum area of the anterior and posterior horns of the meniscus (yellow circle) is marked by taking arbitrary fixed points bordering the maximum area of the anterior horn and posterior horn of the allograft. ROI, region of interest.
Clinical Evaluation
Clinical evaluations were performed before surgery and at subsequent follow-up using the International Knee Documentation Committee (IKDC) and Lysholm scores. The IKDC score consists of subjective and objective subscales. For the subjective score, a higher score on a scale of 0 to100 indicates a better outcome. The objective score includes 4 grades, from the best score of A to the worst score of D. The Lysholm score also has a range of values from 0 to 100, with higher scores indicating a better outcome. Clinical outcomes were obtained by a physician assistant blinded to the information about the study and the patients.
Statistical Analysis
A post hoc power analysis of the study was performed using G*Power (Version 3.1.9.7). The inter- and intraobserver measurement reliabilities were assessed using intraclass correlation coefficients (ICCs), in which an ICC of <0.40 indicates poor agreement, 0.40 to 0.75 indicates fair to good (moderate) agreement, and 0.76 to 1.00 indicates excellent agreement.
Data were reported as means and standard deviations for continuous variables. According to the normality test results, continuous variables were compared between groups using the Mann-Whitney test. In each group, pre- and postoperative measurements were evaluated using the Wilcoxon signed-rank test according to the results of the normality test. The difference in the IKDC objective score between groups was analyzed using the chi-square test and Fisher exact test. All statistical analyses were performed using SPSS Version 25.0 (IBM Corp). The level of significance was set at P < .05.
Results
The mean follow-up period was 41.15 ± 18.86 and 45.43 ± 21.32 months for the MMAT and LMAT groups, respectively. According to post-hoc power analysis, the statistical power of this study was 0.99 (0.998). The intra- and interobserver agreements were excellent (ICC, 0.818-0.831) on the anterior stability evaluations and good (ICC, 0.713-0.750) on the MRI assessments.
The demographics and baseline characteristics are listed in Table 1. There was no statistically significant difference in demographics and preoperative radiologic parameters between the MMAT and LMAT groups.
Demographics and Baseline Characteristics a
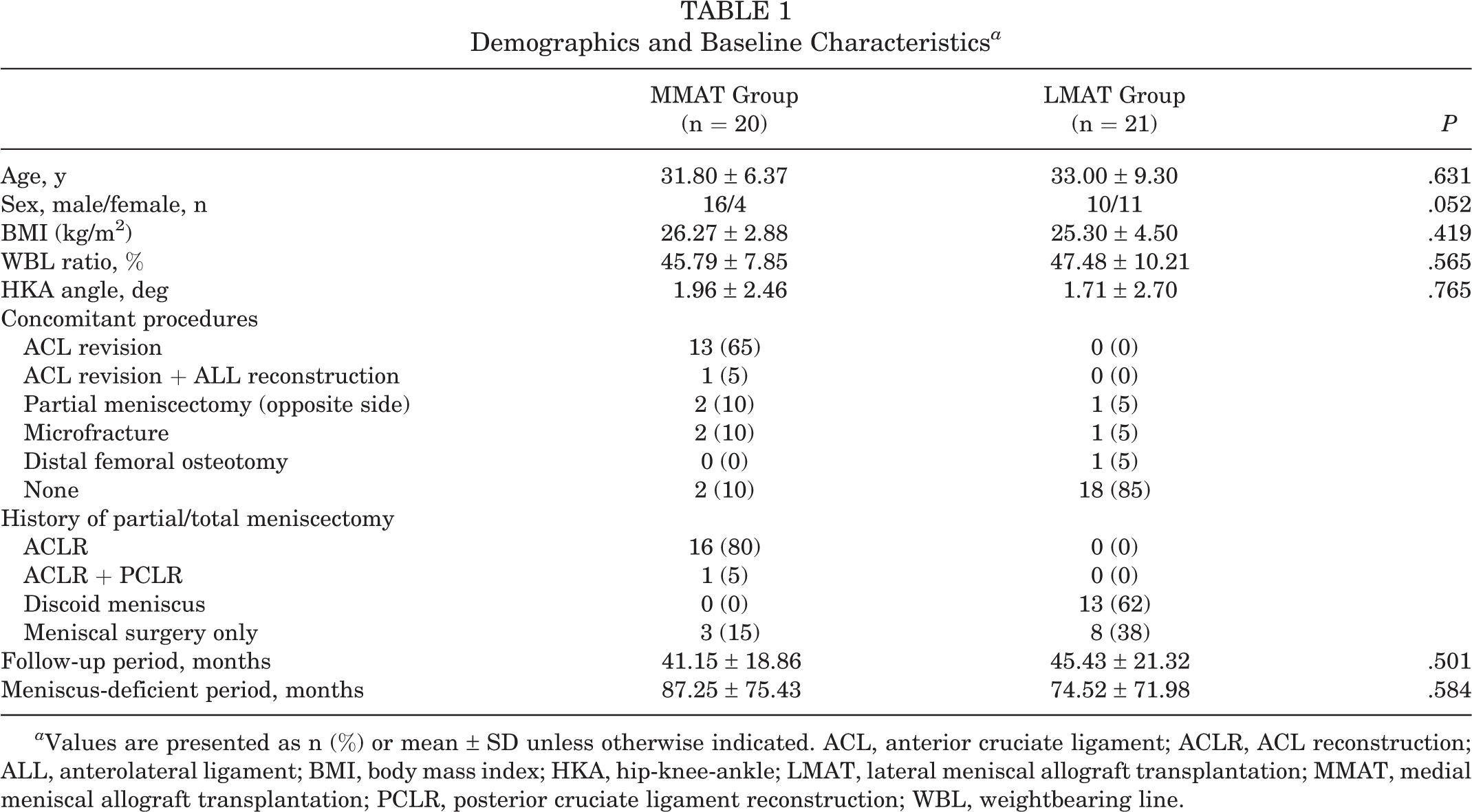
