
Abstract
Background:
In anatomic anterior cruciate ligament (ACL) reconstruction, graft placement through the anteromedial (AM) portal technique requires more horizontal drilling of the femoral tunnel as compared with the transtibial (TT) technique, which may lead to a shorter femoral tunnel and affect graft-to-bone healing. The effect of coronal and sagittal femoral tunnel obliquity angle on femoral tunnel length has not been investigated.
Purpose:
To compare the length of the femoral tunnels created with the TT technique versus the AM portal technique at different coronal and sagittal obliquity angles using the native femoral ACL center as the starting point of the femoral tunnel. The authors also assessed sex-based differences in tunnel lengths.
Study Design:
Descriptive laboratory study.
Methods:
Magnetic resonance imaging scans of 95 knees with an ACL rupture (55 men, 40 women; mean age, 26 years [range, 16-45 years]) were used to create 3-dimensional models of the femur. The femoral tunnel was simulated on each model using the TT and AM portal techniques; for the latter, several coronal and sagittal obliquity angles were simulated (coronal, 30°, 45°, and 60°; sagittal, 45° and 60°), representing the 10:00, 10:30, and 11:00 clockface positions for the right knee. The length of the femoral tunnel was compared between the techniques and between male and female patients.
Results:
The mean ± SD femoral tunnel length with the TT technique was 40.0 ± 6.8 mm. A significantly shorter tunnel was created with the AM portal technique at 30° coronal/45° sagittal (35.5 ± 3.8 mm), whereas a longer tunnel was created at 60° coronal/60° sagittal (53.3 ± 5.3 mm; P < .05 for both). The femoral tunnel created with the AM portal technique at 45° coronal/45° sagittal (40.7 ± 4.8 mm) created a similar tunnel length as the TT technique. For all techniques, the femoral tunnel was significantly shorter in female patients than male patients.
Conclusion:
The coronal and sagittal obliquity angles of the femoral tunnel in ACL reconstruction can significantly affect its length. The femoral tunnel created with the AM portal technique at 45° coronal/45° sagittal was similar to that created with the TT technique.
Clinical Relevance:
Surgeons should be aware of the femoral tunnel shortening with lower coronal obliquity angles, especially in female patients.
Keywords
In single-bundle anterior cruciate ligament (ACL) reconstruction, the femoral tunnel has historically been drilled through the tibial tunnel (transtibial [TT] technique). 29 In the past few decades, the anteromedial (AM) portal technique has gained popularity in anatomic ACL reconstructions, as it allows for femoral tunnel positioning based solely on anatomic considerations, independent from the tibial tunnel trajectory. 17,20,31 This technique leads to increased rotational stability as well as tension patterns similar to the native ACL. 28,31 However, anatomic graft placement through the AM portal requires more horizontal drilling of the femoral tunnel, which may result in excessively short femoral tunnels 7 and, as a consequence, limit the amount of graft within the femoral tunnel and affect graft-to-bone healing. 8,26,35 In previous reports, Qi et al 26 and Greis et al 8 investigated the relationship between femoral tunnel length and graft healing and demonstrated that there was an improvement in graft pullout strength with increasing tunnel length and that an intratunnel graft <15 mm should be avoided.
Several studies have reported significantly shorter femoral tunnels in the AM portal technique versus the TT technique. 2,11,13,22,34 Previous studies 7,11 showed that several independent variables contributed to the tunnel length in ACL reconstruction, such as the starting point, 7,11 the sagittal obliquity for the sagittal axis, 2 the coronal obliquity for the coronal axis, 2 and each patient’s morphometric characteristics. 27 A strong correlation was noted between femoral tunnel length and the femoral tunnel starting point, with a more anterior 11 and vertical (in the coronal plane) 7 starting point being associated with long tunnels. Current data suggest that anatomic ACL reconstructions, in which the graft is placed within the native ACL footprint, might result in better functional outcomes and knee stability. 15,21 Furthermore, it is possible to have relatively good isometricity while still having the femoral tunnel within the anatomic ACL femoral footprint. 33 Therefore, most surgeons aim to position the starting femoral tunnel starting point within the femoral ACL footprint. 10 In addition, Bedi et al 2 found that increasing degrees of knee flexion could significantly affect its length.
