
Abstract
Background:
Predictive factors influencing outcomes after surgical fixation of osteochondral fractures (OCFs) in the knee, particularly time between injury and surgery, have not been determined.
Purpose:
To report imaging and clinical outcomes after OCF fixation and to assess the association between clinical scores and patient characteristics, lesion morphology, and appearance on magnetic resonance imaging (MRI) scans.
Study Design:
Case series; Level of evidence, 4.
Methods:
We assessed the clinical and imaging outcomes of 19 patients after screw fixation for OCFs in the knee at a minimum follow-up of 1 year. Patient characteristics, lesion morphology, and time from trauma to surgery were reviewed for each patient. At final follow-up, patients completed a 100-point visual analog scale (VAS) for pain, Tegner activity scale, Knee injury and Osteoarthritis Outcome Score (KOOS), and patient satisfaction survey. Postoperative MRI scans were assessed using the MOCART (magnetic resonance observation of cartilage repair tissue), Osteochondral Allograft MRI Scoring System, and bone marrow edema (BME) size.
Results:
The mean patient age at surgery was 21.3 ± 11.4 years, and the median time from trauma to surgery was 10 days (range, 0-143 days). The refixed OCF fragment failed in 1 (5.3%) patient on the lateral condyle at 15 months postoperatively. The mean follow-up for the remaining 18 patients was 4.7 ± 3.2 years, and postoperative outcomes were as follows: VAS pain score, 9.5 ± 17.9; Tegner score, 4.8 ± 2.3; KOOS–Pain, 85.9 ± 17.6, KOOS-Symptoms, 76.4 ± 16.1; KOOS–Activities of Daily Living, 90.3 ± 19.0; KOOS–Sport, 74.4 ± 25.4; and KOOS–Quality of Life, 55.9 ± 24.7. Overall, 84.2% were satisfied or very satisfied with outcomes. Patient age was significantly associated with KOOS subscale scores and subchondral imaging parameters including BME and presence of subchondral cysts, which in turn were the only imaging variables linked to clinical outcomes (P < .05). Time from injury to surgery was not correlated with clinical or imaging outcomes.
Conclusion:
Fixation of OCFs yielded acceptable clinical and imaging outcomes at a mean 5-year follow-up with seemingly little influence of delayed surgical treatment. Postoperative subchondral changes were significantly associated with clinical outcomes and were linked to patient age at surgery.
Osteochondral fractures (OCFs) of the knee joint can result from direct trauma or patellar dislocation, particularly in the pediatric and adolescent populations. 2,6,19,21,22,28 Consequent loose bodies frequently cause discomfort and mechanical issues to the patient, and the osteochondral defect might progress to osteoarthritis. 9,36 Yet, the treatment of such injuries is still controversial and usually depends on lesion size and location, as well as on the condition of the fragment. 15 While smaller lesions can be managed conservatively, larger fragments usually represent a surgical indication and undergo fixation, debridement, or cartilage restoration. 16 A recent study reported that fragment fixation yields good mid- to long-term clinical outcomes in patients with large OCFs of the patella. Due to the superior results seen when compared with debridement, the authors recommended fragment fixation whenever possible. 11
Even though fixation seems to be the preferred surgical technique for patients with OCFs, the current literature is limited to case reports and studies with short follow-up periods. 1,7,18 While the provided evidence does not allow for a reliable conclusion of parameters influencing the outcome of OCF fixation, studies investigating osteochondral allograft transplantation (OCA) and osteochondral autograft transplantation have consistently reported increasing age as a risk factor for graft failure. 17,33 In addition, there is an unmet need for imaging studies evaluating postoperative cartilage quality and progression of disease after the fixation of OCFs.
Aside from patient characteristics, chondrocyte viability of the osteochondral fragment is another important aspect of OCF fixation. Chondrocyte viability has been deemed one of the key parameters for graft survival in the transplantation of osteochondral units in the knee. 24,26 While a prior small case series reported a close-to-native chondrocyte viability in loose osteochondritis dissecans fragments, 34 we have also learned from OCA studies that chondrocyte viability falls below the generally acceptable level of 70% by 28 days of storage in a nutrient medium, which seems to have a marked effect on postoperative graft survival. 8,26,32 In fact, a recent study has shown that OCAs that are transplanted later than 24 days are 3.4 times more likely to fail compared with their age- and size-matched controls that have been implanted between 19 and 24 days after harvesting. 24
Despite the challenging comparison of the effect of an in vitro storage condition (OCA storage) to an in vivo environment (OCF fragment in the knee joint), we wondered whether time from trauma to surgery has a similar deleterious effect on the cartilage quality of loose osteochondral fragments in patients with acute OCFs. Although the effect of patient- and lesion-specific variables or delayed fixation are of high clinical relevance as stressed by Kuhle et al 16 in a systematic review and meta-analysis in 2013, surprisingly little evidence is provided by the current literature.