a Values are presented as n (%) or mean ± SD unless otherwise indicated. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; ALL, anterolateral ligament; BMI, body mass index; HKA, hip-knee-ankle; LMAT, lateral meniscal allograft transplantation; MMAT, medial meniscal allograft transplantation; PCLR, posterior cruciate ligament reconstruction; WBL, weightbearing line.
For the MMAT group, concomitant procedures were performed in 90% of cases. Among them, 13 (65%) were accompanied by revision ACL reconstruction (ACLR). In 1 patient, revision ACLR and anterolateral ligament reconstruction were performed. Contralateral partial meniscectomy was performed in 2 patients in the MMAT group and 1 patient in the LMAT group. Microfracture of the involved femoral condyle was necessary in 2 patients in the MMAT group (International Cartilage Regeneration & Joint Preservation Society [ICRS] grade 3; lesion size, 2 × 2.5 cm2 and 3 × 2 cm2, respectively) and 1 patient in the LMAT group (ICRS grade 3; lesion size, 2 × 2.5 cm2). Alignment correction was performed using distal femoral osteotomy in 1 patient in the LMAT group. For the LMAT group, isolated procedures were performed in 85% (n = 18) of patients. Interestingly, before MAT, 80% of patients had undergone ACLR in the MMAT group, and 62% had undergone meniscectomy for a discoid lateral meniscus in the LMAT group. Regarding the interval between index surgery and MAT after total meniscectomy, MMAT and LMAT were performed at 87.25 ± 75.43 and 74.52 ± 71.98 months, respectively (Table 1).
MRI Outcomes
The comparison of parameters between anatomic and restored meniscal position in the MMAT and LMAT groups is summarized in Table 2. Overall, LMAT was performed more anatomically than MMAT. In the LMAT group, there was no statistically significant difference between the native and postoperative root positions. In the MMAT group, compared with the native position, the anterior root was located more posteriorly (preoperative 4.55 ± 2.73 mm, postoperative 7.10 ± 2.74 mm; P = .002) and medially (preoperative 40.55 ± 4.90 mm, postoperative 43.60 ± 5.22 mm; P = .007) in the sagittal and coronal planes, respectively. However, there was no significant difference between the preoperative and postoperative positions of the posterior root. LMAT restored native rotation, but the medial meniscus after MMAT was more internally rotated on average (from 3.19° ± 1.09° to 2.02° ± 1.90°; P = .029) (Table 2 and Figure 5, D and E).
Original and Restored Meniscal Position, Rotation, Insertion, and Slope a

a Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between preoperative and postoperative values (P < .05). LMAT, lateral meniscal allograft transplantation; MMAT, medial meniscal allograft transplantation.
b Negative values indicate upslope.