Under these conditions, including the starting point and the angle of knee flexion, the effect of coronal and sagittal femoral tunnel obliquity angle on femoral tunnel length during anatomic ACL reconstruction has never been investigated. The aim of the present study was to investigate any differences in the length of the femoral tunnels created with the TT technique versus the AM portal technique at several coronal and sagittal obliquity angles, using the native femoral ACL center as the starting point. We also compared tunnel lengths between male and female patients.
Methods
Study Design and Patient Selection
Institutional review board approval was received for the study protocol. Inclusion criteria were age <45 years, no history of trauma or surgery on the injured knee, and magnetic resonance imaging (MRI) scans performed within 1 month of injury (to reduce the risk of not identifying the ACL footprint attributed to ACL stump deterioration). Exclusion criterion was poor-quality MRI scans that did not allow for the identification of the femoral footprint or reconstruction of the 3-dimensional (3D) models. The MRI scans of 95 ACL-ruptured knees (55 men, 40 women; 52 right, 43 left) were included in the study with a mean age of 26 years (range, 16-45 years).
MRI-Based 3D Models
All patients were scanned using a 3.0-T MR Scanner (Achieva; Philips Healthcare). The 3D surface models of the knee, including the femur and tibia, were reconstructed using commercial software (AMIRA, FEI SVG; Thermo Fisher Scientific). The accuracy of the described technique is expected to be <1 mm based on the study of Han et al, 9 who compared the open cadaveric measurements with 1.5-T 3D MRI measurements and demonstrated that the paired differences in femoral length and width between the methods were 1 and 2 mm, respectively. Finally, the surface models were imported to a self-developed MATLAB script for subsequent analyses. The anatomic coordinate system of the distal femur was reconstructed according to a previously published method based on the cylindrical axis, 5 as several studies showed that the cylindrical axis is coincident with the flexion-extension axis of the knee. 6,12 The femoral ACL footprint surface area was digitized on each model, and its centroid was defined as the femoral ACL center using a previously published method. 6
Creation of the TT and AM Portal Tunnels
For the TT technique, the knee was flexed to 90° around the flexion-extension axis of the knee, respecting the femoral rollback according to published literature. 18 An 8-mm cylinder was placed on the tibial tuberosity. The starting point was medial and proximal to the tibial tuberosity to a tibial angle of 20° in the coronal plane and 50° in the sagittal plane by referring to the flexion-extension axis of the knee 1 (Figure 1). The length of the tibial and femoral tunnels was measured as the distance from the proximal to distal cortical bone of the tibia and femur at the center of the cylinder, respectively.

The right knee flexed at 90° demonstrates the femoral tunnel created by the transtibial technique starting medial and proximal to the tibial tuberosity. The tibial angle is (A) 20° in the coronal plane and (B) 50° in the sagittal plane. The femoral anterior cruciate ligament surface area and center are indicated by a green dot.
For the AM portal technique, the knee was flexed to 110°, 1 and an 8-mm cylinder was placed on the femoral ACL center at coronal obliquity angles of 30°, 45°, and 60° (which represented the 10:00, 10:30, and 11:00 clockface positions in the right knees and the 2:00, 1:30, and 1:00 clockface positions in the left knees 19 ) and sagittal obliquity angles of 45° and 60° (Figure 2). The length of the femoral tunnel was measured as the distance from the medial-distal to lateral-proximal cortical bone of the lateral femoral condyle at the center of the cylinder at all combinations of angles.