The purpose of this study was to report the imaging and clinical outcomes after OCF fixation and to assess the associations among patient characteristics, lesion morphology, magnetic resonance imaging (MRI) appearance, and patient outcomes. We hypothesized that time from trauma to surgery and patient age would be inversely correlated with imaging and clinical outcomes.
Methods
Ethical approval was granted by the local research ethics committee, and all included patients gave their written consent.
Patients
We retrospectively identified a total of 28 consecutive patients who underwent open fixation of an osteochondral fragment at one of our institutions between October 2009 and February 2020. Inclusion criteria comprised the treatment of OCF with screw fixation for the diagnosis of a free osteochondral fragment caused by an OCF due to a traumatic event. Patients were excluded from the current study if follow-up was <1 year, preoperative imaging suggested an unstable osteochondritis dissecans, or intraoperative imaging showed a purely chondral flap without attached subchondral bone. Consequently, 21 patients were eligible for study enrollment, but 2 patients were not available for follow-up, as both refused to participate. Thus, this study assessed the outcome of 19 patients (90.5%) who received osteochondral screw fixation at a minimum follow-up of 1 year.
Clinical Assessment
Clinical notes and operative reports were reviewed to determine the patient’s age at the time of surgery, sex, body mass index (BMI), time from trauma to surgery, concomitant surgical procedures, defect size, location, number of screws, complications, and reoperations.
Patients were contacted via telephone and were invited for a clinical examination at our institution including the assessment of standardized patient-reported outcome measures and postoperative MRI scans. Clinical outcomes were evaluated using the Tegner activity scale (maximum sporting activity their knee allowed or maximum sporting activity they frequently performed if general sports were quit because of fear of reinjury or symptoms getting worse), 41 the Knee injury and Osteoarthritis Outcome Score (KOOS) with its subscales (Pain, Symptoms, Activities of Daily Living [ADL], Sport and Recreation [Sport], and Quality of Life [QOL]), 35 and the visual analog scale (VAS; range, 0-100) for pain during daily activities and pain during sports and running. 3 In an attempt to mirror preoperative clinical scores, we asked patients to retrospectively rate their knee using the Tegner activity scale for the time point after injury but before surgery. Patients were also asked to rate their overall postoperative outcome as “excellent,” “good,” “fair,” or “unsatisfactory.”
MRI Assessment
At final follow-up, all patients underwent a dedicated MRI examination of the respective knee joint using either a 7-T MRI system (MAGNETOM Terra; Siemens Healthcare) with a dedicated 28-channel transmit/receive knee coil (n = 16) or a 3-T MRI scanner (MAGNETOM Prisma; Siemens Healthcare) with a 15-channel transmit/receive knee coil (n = 3). Image protocol comprised intermediate-weighted turbo spin-echo sequences with frequency-selective fat suppression in the transverse, coronal, and sagittal planes, and a T1-weighted turbo spin-echo sequence without fat saturation in the coronal plane (slice thickness, 2.5-3 mm).
A musculoskeletal fellowship–trained board-certified radiologist with 8 years of experience (C.G.) assessed the fixed osteochondral fragment utilizing the previously published and validated comprehensive MOCART 2.0 (magnetic resonance observation of cartilage repair tissue) score, 38 the Osteochondral Allograft MRI Scoring System (OCAMRISS), 5,23 and bone marrow edema (BME) evaluation according to Henderson et al. 12
Surgical Technique and Postoperative Care
The treatment with osteochondral fragment fixation with screw osteosynthesis was indicated in patients with a symptomatic fresh traumatic OCF with an intact fragment containing subchondral bone for adequate fixation.
