
Abstract
Background:
Sufficient intra-articular graft ligamentization enhances the biomechanical and biological properties of the femur-graft-tibia complex to ensure knee stability after anterior cruciate ligament (ACL) reconstruction using a tendon graft. It remains unclear whether stem cell therapy promotes tendon graft ligamentization.
Purpose/Hypothesis:
The purpose of this study was to compare tendon graft ligamentization after primary ACL reconstruction with versus without stem cell therapy. It was hypothesized was that stem cell therapy would promote tendon graft ligamentization by enhancing the biomechanical and histological properties of the tendon graft after ACL reconstruction.
Study Design:
Systematic review.
Methods:
A systematic review was performed according to the guidelines outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement to identify controlled animal studies that compared tendon graft ligamentization outcomes after primary ACL reconstruction in groups with and without stem cell therapy. Biomechanical and histological outcomes were assessed.
Results:
A total of 4 studies met the eligibility criteria and were included in this review. Bone marrow–derived mesenchymal stem cells were used in 3 studies, while tendon-derived stem cells were used in 1 study. An intra-articular injection was used to deliver conditioned medium and stem cells in 2 studies, while around-graft application was used to deliver bone marrow–derived mesenchymal stem cells in 2 studies. Stem cell therapy enhanced the biomechanical and histological properties of the tendon graft after ACL reconstruction.
Conclusion:
This review revealed that stem cell therapy is a promising technique that promotes graft ligamentization by enhancing the biomechanical and histological properties of the tendon graft after ACL reconstruction in animal models. There is a need for future preclinical studies aimed at evaluating the effect of stem cells on graft ligamentization and identifying the optimal method of intra-articular stem cell delivery.
Anterior cruciate ligament (ACL) reconstruction is recommended to restore knee stability and allow patients to return to sports. 3,22 The most commonly used tissue for ACL reconstruction is a hamstring tendon graft. 17,32 Although both the hamstring tendon and ACL are composed of dense connective tissue primarily containing type I and type III collagen, proteoglycans, and cells, there are many ultrastructural differences between tendons and ligaments; in comparison with tendons, ligaments contain more type III collagen, more proteoglycans, less total collagen, a different amount of nonreducible collagen cross-links, and a different distribution of collagen fibril diameters. 8,21
The process of intra-articular tendon graft transformation into the ACL is described as ligamentization. 1,4,20 The 3 characteristic stages of tendon graft ligamentization are an early graft healing phase with central graft necrosis and hypocellularity and no detectable revascularization of graft tissue, followed by a phase of proliferation (during which the most intensive remodeling and revascularization occur), and a final ligamentization phase in which the characteristics of the graft progress toward the properties of the intact ACL. 4,11 Successful ACL reconstruction using a tendon graft requires sufficient graft ligamentization to enhance the mechanical and biological properties of the femur-graft-tibia complex to bear tension and ensure knee stability. 6
Stem cell therapy has shown promise as an adjunct treatment because of its self-renewal properties, differentiation potentials, and immunomodulatory activities. 29 It is well established that stem cells and their cytokines execute many therapeutic effects in improving tendon injury healing and biomechanical properties. 31 The process of tendon healing includes 3 phases (inflammatory, proliferative, and remodeling), which are similar to the phases of graft ligamentization. 27,35 However, only a few studies have reported the use of stem cells to promote intra-articular graft healing. Furthermore, there is a lack of systematic reviews that have comprehensively compared the biomechanical and histological outcomes of primary ACL reconstruction with versus without stem cell therapy.
The purpose of the current systematic review was to compare tendon graft ligamentization outcomes after primary ACL reconstruction with versus without stem cell therapy in animal studies. We hypothesized that stem cell therapy would promote tendon graft ligamentization by enhancing the biomechanical and histological properties of the tendon graft after ACL reconstruction.
Methods
This systematic review was performed according to the guidelines outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 10
Eligibility Criteria
All controlled animal studies comparing the outcomes of primary ACL reconstruction using a tendon graft with the application of stem cells versus the same procedure without the application of stem cells were eligible for inclusion in this review. The required outcome data were biomechanical and/or histological outcomes. Studies were excluded if they were described as review studies, cases series, technique notes, or meeting abstracts.
Literature Search and Study Selection
There were 2 independent reviewers (H.-D.W. and Z.L.) who separately searched PubMed, Embase, and the Cochrane Library to identify studies published between database inception and March 13, 2021. The title and abstract fields were searched for MeSH terms and other terms pertaining to the ACL and stem cell; the search procedures used for each database are provided in Appendix Table A1.
The search yielded 134 studies across all databases. After all titles and abstracts were reviewed, 11 duplicates were removed. Of the 123 remaining studies, 78 were excluded because they were review studies, case studies, technique notes, or meeting abstracts. After reviewing the full text, 40 studies were excluded because they did not include biomechanical or histological outcomes or because ACL reconstruction was performed using nontendon grafts. One study was excluded because it did not include stem cell therapy. The remaining studies underwent a secondary review of the full text to confirm that they met the eligibility criteria. A summary of the study selection process is presented in Figure 1.