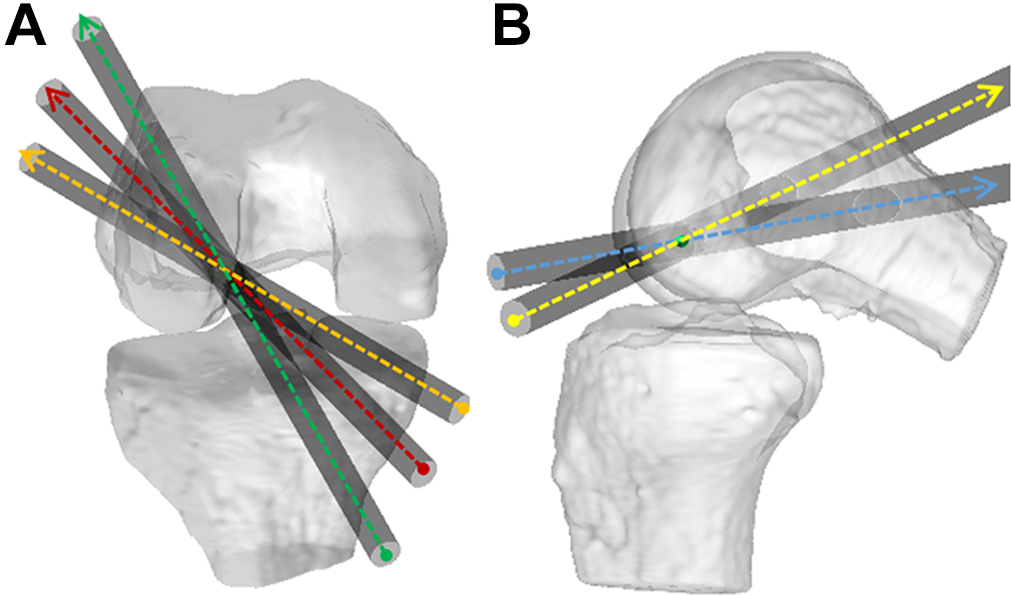
The right knee flexed at 110° demonstrates the femoral tunnel created by the anteromedial portal technique starting at the native femoral anterior cruciate ligament center (green dot). The coronal obliquity angles are (A) 30° (orange), 45° (red), and 60° (green), and the sagittal obliquity angles are (B) 45° (blue) and 60° (yellow).
Repeatability Analysis
Manual digitization was involved for the femoral ACL center and tibial starting point. Inter- and intraobserver reliabilities of these measurements were evaluated for all the models using the single-measure intraclass correlation coefficient with a 2-way random effects model for absolute agreement. For interobserver reliability, 2 blinded observers (D.D. and R.C.) made the measurements independently. For intrarater reliability, 2 sets of measurements were performed by the same observer (D.D.) within 4 weeks.
Statistical Analysis
Continuous data were reported as means, standard deviations, and ranges while categorical data were reported as frequencies and percentages. One-way analysis of variance followed by Bonferroni post hoc analysis was used to investigate whether a significant difference in length was present between the femoral tunnels created with the TT technique and the AM portal technique at different angles. For non-normally distributed data, nonparametric analysis was used. A t test was used to compare the differences between techniques in male and female patients. The percentage of the femoral tunnels <25 mm, defined as the critical length of the femoral tunnel, 2 was also noted for the various techniques. All the statistical analyses were performed using SPSS Version 21 software (IBM). Statistical significance was set at P < .05.
Results
Intra- and Interobserver Reliability
The intra- and interobserver intraclass correlation coefficients were, respectively, 0.97 and 0.95 for the femoral ACL center and 0.94 and 0.91 for the tibial starting point, indicating excellent reliability overall.