The OCF for all patients was accessed via arthrotomy using an open approach. The defect site and the loose fragment were identified, and the fragment was thoroughly inspected. If the fragment contained subchondral bone, the decision was made to reattach the fragment to the defect site. Both the defect and the fragment were carefully debrided until good fit was achieved. In the case of a large bony defect, autologous cancellous bone from the ipsilateral tibia or femur was impacted into the defect before fragment fixation. The OCF fragment was then fixed with 1 or several 2.0-mm cortical screws, depending on fragment size (Figure 1). To ensure stable fixation, we brought the joint through full range of motion. Concomitant surgery for coexisting pathologies was performed as indicated. Arthrotomy was closed using running absorbable sutures followed by standard wound closure.

(A) Osteochondral fragment deriving from the lateral femoral condyle and (B) intraoperative imaging of fragment fixation with 3 cortical screws.
Postoperative Rehabilitation
After surgery, patients were immobilized in a knee brace with protected partial weightbearing for the first 4 to 6 weeks. Stepwise increase of active and passive range of motion was emphasized to avoid arthrofibrosis. Then, the brace was removed, and full weightbearing was allowed. At approximately 12 weeks, all patients underwent surgical mini-open screw removal with postoperative full weightbearing.
Statistical Analysis
Sociodemographic and clinical characteristics of patients are presented using descriptive statistics. Data were assessed for normality utilizing the Shapiro-Wilk test. Subsequently, the paired t test was utilized to analyze the change in patient activity (Tegner score) from preinjury to postoperatively. Pearson and point biserial correlations were used to assess the relationship of patient characteristics, imaging outcomes, and clinical outcomes. Patients were also stratified into late and early fixation groups (≤30 vs >30 days). Clinical and imaging outcomes were compared using the Fisher exact and Mann-Whitney U tests as indicated. All statistical analyses were performed using SPSS for Mac Version 23.0 (SPSS Inc). Significance was set at P ≤ .05.
Results
The assessed cohort included 19 patients with a mean age at the time of surgery of 21.3 ± 11.4 years and time from trauma to surgery in the range of 0 to 143 days (median, 10 days). Of these patients, 14 (73.7%) underwent surgery within 30 days of the traumatic event. Patients with an intact OCF fragment were evaluated at a mean follow-up of 4.7 ± 3.2 years (range, 1-10 years). Of the included patients, 9 (47.4%) underwent concomitant surgery for coexisting pathologies such as patellar instability, ligament insufficiency, or concomitant cartilage defects. Traumatic injury due to patellar dislocation was reported in 12 (63.2%) knees. A summary of patient and injury characteristics is in Table 1.