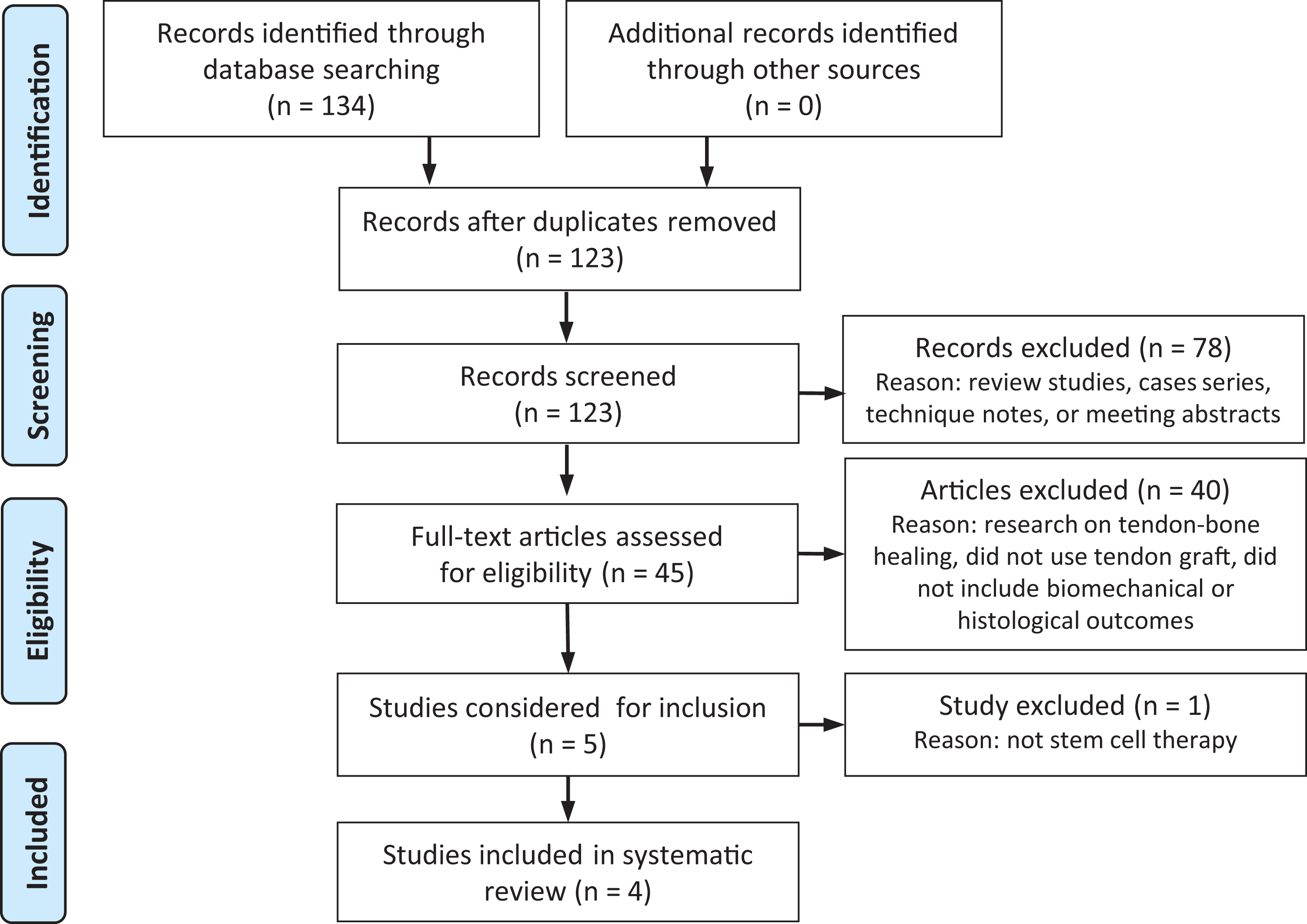
Flowchart of literature search and study selection.
Data Extraction
The same 2 authors (H.-D.W. and Z.L.) independently extracted the following data from each study: author, publication year, study design, type of study, ACL reconstruction model, stem cell type, preparation of animals/cells, intervention in the main group, and control(s). The outcomes consisted of in vivo study outcomes (including biomechanical and histological outcomes) and/or in vitro study outcomes (including the expression level of ligamentization-related genes). Duplicate data were removed. Disagreements between the reviewers were resolved via a consensus or via a discussion with the corresponding author (Y.A.) if a consensus could not be reached.