TT and AM Portal Tunnel Lengths
The mean ± SD femoral and tibial tunnel lengths for the TT technique were 40.0 ± 6.8 and 45.1 ± 4.7 mm, respectively. For the AM portal technique, a significantly shorter femoral tunnel was created at 30° coronal/45° sagittal (35.5 ± 3.8 mm, P < .05), whereas a significantly longer tunnel was created at 60° coronal/60° sagittal (53.3 ± 5.3 mm, P < .05) (Figure 3). Significant differences were found in the femoral tunnel length created with the TT technique versus the AM portal technique at 60° coronal/60° sagittal (mean difference, 13.3 mm; P < .05), 60° coronal/45° sagittal (mean difference, 9.0 mm; P < .05), 45° coronal/60° sagittal (mean difference, 4.0 mm; P < .05), 30° coronal/60° sagittal (mean difference, –3.6 mm; P < .05), and 30° coronal/45° sagittal (mean difference, –4.6 mm; P < .05). The femoral tunnel created with the AM portal at 45° coronal/45° sagittal was similar to that created with the TT technique (mean difference, 0.7 mm; P > .05).
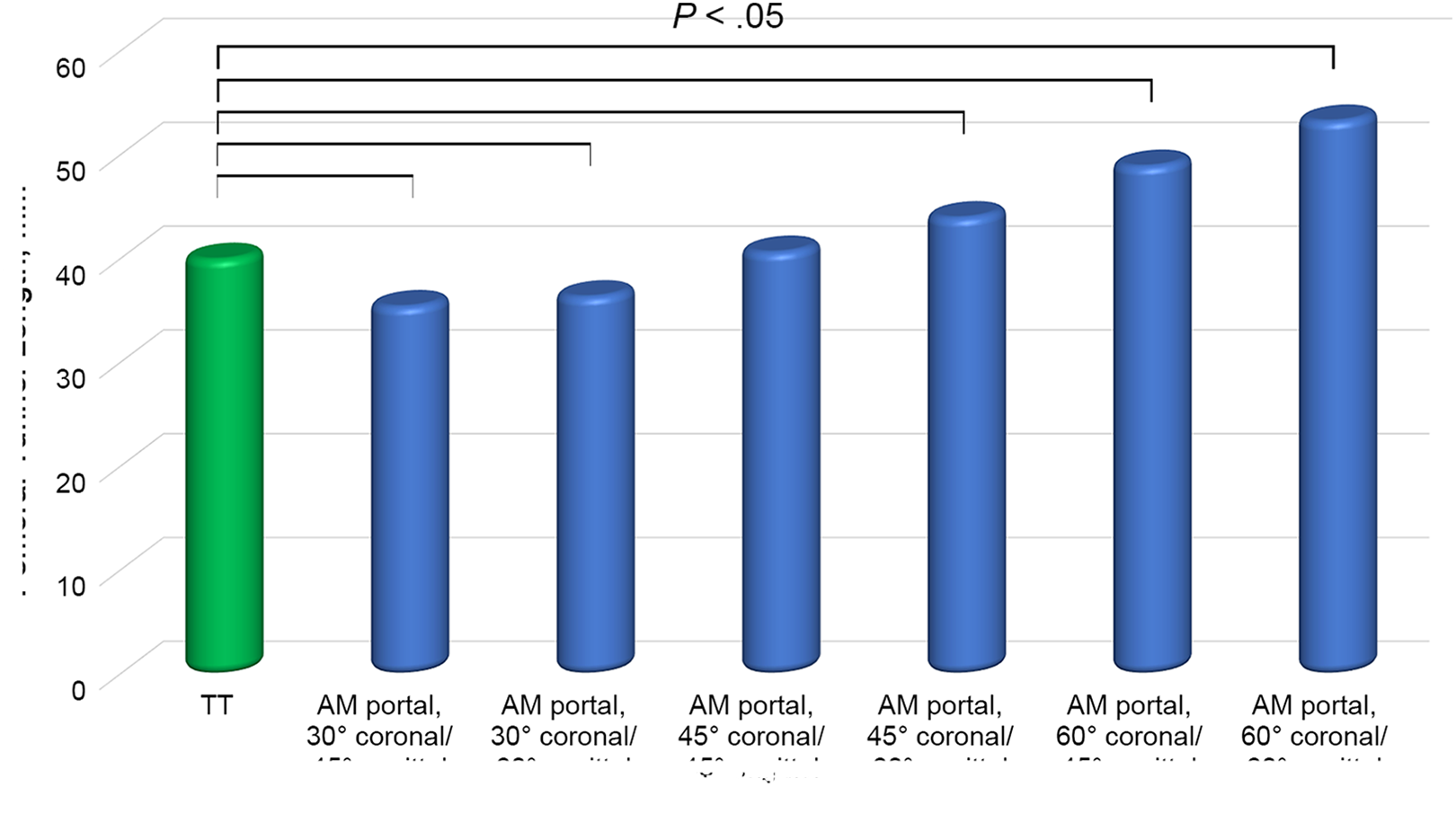
Mean femoral tunnel lengths created using the transtibial (TT) and anteromedial (AM) portal techniques.