Patient and Lesion Characteristics (N = 19) a
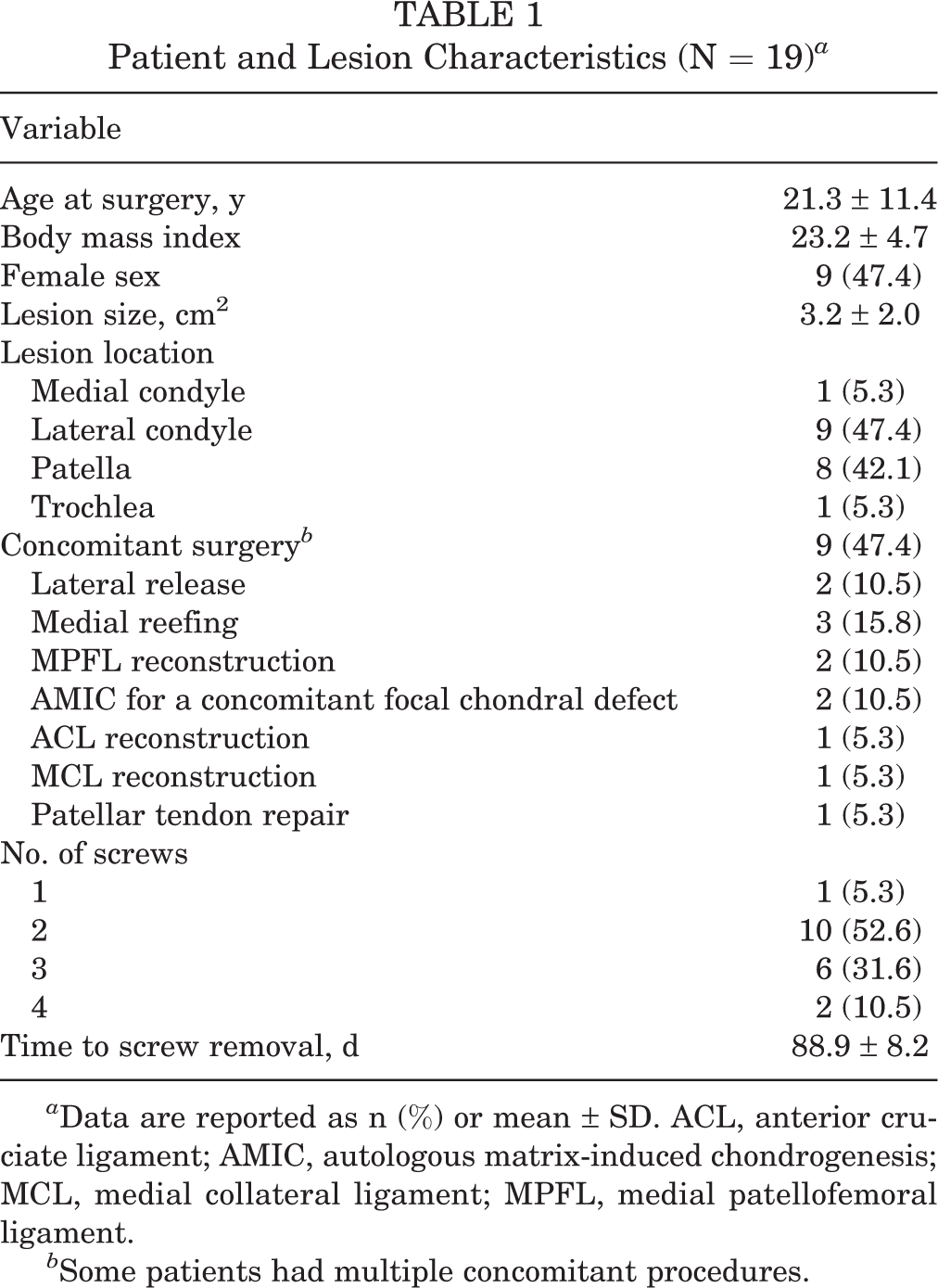
a Data are reported as n (%) or mean ± SD. ACL, anterior cruciate ligament; AMIC, autologous matrix-induced chondrogenesis; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament.
b Some patients had multiple concomitant procedures.
Complications and Reoperations
During the study period, the refixed OCF fragment, which was fixed within 8 days of the trauma, failed in 1 (5.3%) patient on the lateral condyle at 15 months postoperatively. This was treated using loose body removal, autologous matrix-induced chondrogenesis, and closed-wedge distal femoral osteotomy. Additionally, a further 5 (26.3%) patients underwent reoperations, of which 3 (15.8%) were tibial tubercle osteotomies, 3 (15.8%) were medial patellofemoral ligament reconstructions, 1 (5.3%) was a trochleoplasty, and 1 (5.3%) was a high tibial osteotomy with concomitant autologous matrix-induced chondrogenesis for a cartilage defect at a new location.
Clinical Outcomes
At final follow-up, patients with an intact refixed OCF fragment (n = 18; 94.7%) had mean pain VAS scores of 9.5 ± 17.9 during daily activities and 25.9 ± 27.3 during sports, as well as KOOS subscale scores of 85.9 ± 17.6 for Pain, 76.4 ± 16.1 for Symptoms, 90.3 ± 19.0 for ADL, 74.4 ± 25.4 for Sport, and 55.9 ± 24.7 for QOL. The mean Tegner score significantly declined from 5.8 ± 2.3 preinjury to 4.8 ± 2.3 postoperatively (P = .01).
Generally, 47.4% of patients reported that they were very satisfied with the result of the surgery, 36.8% were satisfied, and 15.8% were rather unsatisfied at final follow-up.
MRI Outcomes
The 18 patients with remaining in situ OCF fragment demonstrated a mean OCAMRISS of 6.6 ± 1.8 and MOCART 2.0 score of 65.8 ± 9.1. At final follow-up, 4 (22.2%) patients presented without a BME; 11 (61.1%) patients, with a mild BME; and 3 (16.7%) patients, with a moderate BME according to the Henderson scale (Table 2). 12 The majority of patients (55.6%) showed subchondral cyst formation with a mean cyst size of 2.5 ± 1.1 mm. All osteochondral fragments displayed full osseous integration, with 77.8% also showing cartilage edge integration. All patients showed an irregularity of the subchondral plate, with 1 (5.6%) patient showing subchondral sclerosis. The volume fill of the cartilage layer was still complete in 72.2% and slightly underfilled (75%-99% volume fill) in 27.8% of patients. The cartilage surface was intact in 27.8%, irregular along <50% of the defect diameter in 55.6%, and irregular along >50% in 16.7% of patients (Figure 2).