Results
Study Characteristics
The study characteristics are summarized in Table 1. Of the 4 included studies, 2 used rats, 19,26 while 2 used rabbits. 18,33 Injury models were established via ACL resection, followed by ACL reconstruction. Flexor digitorum longus tendon autografts were used in the rat models. 19,26 An Achilles tendon allograft and a hamstring tendon allograft were used in the rabbit models. 18,33
Description of Included Studies a

a ACLR, anterior cruciate ligament reconstruction; BMMNC, bone marrow mononuclear cell; BMSC, bone marrow–derived mesenchymal stem cell; CI, control injection; CM, conditioned medium; DMEM, Dulbecco’s Modified Eagle Medium; NI, no injection; PBS, phosphate-buffered saline; TDSC, tendon-derived stem cell; TGF-β1, transforming growth factor–β1; VEGF, vascular endothelial growth factor.
Bone marrow–derived mesenchymal stem cells (BMSCs) and tendon-derived stem cells (TDSCs) were used in the 4 included studies. Wei et al 33 isolated BMSCs from rabbit bone marrow and mixed gene-transduced BMSCs with fibrin sealant for application around the graft. Lui et al 19 isolated TDSCs from the rat patellar tendon and induced TDSC sheet formation by using connective tissue growth factor and ascorbic acid. The tendon graft was wrapped with a TDSC sheet before insertion in bone tunnels. 19 Sun et al 26 used human BMSCs purchased from other laboratories and obtained conditioned medium (CM) from the culture media of BMSCs. They compared BMSC-CM injections with Dulbecco’s Modified Eagle Medium injections once per week starting at 7 days postoperatively. Lu et al 18 isolated BMSCs from the rabbit iliac crest. They compared bone marrow mononuclear cell injections and BMSC injections with no cell injections.
In Vivo Study Outcomes
Biomechanical Evaluation
Biomechanical outcomes were reported in 3 studies. 19,26,33 The biomechanical outcomes are summarized in Table 2 and Figure 2. The positive effect of stem cell application after ACL reconstruction was supported by the biomechanical outcomes. Wei et al 33 reported that the transforming growth factor–β1 (TGF-β1)/vascular endothelial growth factor (VEGF-165)–transduced BMSC group had the highest ultimate failure load and stiffness among all groups. Lui et al 19 reported that the ultimate failure load at week 2 (11.2 vs 7.4 N, respectively; P = .027) and stiffness (37.0 vs 23.0 N/mm, respectively; P = .08) at week 6 were significantly higher in the TDSC group than in the control group. Sun et al 26 reported that the ultimate failure load and stiffness of the grafts in the CM group increased from 4 to 8 weeks and were significantly increased compared with the control group at both 4 weeks (ultimate failure load: 5.68 ± 1.13 vs 3.81 ± 0.76 N, respectively [P = .001]; stiffness: 9.00 ± 1.57 vs 7.09 ± 1.32 N/mm, respectively [P = .029]) and 8 weeks (ultimate failure load: 14.91 ± 1.54 vs 10.21 ± 1.12 N, respectively [P < .001]; stiffness: 12.83 ± 2.04 vs 8.51 ± 1.70 N/mm, respectively [P < .001]).
Results From Included Studies a
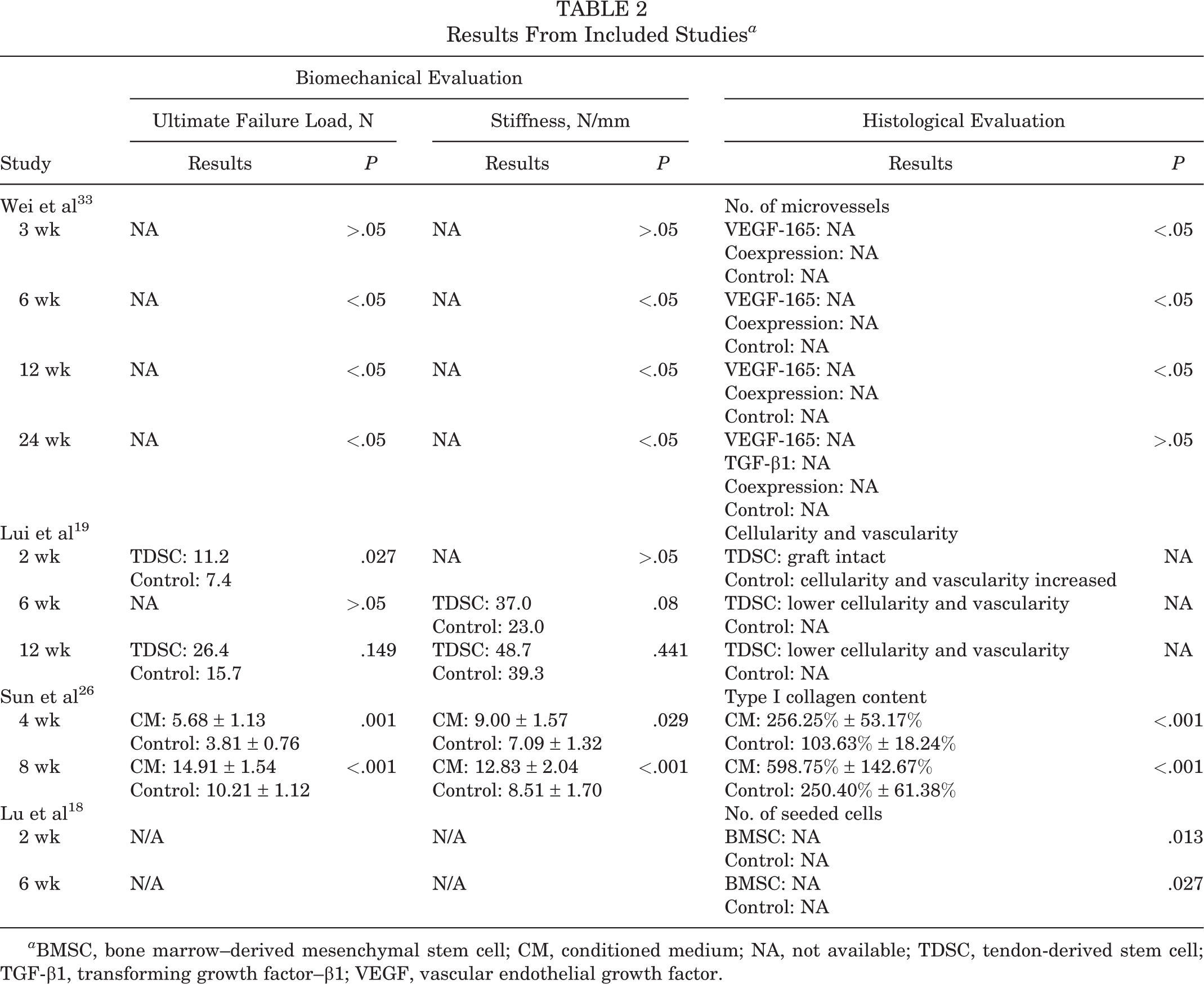
a BMSC, bone marrow–derived mesenchymal stem cell; CM, conditioned medium; NA, not available; TDSC, tendon-derived stem cell; TGF-β1, transforming growth factor–β1; VEGF, vascular endothelial growth factor.
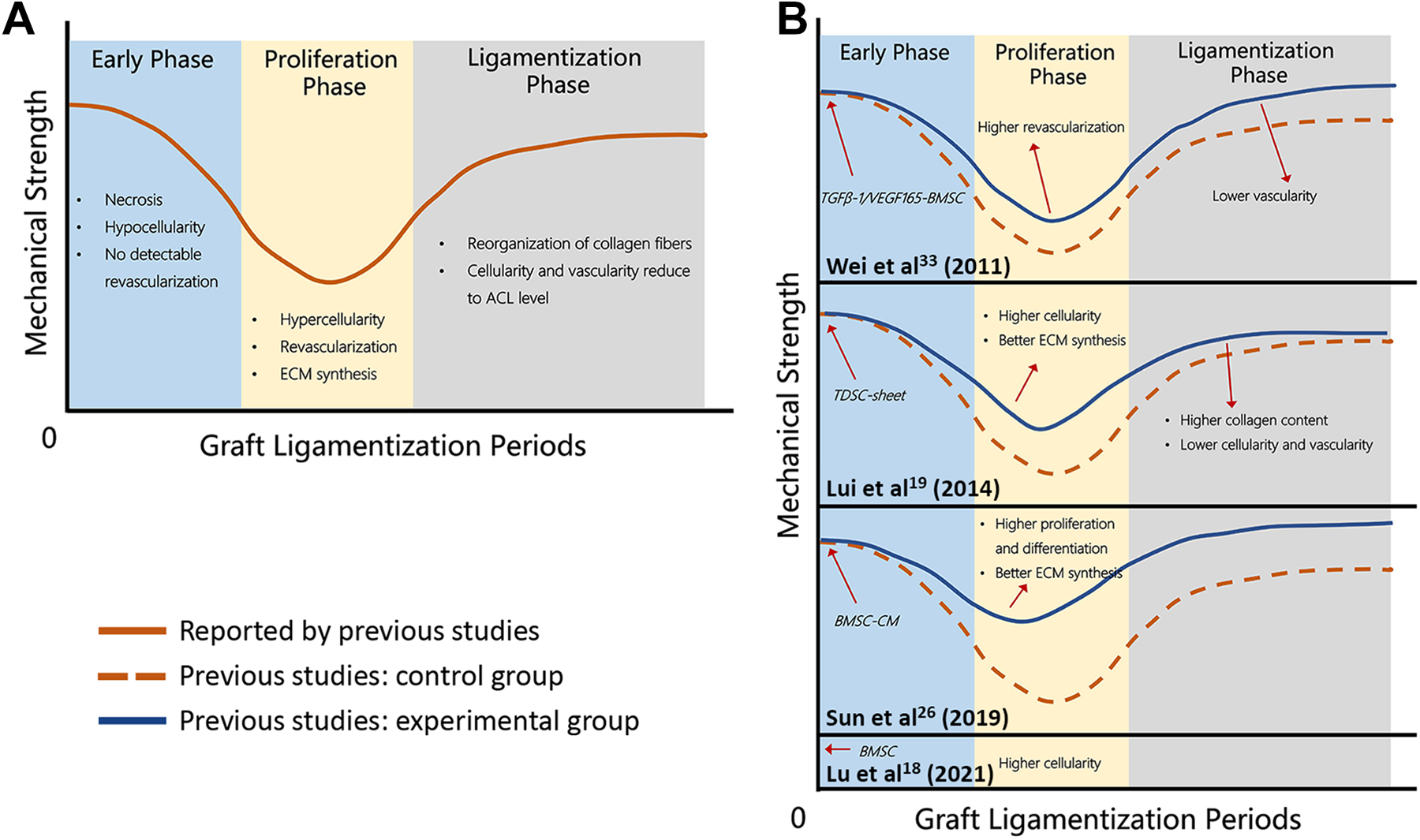
Illustration of mechanical and histological changes during graft ligamentization. The 3 characteristic stages of tendon graft ligamentization are an early graft healing phase with central graft necrosis and hypocellularity and no detectable revascularization of graft tissue, followed by a phase of proliferation (during which the most intensive remodeling and revascularization occur) and a final ligamentization phase in which the characteristics of the graft progress toward the properties of the intact anterior cruciate ligament. (A) Summary of mechanical and histological properties in the 3 phases of graft ligamentization according to previous studies. (B) Changes in mechanical and histological properties in the 3 phases of graft ligamentization under stem cell therapy in each included study. ACL, anterior cruciate ligament; BMSC, bone marrow-derived mesenchymal stem cell; CM, conditioned medium; ECM, extracellular matrix; TDSC, tendon-derived stem cell; TGFB, transforming growth factor β; VEGF165, vascular endothelial growth factor 165.
Histological Evaluation