The mean femoral tunnel length was significantly shorter in female patients than male patients in both techniques and at all obliquity angles (P < .05 for all) (Table 1). One female patient (1%) had a femoral tunnel length shorter than the 25-mm critical cutoff value with the TT technique, and 1 female patient (1%) had a femoral length equal to the critical cutoff value of 25 mm with the AM portal technique at 30° coronal/45° sagittal.
Sex-Based Comparison of Femoral Tunnel Lengths Created Using the Transtibial and Anteromedial Portal Techniques a

a Data are provided as mean ± SD (range). Female patients had significantly shorter femoral tunnel lengths than male patients for all techniques (P < .05 for each row).
Discussion
The most important finding of the present study was that the coronal and sagittal obliquity angles of the femoral tunnel could significantly affect its length. Femoral tunnels with coronal and sagittal obliquity angles ≥45° demonstrated similar or even longer lengths as compared with the TT technique. No patients showed femoral tunnel lengths shorter than the critical cutoff value of 25 mm with the AM portal technique at coronal and sagittal obliquity angles >45°. Female patients had a significantly shorter femoral canals than male patients.
Several studies have reported that the AM portal technique could result in significantly shorter femoral tunnels as compared with the TT approach. Jennings et al, 14 in a laboratory study of 36 cadaveric knees, found that the AM portal technique resulted in significantly shorter femoral tunnels than the TT technique (31.6 ± 1.6 vs 42.6 ± 2.8 mm, P < .001). However, the coronal and sagittal obliquity angles of the femoral tunnel in the AM portal technique were not indicated. Similarly, in a retrospective comparative study, Tampere et al 32 reported significantly shorter femoral tunnels with the AM portal technique than the TT technique (37.4 vs 51.9 mm, P < .001). In a retrospective comparative study of 100 patients who underwent single-bundle reconstruction with the TT technique (n = 36), AM portal technique (n = 32), and outside-in technique (n = 32), Osti et al 25 found significantly shorter femoral canals created by the AM portal technique in 30° coronal obliquity as compared with the TT technique (33.4 ± 6.7 vs 42.3 ± 8.5 mm, P < .01). Ilahi et al, 13 in a prospective study of 115 consecutive patients (35 with TT technique and 80 with AM portal technique), reported a significant difference in mean intraoperative femoral tunnel length between the TT and AM portal techniques in male patients (41.7 mm [range, 34-55 mm] vs 36.7 mm [range, 35-42 mm], P < .0001) as well as between the TT and AM portal techniques in female patients (36.8 mm [range, 30-48 mm] vs 33.5 mm [range, 28-40 mm], P < .05). Moon et al 24 concluded that a lower coronal obliquity angle of the femoral tunnel resulted in shorter femoral tunnel lengths and that a smaller coronal angle should be avoided.
In accordance with the literature, we found that the AM portal technique would have resulted in a significantly shorter femoral tunnel in 30° coronal obliquity angles as compared with the TT technique in the same patient. For all drilling techniques, female patients demonstrated significantly shorter femoral canals versus male patients. Femoral tunnels with coronal and sagittal obliquity angles ≥45° had similar or even longer lengths than the TT technique. These findings are supported by Chang et al, 3 who reported that a lower coronal obliquity angle of the femoral tunnel resulted in shorter femoral tunnel lengths, with a mean length of 51.1 ± 6.3 mm at 11:30 o’clock (75° coronal obliquity), 40.0 ± 5.4 mm at 10:30 o’clock (45° coronal obliquity), and 34.2 ± 3.9 mm at 9:30 o’clock (15° coronal obliquity). Although only 1 patient (1%) had a femoral tunnel length equal to the critical cutoff value of 25 mm in the AM portal technique, surgeons should be aware of shorter femoral tunnels with lower coronal obliquity angles, especially in female patients.