Characteristics and Outcomes of the Patients With Intact Osteochondral Fragment (n = 18) a
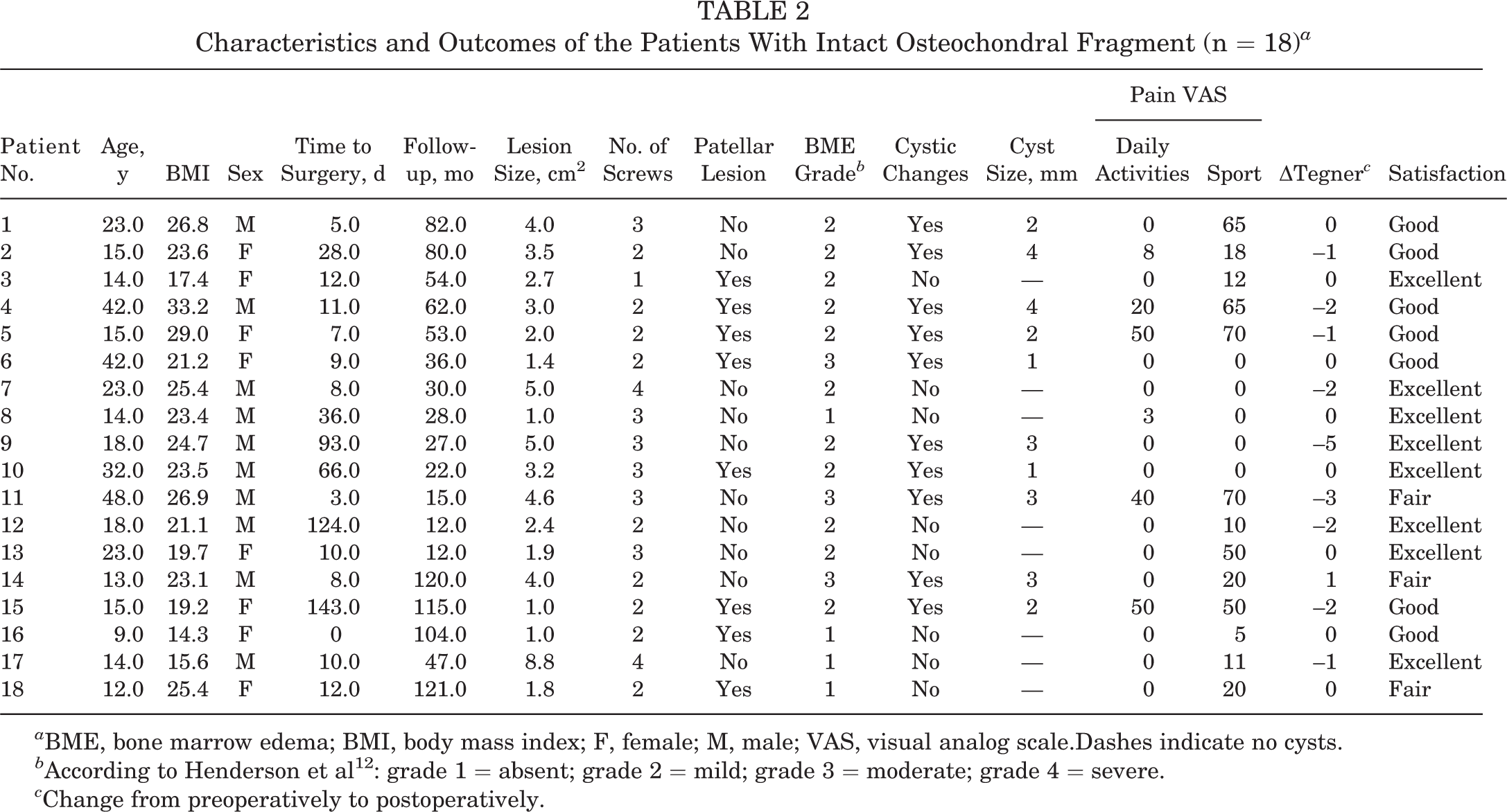
a BME, bone marrow edema; BMI, body mass index; F, female; M, male; VAS, visual analog scale.Dashes indicate no cysts.
b According to Henderson et al 12 : grade 1 = absent; grade 2 = mild; grade 3 = moderate; grade 4 = severe.
c Change from preoperatively to postoperatively.