Histological outcomes were reported in all included studies. 18,19,26,33 The histological outcomes are summarized in Table 2 and Figure 2. Lui et al 19 reported that hematoxylin and eosin–stained images of the grafts in the TDSC group showed less chondrocyte-like cells and microvessels compared with those in the control group at both 6 and 12 weeks, while Wei et al 33 found that CD33-positive–stained microvessels were predominantly at the superficial proximal bone insertion sites in the ACL grafts and that the number of microvessels in the VEGF-165 group (4.67 ± 0.21, 6.17 ± 0.17, and 5.50 ± 0.34, respectively) and coexpression group (5.17 ± 0.31, 6.33 ± 0.21, and 5.67 ± 0.33, respectively) was significantly higher than that in the control group (2.67 ± 0.21, 3.17 ± 0.17, and 3.83 ± 0.17, respectively) and TGF-β1 group (3.17 ± 0.17, 3.00 ± 0.26, and 4.17 ± 0.17, respectively) at 3, 6, and 12 weeks (P < .05 for all).
There were 2 studies that reported a greater production of collagen in the treated graft group compared with the control group from 4 to 8 weeks. 19,26 Lui et al 19 found that polarized images of the graft in the TDSC group showed higher collagen birefringence at 6 weeks. Sun et al 26 reported that relatively more areas of type I collagen birefringence were observed in the CM group (256.25% ± 53.17% and 598.75% ± 142.67%, respectively) than in the control group (103.63% ± 18.24% and 250.40% ± 61.38%, respectively) at 4 and 8 weeks. Furthermore, Lu et al 18 demonstrated that there were significantly more seeded cells in the grafts in the stem cell injection group than in the group without stem cell injections. Immunohistochemical staining showed that the CM group had an increased number of Ki-67(+) cells and a 1.85-fold higher mean expression of α-smooth muscle actin (α-SMA) per cell. 26
Discussion
The primary finding of this systematic review was that stem cells improved the biomechanics and some of the histological markers of a tendon graft after ACL reconstruction in preclinical studies. Overall, 3 in vivo studies showed that stem cell therapy improved biomechanical outcomes in most cases. This finding was also supported by an in vitro study in which CM facilitated the proliferation, differentiation, and function of α-SMA+ myofibroblasts. Additionally, collagen synthesis and secretion were promoted by the application of stem cells. 19,26,33 Although this is a systematic review of animal studies because of the lack of human studies, the findings in this study provide a feasible strategy for promoting tendon graft ligamentization after ACL reconstruction.