Several studies have focused on the influence of graft length within the bone tunnel on tendon-bone healing. 8,26,30 Rodeo et al 30 described that the increase of collagen fibers in the graft and the bone wall was correlated with an increase in the pullout strength of the graft within the bone tunnel and that the pullout strength of the tendon from the bone tunnel increased with the increase of the ligament length. Qi et al 26 found an improvement in the pullout strength with the increase of graft length within the bone tunnel. Greis et al 8 demonstrated a significant improvement in pullout strength of the tendon with the increase of graft length in an extra-articular tendon-bone healing model. The pullout strength of the tendon with 10 mm was significantly lower than that with 20 mm.
Our study showed that the coronal and sagittal obliquity angles of the femoral tunnel could significantly affect its length. Furthermore, Tampere et al 32 showed that mean reaction forces in the graft using the AM technique were nonsignificant and higher than that of the TT technique and that mean reaction moments in the graft using the TT technique were nonsignificant and higher than that of AM technique. Cheng et al 4 showed that the femoral tunnel drilling angle could affect the stress and strain distribution on the femoral tunnel, tibial tunnel, and graft. Therefore, the optimal coronal and sagittal femoral tunnel obliquity angle to achieve longer femoral tunnels in anatomic ACL reconstructions may be beneficial for graft-to-bone healing.
Female patients demonstrated significantly shorter femoral tunnels than male patients with lower coronal obliquity angles. A coronal and sagittal obliquity angle of 45° might be advisable to achieve femoral tunnel lengths while maintaining the advantages of a horizontal femoral tunnel.
Limitations
The present study should be interpreted in light of its potential limitations, mostly inherent to the MRI identification of the femoral ACL footprint, which might be difficult as a result of the tissue disruption and rapid deterioration of the ACL stump after the ACL rupture. However, the present study included only those patients with high-quality MRI scans obtained within 1 month of injury. The femoral ACL footprint was visible in all the patients included. Furthermore, all the patients in the present study were White. Therefore, the results of the present study might not reflect the femoral tunnel length of the non-White population, as ethno-specific anatomic variations of the knee have been reported. 16 Third, the knees in the present study were ACL-deficient, and the effect of this was unclear. Fourth, the modeling of the AM portal drilling did not take portal placement into account. Fifth, the present study is based on computer simulations from MRI scans acquired from actual patients, with potential simulation errors. Although Montreuil et al 23 described femoral tunnel placement in ACL reconstruction through the use of a novel 3D reference with biplanar stereoradiographic imaging, the results showed a poor correlation for tunnel orientation. The advantage of our technique is that it allows for intrasubject comparisons of various techniques, which enables us to estimate the effect of the drilling angle on the femoral tunnel length.
Conclusion
Study results indicated that the coronal and sagittal obliquity angles of the femoral tunnel in ACL reconstruction can significantly affect its length. The femoral tunnel created with the AM portal at 45° coronal/45° sagittal resulted in a similar tunnel length as the TT technique. Female patients demonstrated significantly shorter femoral canals when compared with male patients. Surgeons should be aware of femoral tunnel shortening with lower coronal obliquity angles, especially in female patients.
Footnotes
Final revision submitted February 11, 2022; accepted February 25, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was sponsored by the National Natural Science Foundation of China (31972924), the National Key R&D Program of China (2019YFC0120600), and the Interdisciplinary Program of Shanghai Jiao Tong University (ZH2018QNA06, YG2021QN68). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of northwest and central Switzerland (2018-01410).