Postoperative fat-saturated 7-T magnetic resonance imaging scans in the sagittal plane showing varying degrees of subchondral changes (bone marrow edema and cyst formation) in patients after osteochondral fracture fixation of the lateral femoral condyle: (A) grade 3 (moderate); (B) grade 2 (mild); and (C) grade 1 (absent).
Of the 18 patients, 11 (61.1%) had at least 1 additional postoperative MRI in the study period. Of these, 8 (72.7%) showed a regression of the BME over time, 1 (9.1%) patient had an increase in size of the BME, and 2 (18.2%) patients had an unchanged BME signal. In contrast, only 1 (9.1%) patient had a decrease of subchondral cysts across the studied period, 3 (27.3%) had an increase of subchondral cysts, and 7 (63.6%) patients showed unchanged subchondral cyst formation.
Relationship Between Characteristics and Imaging and Clinical Outcomes
Among the preoperative patient and lesion characteristics, only BMI and patient age correlated with postoperative clinical outcome. BMI was significantly associated with VAS during sports (r = 0.506; P = .032) and with KOOS-QOL (r = –0.588; P = .01) and showed a tendency to correlate with KOOS–Pain (r = –0.468; P = .058), KOOS-ADL (r = –0.427; P = .099), and KOOS–Sport (r = –0.418; P = .095). Patient age was significantly associated with KOOS-ADL (r = –0.536; P = .032) and KOOS-QOL (r = –0.494; P = .037) and showed a tendency to correlate with KOOS–Pain (r = –0.448; P = .071) and KOOS–Sport (r = –0.474; P = .054).
Given the limitations of this study, we could not identify a statistically significant relationship between time to surgery, follow-up, lesion size, or lesion location with clinical outcome. Similarly, none of the patient- and lesion-specific factors or concomitant surgeries was associated with postoperative total OCAMRISS or MOCART 2.0 scores. Comparing the early-fixation (n = 13) and late-fixation (n = 5) groups did not yield significant differences in clinical or imaging outcomes; yet all patients in the late-fixation group showed surface irregularity, and 60% presented with inferior volume fill compared with 46% and 13% in the early group, respectively (P = .101 and P = .099).
When analyzing imaging subscores, we found that subchondral parameters such as BME and subchondral cyst formation were the only variables that showed significant associations with descriptive factors. In fact, while BMI was the only factor that significantly correlated with cystic changes (r = 0.523; P = .026), the patient’s age was the most consistent association between imaging outcome and characteristics (Table 3). Follow-up did not show any correlation with imaging total or subscale scores, except “integration of border zone” of the MOCART 2 (r = 0.507; P = .032).
Association Between Patient Age at Surgery and Subchondral Parameters of Imaging Outcomes a

a Boldface P values indicate statistical significance (P ≤ .05). BME, bone marrow edema; MOCART, magnetic resonance observation of cartilage repair; OCAMRISS, Osteochondral Allograft MRI Scoring System; MRI, magnetic resonance imaging.
When analyzing the relationship between imaging and clinical outcome, again, subchondral parameters were the only imaging variables that were linked to clinical outcome (Table 4). Contrarily, considering the given limitations, none of the cartilage specific variables in either the OCAMRISS or MOCART 2.0 score were associated with clinical outcome.
Association of Subchondral Parameters of Imaging Outcomes With Clinical Outcomes a

a Boldface P values indicate statistical significance (P ≤ .05). Patients showed a tendency to be more likely satisfied with the surgery if they showed less BME (P = .076), no cystic changes (P = .056), fewer subchondral changes (P = .07), and no progression of cystic lesions if existent (P = .027). ADL, Activities of Daily Living; BME, bone marrow edema; KOOS, Knee injury and Osteoarthritis Outcome Score; MOCART, magnetic resonance observation of cartilage repair; MRI, magnetic resonance imaging; OCAMRISS, Osteochondral Allograft MRI Scoring System; QOL, Quality of Life; Sport, Sport and Recreation; VAS, visual analog scale.