Both biomechanical and histological properties must be evaluated to determine whether stem cells promote graft ligamentization after ACL reconstruction. During the early graft healing phase, cells from the stump of the native ACL or bone marrow elements originating from drilling the bone tunnels migrate and infiltrate into the tendon graft. 13,14 Lu et al 18 reported that the total cell number was lower in the control group than in the bone marrow cell–injected group at 2 weeks postoperatively, suggesting that more host cells migrated and infiltrated into the tendon graft after stem cell therapy in this phase. The proliferation phase is characterized by maximum proliferation, the appearance of myofibroblasts, and extracellular matrix synthesis. 36 Sun et al 26 reported that the CM group had an increased number of Ki-67(+) cells and a 1.85-fold higher mean expression of α-SMA per cell, suggesting fibroblast-myofibroblast differentiation; the CM group also had an upregulated expression of type I collagen, a representative protein produced by myofibroblasts from the extracellular matrix. The biomechanical properties of the graft are reportedly weakest during this proliferation phase. 30 To protect the graft during this phase, previous studies attempted to use internal bracing. 5,9 However, the strength of the graft cannot be improved because of a lack of improvement in histological properties. 7 Wei et al 33 reported that the TGF-β1 group had significantly better biomechanical properties than the control group regarding the ultimate failure load and stiffness at 6 weeks postoperatively. Similarly, Lui et al 19 reported a 62% improvement in stiffness at 6 weeks in the TDSC group compared with the control group. When the graft progresses into the remodeling phase, vascularity throughout the graft decreases and returns to values of the intact ACL. 28,34 Lui et al 19 reported that the TDSC group had lower vascularity and cellularity than the control group at 12 weeks postoperatively. The biomechanical properties of the ACL-reconstructed knee joint improve substantially during the remodeling phase and reach their maximum values at approximately 1 year postoperatively. 23,34 Wei et al 33 reported that the VEGF-165 group and the coexpression group had a higher ultimate failure load and stiffness than the control group. Thus, stem cell therapy promotes tendon graft ligamentization by accelerating the change in histological properties and improving biomechanical properties (Figure 2).
Mounting evidence has shown that stem cells secrete numerous components that attract and enhance the activity and differentiation of surrounding cells. 15,24,37 These components include exosomes, growth factors, and the extracellular matrix, which are involved in regeneration of the musculoskeletal system. This effect was also found during graft ligamentization after the application of stem cells. Sun et al 26 found that CM promoted graft ligamentization by facilitating the proliferation, differentiation, and function of α-SMA+ myofibroblasts, which are essential for extracellular matrix remodeling. The delivery modes of stem cells applied to promote graft ligamentization in the included studies were intra-articular direct injections, stem cell sheet wrapping, and intra-articular CM injections. An intra-articular direct injection of stem cells was reported in 2 studies. 18,26 Although the intra-articular direct application of stem cells is commonly performed, its potential safety including tumorigenicity is still a concern. A TDSC sheet was used in 1 study. 19 The stem cell sheet eliminated the need to use synthetic scaffolds, which may have problems of biocompatibility, biodegradability, and immunogenicity. However, the implantation and fixation of a stem cell sheet on the graft are still problems for surgeons. An intra-articular injection of CM was reported in 1 study. 26 Stem cell CM contains a variety of growth factors, including VEGF, TGF-β, and insulin-like growth factor, along with exosomes. 12,37 Many of these components have already been applied to promote tendon-bone healing via the paracrine effect. 25,38 Similarly, the CM group had more orderly arrangements of collagen fibers in the graft midsubstance. 26 In comparison with intra-articular direct injections and stem cell sheet wrapping, CM injections not only decrease the risk of tumorigenicity but are also convenient. Moreover, to regulate the content of CM, we can regulate the culture condition and provide different stimulations for the stem cells.
BMSCs were used in 3 of the included studies. 18,26,33 BMSCs were obtained by drilling a hole into the femur, tibia, or iliac crest. 18,26,33 Although TDSCs were only used in 1 study, TDSCs proliferated faster and exhibited higher clonogenicity and multilineage differentiation potential compared with BMSCs. 16,19 TDSCs are obtained from residual tendon tissue during surgery, cultured, and subsequently applied. Therefore, no extra surgery is required, and no additional pain is imposed compared with bone marrow aspiration for the harvesting of BMSCs. The obtained concentration of BMSCs decreased with the increased volume of aspirated bone marrow because of the dilution of bone marrow with peripheral blood. Therefore, TDSCs may be a better prospect for stem cell therapy after ACL reconstruction compared with BMSCs.