When comparing meniscal extrusion, there was a significant difference between MMAT and LMAT in all meniscal regions (P < .001 at the posterior horn, .027 at the midbody, and .006 at the anterior horn), and MMAT showed, on average, approximately 1 to 3 mm more extrusion in all areas. There were no differences between the MMAT and LMAT groups in the intrameniscal signal intensity at either area (Table 3).
Meniscal Extrusion and Intrameniscal Signal Intensity a

a Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). LMAT, lateral meniscal allograft transplantation; MMAT, medial meniscal allograft transplantation.
b Data in parentheses indicate relative ratio of extrusion.
In a subgroup analysis, no significant difference was observed postoperatively between combined MMAT and ACLR versus isolated MMAT (Table 4).
Comparison Between Combined ACLR and Isolated MMAT a

a Values are presented as mean ± SD or No. of patients. Boldface P value indicates statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; IKDC-O: International Knee Documentation Committee objective score; IKDC-S, International Knee Documentation Committee subjective score; MMAT, medial meniscal allograft transplantation.
Clinical Outcomes and Complications
Significant pre- to postoperative improvements were observed in both the MMAT and the LMAT groups on the IKDC subjective score, IKDC objective score, and Lysholm score (P < .001 for all). In addition, there was no significant difference in the final follow-up clinical scores between the 2 groups (Table 5). There were no specific fixation-related complications or adverse events in either group.
Comparison of Clinical Outcomes Between MMAT and LMAT a

a Values are presented as mean ± SD or No. of patients. IKDC-O, International Knee Documentation Committee objective score; IKDC-S, International Knee Documentation Committee subjective score; LMAT, lateral meniscal allograft transplantation; MMAT, medial meniscal allograft transplantation.
Discussion
The principal findings of this study were that clinical outcomes were improved after both MMAT and LMAT compared with preoperative values, and there was no significant difference in midterm clinical outcomes between the 2 groups. However, radiological outcomes were different. In particular, a significant difference was observed between the location of the anterior root and the meniscal rotation on follow-up MRI. In the MMAT group, there were many cases of ACL revision or primary ACLR, and it was assumed that the ACL tibial tunnel could be an obstacle in making the anterior horn tunnel. In addition, the anterior horn tunnel was created using retro-reaming, and posterior shifting was inevitable to prevent anterior cortical breakage. In the subgroup analysis, the locations of the MMAR and medial meniscal posterior root (MMPR) tended to be positioned laterally in patients undergoing combined procedures. It is thought that the overall lateral shift occurred during the process of intentionally drilling the tunnel to avoid breakage due to communication with the ACL tibial tunnel. However, no significant difference was observed between combined MMAT and isolated MMAT in the subgroup analysis. The degree of meniscal extrusion was significantly lower after LMAT versus MMAT. It was assumed that anatomic restoration and firm attachment to the native bone block made extrusion less likely.
Improved clinical outcomes are generally reported after MMAT and LMAT. Yoon et al 30 described a statistically significant improvement in visual analog scale (VAS) score, IKDC subjective score, Lysholm score, Tegner activity score, and patient subjective score in the LMAT and MMAT groups in a retrospective series of 91 patients with a mean follow-up of 40 months. However, there was no significant difference in the clinical results between MMAT and LMAT. Verdonk et al 27 also reported that both the MMAT and LMAT groups showed improved results in pain and walking scores. Significant pain reduction and increased activity in 85% of patients receiving MAT was detailed by Lee et al. 15 These results correspond with the results of this study, with similar follow-up periods. Additionally, according to a meta-analysis reported by Bin et al, 1 midterm and long-term survival rates were not different between MMAT and LMAT (287 and 407 knees, respectively), but pain relief was significantly better in LMAT.
The MMPH is a secondary anterior stabilizer of the knee and is known to play a role in limiting anterior tibial translation in ACL-injured knees. 15 Zaffagnini et al 31 reported that MMAT with concomitant primary or revision ACLR yielded better results than LMAT in knees with ACL injury or failure of ACLR after meniscectomy. MMAT improved rotational stability as well as anterior posterior stability in a retrospective study by Yoon et al 29 investigating 16 cases of MMAT and 15 cases of LMAT with previous ACLR. In a meta-analysis of 24 studies that compared isolated MAT and combined MAT no significant difference was found in Lysholm, Tegner activity, IKDC subjective, or VAS scores. 17 However, in a retrospective analysis of 6 isolated and 29 combined cases, Yoon et al 30 reported better clinical outcomes in the isolated MAT than combined with MAT. In the current study, there was no significant difference between the isolated and combined groups in IKDC subjective, IKDC objective, or Lysholm scores.