Discussion
The key finding of the current study was that fixation of OCFs yielded acceptable clinical and imaging outcomes at a follow-up of up to 10 years, with seemingly little influence of time from trauma to surgery. However, subchondral changes such as BME and subchondral cyst formation were found to be linked to age and clinical outcome in patients with OCFs in the knee, hence partially confirming the initial hypothesis.
Despite the still ongoing controversy regarding the optimal treatment of OCFs of the knee, multiple studies have shown that fixation of the fragment yields good clinical outcome, even in cases of purely chondral fragments. 7,11,20,27,30,37,44,42 In a recent comparative study investigating the outcome after fixation or debridement and microfracturing of OCFs of the knee, Gesslein et al 11 reported excellent clinical outcome in patients whose fragment was refixed (n = 20), with mean KOOS subscale scores between 85.5 and 95.9 after a mean follow-up of 7.8 ± 4.5 years. Similar results were published by Malecki et al 20 who studied clinical and imaging outcomes after patellar OCF fixation in adolescent patients with acute patellar dislocation. Patients presented with Kujala and Lysholm scores of 89.6 and 89.2, respectively, after a mean follow-up of 7.5 years (range, 3-10 years). Interestingly, while MRI scans revealed complete fragment integration and restoration of the articular surface in all patients, 94.1% of patients displayed an irregular subchondral bone and inhomogeneous cartilage layer. Unfortunately, the study cohort evaluated by Malecki et al was not comprehensively assessed regarding the relationship between clinical and imaging outcomes and the effect of time from trauma to surgery, yet patients with surgery after 30 days of the initial trauma were excluded from the analysis.
In 2013, a systematic review and meta-analysis was conducted to gather scientific evidence for the treatment and prognosis of OCFs in the knee. 16 Specifically, the authors aimed to determine prognostic factors that influence outcome such as age, lesion size and location, and time from trauma to surgery. However, they concluded that most studies were of poor methodological quality and could not provide the scientific evidence to provide valuable information on prognostic factors of such injuries. In the current study, age and BMI were both significantly associated with clinical and imaging outcomes. This is consistent with previous studies that reported excellent regenerative potential in pediatric and adolescent patients, as even purely chondral flaps seem to almost perfectly heal after fixation. 7,27,30,42 Interestingly, the assessment of the relationship between characteristics and clinical and imaging outcomes in the current study revealed that age was most consistently linked to imaging outcome, in particular the subchondral parameters, which in turn were the only imaging parameters associated with clinical outcome and patient satisfaction.
In a recent study by Jung et al, 13 21 patients were clinically and radiographically (quantitative 3-T MRI) evaluated after osteochondral transplantation with matrix-associated autologous chondrocyte implantation and autologous bone grafting. They reported that the subchondral imaging parameters such as BME volume and bony defect were significantly associated with pain in their cohort, emphasizing the importance of the subchondral bone. Furthermore, Merkely et al 25 advocated to distinguish between acute and chronic BME after cartilage repair procedures. While preoperative grade 4 BME predicted autologous chondrocyte implantation graft failure in patients with prior microfracture at a mean of 4.9 years before autologous chondrocyte implantation, grade 4 BME was not a predictor for failure in patients without prior cartilage procedure. Those authors reasoned that the histological properties of BME might change from subchondral remodeling in the acute phase to potentially fibrotic alterations with subchondral cyst formation in chronic BME, ultimately leading to inferior biological and mechanical properties.
In fact, the histological assessment of BME in patients with advanced osteoarthritis has shown very little actual edema but mostly bone marrow necrosis and fibrosis as well as increased bone remodeling with trabeculae abnormalities such as proliferation and thickening. 14,45 These changes were predominantly in areas with an abnormal or degenerated overlying cartilage layer. 14 Interestingly, Carrino et al 4 reported in a study with sequential MRI follow-up that subchondral cyst formation always developed within areas of preexisting BME, yet not all BME areas gave rise to cystic changes. Subsequently, future studies are warranted to assess if histological differences exist between acute and chronic BME, identifying causes that promote subchondral cyst formation and progressive chondral deterioration.