While the present review was conducted in accordance with the PRISMA guidelines, it does have 3 limitations. First, most included studies were in vivo studies. Only 1 study used NIH-3T3 fibroblasts as a model to explore the mechanism at the gene and cell levels. 26 There is still a lack of evidence at the protein level. Second, the assessment criteria varied widely among studies. Although a biomechanical evaluation was reported in 3 studies as a primary outcome, 19,26,33 Lui et al 19 compared the percentage of unoperated data between the experimental and control groups. Sun et al 26 compared the true value between the 2 groups. However, Wei et al 33 only reported P values for comparisons between groups. Therefore, it was impossible to perform a quantitative analysis of the included studies. Third, rabbit and rat ACL reconstruction models were used in the included studies. There is a difference between these small animals and humans in terms of the stability and mechanical properties of ACL grafts, 2 but the biomechanical testing in the included studies were performed by tensile instead of knee stability. Small animal models were still the most commonly used for preclinical research. Further research is needed to investigate how stem cells play a role in promoting graft ligamentization after ACL reconstruction.
Conclusion
The current systematic review suggests that stem cell therapy is a promising option for the promotion of intra-articular tendon graft ligamentization by enhancing the biomechanical and histological properties of the tendon graft after ACL reconstruction. Future preclinical studies aimed at evaluating the effect of stem cells on graft ligamentization and identifying the optimal method of intra-articular delivery are still required.
Footnotes
Final revision submitted December 27, 2021; accepted February 17, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Details and Results of Database Searches

| No. | Details | Results |
|---|---|---|
| PubMed Search | ||
| #1 | “anterior cruciate ligament”[MeSH Terms] OR “cruciate ligament anterior”[Title/Abstract] OR “anterior cruciate ligaments”[Title/Abstract] OR “cruciate ligaments anterior”[Title/Abstract] OR “ligament anterior cruciate”[Title/Abstract] OR “ligaments anterior cruciate”[Title/Abstract] OR “anterior cranial cruciate ligament”[Title/Abstract] OR “cranial cruciate ligament”[Title/Abstract] OR “cranial cruciate ligaments”[Title/Abstract] OR ((“Cruciate”[All Fields] OR “cruciates”[All Fields]) AND “ligament cranial”[Title/Abstract]) OR ((“Cruciate”[All Fields] OR “cruciates”[All Fields]) AND “ligaments cranial”[Title/Abstract]) OR ((“ligament s”[All Fields] OR “Ligaments”[MeSH Terms] OR “Ligaments”[All Fields] OR “Ligament”[All Fields]) AND “cranial cruciate”[Title/Abstract]) OR “ligaments cranial cruciate”[Title/Abstract] | 11,659 |
| #2 | “wound healing”[MeSH Terms] OR “Healing”[Title/Abstract] OR “Ligamentization”[Title/Abstract] OR “Remodeling”[Title/Abstract] | 360,415 |
| #3 | “stem cells”[MeSH Terms] OR “cell stem”[Title/Abstract] OR “cells stem”[Title/Abstract] OR “stem cell”[Title/Abstract] OR “progenitor cells”[Title/Abstract] OR “cell progenitor”[Title/Abstract] OR “cells progenitor”[Title/Abstract] OR “progenitor cell”[Title/Abstract] OR “mother cells”[Title/Abstract] OR “cell mother”[Title/Abstract] OR “cells mother”[Title/Abstract] OR “mother cell”[Title/Abstract] OR “colony forming unit”[Title/Abstract] OR “colony forming unit”[Title/Abstract] OR “colony forming units”[Title/Abstract] OR “colony forming units”[Title/Abstract] | 364,818 |