Accurate positioning of a meniscal allograft is thought to be an important factor for successful outcomes after MAT. 14,23 The nonanatomic graft position can cause disadvantages in knee biomechanics. In particular, when the graft position is >5 mm away from the native meniscus, it can affect the contact pressure and adversely affect the cartilage prevention ability of the graft. 13,24 In this study, the anterior root position differed by 2 to 3 mm compared with the preoperative native position. However, our results suggest that this postoperative change has little biomechanical or clinical relevance since there was no difference in intrameniscal signal intensity and clinical outcome between LMAT and MMAT. Because of the anatomical situation where the anterior and posterior horn of the lateral meniscus are close together, breakage may occur due to tunnel communication in the case of the bone plug technique, so the bone bridge technique is usually performed in LMAT. 15 Kim et al 13 reported that postoperative transplanted meniscal position change was occurred less than 5% (relative values) and 5 mm (absolute value). Misplacement of the meniscal allograft is a major cause of transplantation failure. 16 In this study, there was no statistical difference in the position of MMPR pre- and postoperatively, but there was a posteromedial translation compared with the native medial meniscus in MMAR, although the graft deviation was <5 mm. In particular, the anterior root showed a statistically significant difference in the sagittal and coronal planes (P = .002 and .006, respectively) and more internal rotation (P = .029) in rotation angle.
There are several reasons why the location of the anterior root showed a posteromedial translation and internal rotation. The anterior tunnel was measured as medial because it was made as lateral as possible, but it is thought that the allograft was pulled to the medial within the tunnel entrance after meniscal repair and tying of the pulling suture of both roots, which pulled the menisci medially (Figure 5D). Because the location of the MMAR tunnel was not sufficiently lateral, posterior positioning was performed to prevent excessive extrusion in consideration of the meniscal size. If the posterior root was too medialized without considering the anterior root position, the meniscus can be redundant and there would be a possibility of meniscal extrusion. In addition, the tunnel was moved posteriorly to avoid breakage of the anterior cortical rim because retro-reaming was performed using the Flipcutter. It is difficult to access the MMPR using the anterior portal; therefore, the surgeon tried to determine the exact location of the posterior horn using the posterior transseptal portal and was able to position the tunnel very close to the native posterior horn of the medial meniscus.
The difference in surgical technique between MMAT and LMAT (bone plug vs keyhole) causes a variation in allograft extrusion. In general, the extrusion rate was higher in MMAT than LMAT. 18 However, Ha et al 8 and Lee et al 18 reported that extrusion was not associated with early clinical outcomes and radiologic or arthroscopic outcomes. Similarly, in this study, extrusion was also significantly greater in MMAT than in LMAT, with no difference in clinical results between the 2 groups. The extent of extrusion was slightly smaller than that in previously reported cases. We assume that this lesser extrusion was achieved through intentional adjustment of the tunnel position, especially the anterior horn of the medial meniscus, and firm repair of the meniscus with the residual peripheral rim of the original meniscus. This may be a strength of this study.
Limitations
There were several limitations to this study. First, the surgical technique was different between the 2 study groups, making it difficult to compare them. Second, there were many cases with instability in MMAT as a secondary knee stabilizer, and more cases of concomitant operation than LMAT. This heterogeneity made it difficult to compare the 2 groups under similar conditions. Therefore, it will be necessary to compare the 2 groups by securing sufficient cases of isolated MMAT in the future. Third, the number of patients was too small to perform subgroup analysis between isolated MMAT and combined MAT with other procedures. Fourth, the evaluation tool was not sensitive enough to identify the biomechanical effect of such a small difference. Finally, the mean follow-up period was <5 years, and longer-term follow-up is still necessary.
Conclusion
LMAT using the keyhole technique showed higher accuracy than MMAT using the bone plug technique in restoring meniscal location and rotation. It also showed lesser extrusion in all areas. However, clinical scores improved after both LMAT and MMAT compared with preoperative values, and midterm clinical outcomes were not significantly different. The small anatomical errors seen in the MMAT technique were not clinically relevant at midterm follow-up.
Footnotes
Final revision submitted April 14, 2022; accepted May 16, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Research Foundation of Korea grant funded by the Korean Ministry of Science and Information and Communication Technologies (No. 2021R1A2C1092657). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Bundang Hospital (ref No. B-2105/682-101).