While BME was significantly associated with KOOS-QOL scores in the current study, subchondral cystic changes were the most frequently related parameter with clinical outcome. In 2010, van Dijk et al 43 elucidated the concept of painful subchondral cysts in the setting of osteochondral lesions of the talus. They reasoned that when cartilage is compressed during loading, the water outflow is forced into microfractures of the subchondral bone. This ultimately leads to high water pressure resulting in the formation of subchondral cysts. As hyaline cartilage is devoid of vessels and innervation, the pain most likely arises from the highly innervated subchondral bone that is repetitively stimulated by the high increase water flow during walking. In a meticulous analysis of the current literature, Gao et al 10 studied the influence of subchondral cyst formation on cartilage repair. While postoperative subchondral cysts and accompanying BME are frequently found across all cartilage repair techniques, their association with clinical outcome is still controversial, and further studies are warranted to establish a comprehensive conclusion. 31 Notably, while age showed associations with all subchondral parameters in the current study, it may also be theorized that the fixation with subsequent screw removal may have acted as a conduit to the subchondral bone. However, neither the number of screws nor lesion size was connected to MRI parameters. Instead, the results of the current study suggest an enhanced subchondral remodeling among the pediatric and adolescent population, again testifying to the excellent regenerative potential in this patient cohort.
Part of the initial hypothesis was that the time from trauma to surgery would affect the clinical or imaging outcome after OCF fixation. This theory is rooted in the observation that OCA storage time is significantly associated with outcome after OCA transplantation in the knee as chondrocyte viability gradually decreases over time, despite being stored in a nutrient medium. 8,24,26,29,32 Yet, the importance of surgical timing of OCF fixation has not been evaluated. In case series of 5 and 3 patients, respectively, undergoing internal reduction and fixation of chondral fragments, both Ogura et al 30 and Siparsky et al 39 reported good clinical outcome and fragment reattachment, regardless of the period between the onset of symptoms until surgery. Accordingly, both concluded that there is no time limit for fixation of chondral fragments as long as the fragment still fits the defect, as the synovial fluid may provide sufficient nutrition to maintain chondral integrity. 40 Interestingly, considering the given limitations, no statistically significant effect of surgical timing on either clinical or imaging outcome was seen in the current study, suggesting that outcome after OCF fixation may be independent of surgical delay in the treatment of OCFs on the condition that good reduction and fixation can be achieved.
Limitations
This study has some limitations. First, preoperative clinical scores were not available, as the study was retrospective in its design and preinjury Tegner scores were collected retrospectively. Second, the small sample size of only 19 patients did not allow for more detailed analyses because of lack of power. Yet, we reviewed all patients undergoing surgical screw fixation for OCFs and were able to minimize selection bias by achieving a follow-up rate of 90.5% after a follow-up of up to 10 years. Third, the general heterogeneity of the studied patient cohort with a wide range of preinjury activity levels, large variety of lesion locations, follow-up, underlying conditions, associated injuries, and injury mechanisms certainly limits the validity of the results presented herein. Yet, it represents an inherent limitation of this exclusive patient cohort with little scope to homogenize the study sample without drastically decreasing statistical power. Fourth, this study did not include a control group. However, the purpose of the current study was not to evaluate and compare clinical outcome after distinctive treatment approaches for OCFs but to comprehensively assess the effect of preoperative factors including age and surgical timing on radiographic and clinical outcomes after fixation of OCFs. Last, histological assessment was not conducted to determine chondrocyte viability of the osteochondral fragment during fixation. Undoubtably, it would be of great interest to assess cartilage quality at the time of fixation as well as to evaluate cartilage integrity at long-term follow-up beyond MRI scans to ascertain if subchondral changes disturb cartilage integrity in those patients.
Despite these limitations, this study represents the largest cohort of patients assessed via clinical outcome and detailed MRI scans after OCF fixation with the attempt to shed some light on this rare, yet significant, injury in predominantly young patients.
Conclusion
Fixation of OCFs yielded acceptable clinical and imaging outcomes at a mean follow-up of approximately 5 years with seemingly little influence of delayed surgical treatment. Yet, postoperative subchondral changes were significantly associated with clinical outcome and linked to patient age at the time of surgery.
Footnotes
Final revision submitted March 20, 2022; accepted May 12, 2022.
Acknowledgment
We would like to thank the Swiss Center for Musculoskeletal Imaging (SCMI) for providing the dedicated MRI examination in this study.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A. has received grant support from JRF Ortho and Vericel and consulting fees from ElevateBio. G.M. has received grant support and consulting fees from JRF Ortho. S.F.F. has received consulting fees from Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of the Canton of Zurich (ref No. 2020-01052).