| #4 | (“anterior cruciate ligament”[MeSH Terms] OR “cruciate ligament anterior”[Title/Abstract] OR “anterior cruciate ligaments”[Title/Abstract] OR “cruciate ligaments anterior”[Title/Abstract] OR “ligament anterior cruciate”[Title/Abstract] OR “ligaments anterior cruciate”[Title/Abstract] OR “anterior cranial cruciate ligament”[Title/Abstract] OR “cranial cruciate ligament”[Title/Abstract] OR “cranial cruciate ligaments”[Title/Abstract] OR ((“Cruciate”[All Fields] OR “cruciates”[All Fields]) AND “ligament cranial”[Title/Abstract]) OR ((“Cruciate”[All Fields] OR “cruciates”[All Fields]) AND “ligaments cranial”[Title/Abstract]) OR ((“ligament s”[All Fields] OR “Ligaments”[MeSH Terms] OR “Ligaments”[All Fields] OR “Ligament”[All Fields]) AND “cranial cruciate”[Title/Abstract]) OR “ligaments cranial cruciate”[Title/Abstract]) AND (“wound healing”[MeSH Terms] OR “Healing”[Title/Abstract] OR “Ligamentization”[Title/Abstract] OR “Remodeling”[Title/Abstract]) AND (“stem cells”[MeSH Terms] OR “cell stem”[Title/Abstract] OR “cells stem”[Title/Abstract] OR “stem cell”[Title/Abstract] OR “progenitor cells”[Title/Abstract] OR “cell progenitor”[Title/Abstract] OR “cells progenitor”[Title/Abstract] OR “progenitor cell”[Title/Abstract] OR “mother cells”[Title/Abstract] OR “cell mother”[Title/Abstract] OR “cells mother”[Title/Abstract] OR “mother cell”[Title/Abstract] OR “colony forming unit”[Title/Abstract] OR “colony forming unit”[Title/Abstract] OR “colony forming units”[Title/Abstract] OR “colony forming units”[Title/Abstract]) | 43 |
| Cochrane Library Search | ||
| #1 | MeSH descriptor: [Stem Cells] explode all trees | 794 |
| #2 | (Cell, Stem): ti, ab, kw OR (Cells, Stem): ti, ab, kw OR (Stem Cell): ti, ab, kw OR (Progenitor Cells): ti, ab, kw OR (Cell, Progenitor): ti, ab, kw (Word variations have been searched) | 14,057 |
| #3 | (Cells, Progenitor): ti, ab, kw OR (Progenitor Cell): ti, ab, kw OR (Mother Cells): ti, ab, kw OR (Cell, Mother): ti, ab, kw OR (Cells, Mother): ti, ab, kw (Word variations have been searched) | 2934 |
| #4 | (Mother Cell): ti, ab, kw OR (Colony-Forming Unit): ti, ab, kw OR (Colony Forming Unit): ti, ab, kw OR (Colony-Forming Units): ti, ab, kw OR (Colony Forming Units): ti, ab, kw (Word variations have been searched) | 3177 |
| #5 | #1 or #2 or #3 or #4 | 17,068 |
| #6 | MeSH descriptor: [Anterior Cruciate Ligament] explode all trees | 659 |
| #7 | (Cruciate Ligament, Anterior): ti, ab, kw OR (Anterior Cruciate Ligaments): ti, ab, kw OR (Cruciate Ligaments, Anterior): ti, ab, kw OR (Ligament, Anterior Cruciate): ti, ab, kw OR (Ligaments, Anterior Cruciate): ti, ab, kw (Word variations have been searched) | 2699 |
| #8 | (Anterior Cranial Cruciate Ligament): ti, ab, kw OR (Cranial Cruciate Ligament): ti, ab, kw OR (Cranial Cruciate Ligaments): ti, ab, kw OR (Cruciate Ligament, Cranial): ti, ab, kw OR (Cruciate Ligaments, Cranial): ti, ab, kw (Word variations have been searched) | 7 |
| #9 | (Ligament, Cranial Cruciate): ti, ab, kw OR (Ligaments, Cranial Cruciate): ti, ab, kw (Word variations have been searched) | 7 |
| #10 | #6 or #7 or #8 or #9 | 2706 |
| #11 | MeSH descriptor: [] explode all trees | 0 |
| #12 | MeSH descriptor: [] explode all trees | 0 |
| #13 | (Healing): ti, ab, kw OR (Ligamentization): ti, ab, kw OR (Remodeling): ti, ab, kw (Word variations have been searched) | 37,765 |
| #14 | #11 or #12 or #13 | 37,765 |
| #15 | #5 and #10 and #14 | 15 |
| Embase Search | ||
| #1 | “stem cell”/exp | 395,432 |
| #2 | “cell, stem”: ab, ti OR “cells, stem”: ab, ti OR “stem cell”: ab, ti OR “progenitor cells”: ab, ti OR “cell, progenitor”: ab, ti OR “cells, progenitor”: ab, ti OR “progenitor cell”: ab, ti OR “mother cells”: ab, ti OR “cell, mother”: ab, ti OR “cells, mother”: ab, ti OR “mother cell”: ab, ti OR “colony-forming unit”: ab, ti OR “colony forming unit”: ab, ti OR “colony-forming units”: ab, ti OR “colony forming units”: ab, ti | 346,929 |
| #3 | #1 or #2 | 543,576 |
| #4 | “anterior cruciate ligament”/exp | 12,175 |
| #5 | “cruciate ligament, anterior”: ab, ti OR “anterior cruciate ligaments”: ab, ti OR “cruciate ligaments, anterior”: ab, ti OR “ligament, anterior cruciate”: ab, ti OR “ligaments, anterior cruciate”: ab, ti OR “anterior cranial cruciate ligament”: ab, ti OR “cranial cruciate ligament”: ab, ti OR “cranial cruciate ligaments”: ab, ti OR “cruciate ligament, cranial”: ab, ti OR “cruciate ligaments, cranial”: ab, ti OR “ligament, cranial cruciate”: ab, ti OR “ligaments, cranial cruciate”: ab, ti | 1449 |
| #6 | #4 or #5 | 12,936 |
| #7 | “healing”/exp | 265,073 |
| #8 | healing: ab, ti OR ligamentization: ab, ti OR remodeling: ab, ti | 390,588 |
| #9 | #7 or #8 | 521,824 |
| #10 | #3 and #6 and #9 | 76 |