
Abstract
Purpose:
Recently, tunnel placements in anatomic positions have been emphasized for successful restoration of knee function after anterior cruciate ligament (ACL) reconstruction. The anteromedial portal technique is considered to be more favorable than the transtibial technique for anatomic femoral tunnel placements; however, it has some technical disadvantages. To minimize these disadvantages, the authors developed the curved dilator system (CDS). The purpose of this study was to evaluate the femoral tunnel position, length, and intraoperative complications with CDS.
Methods:
Sixty-two consecutive patients who underwent ACL reconstruction with CDS were subjects of this study. The femoral tunnel was created using a 4.5 mm-diameter curved guide trocar and was widened in a step-by-step manner, increasing by 1 mm dilator diameter to match the graft with the knee flexed to slightly over 90°. Femoral tunnel positions were evaluated by the quadrant method from postoperative computed tomographic images. Femoral tunnel length was measured using the curved depth gauge during surgery. Complications such as posterior wall blowout and cartilage damage were checked intraoperatively. Peroneal nerve injury was observed during the hospital stay.
Results:
Femoral tunnel position was 32.7% ± 5.4% and 39.1% ± 5.9% in the superior-inferior and anterior-posterior positions, respectively. Femoral tunnel length was 39.2 ± 4.1 mm. Damage to medial femoral condyle cartilage, posterior wall blowout, and peroneal nerve injury did not occur in any case.
Conclusion:
ACL reconstruction with CDS resulted in anatomic positioning of the femoral tunnel and sufficient femoral tunnel length without intraoperative complications.
Keywords
Introduction
Anatomic positioning of the tunnels yields better functional outcome and knee stability than isometric positioning in anterior cruciate ligament (ACL) reconstruction. 1 –3 The transtibial technique is traditionally used to create the femoral tunnel; however, there are concerns regarding its feasibility to locate the tunnel anatomically. 4 –7 To resolve this, there have been several changes, and the anteromedial (AM) portal technique is one such change. Because the femoral tunnel position can be located independently with the AM portal technique, unlike with the transtibial technique, the probability of locating the femoral tunnel anatomically is higher. Several reports support that tunnels are created in more anatomic positions with the AM portal technique than with the transtibial technique. 8,9 However, the AM portal technique has some disadvantages. Deep knee flexion is required while passing the reamer to the lateral femoral condyle to create a femoral tunnel, which limits arthroscopic view. Even with the deep knee flexion, the risk of medial femoral condyle cartilage damage when inserting the reamer is high. Furthermore, because the trajectory for the tunnel is oblique, the outlet of the femoral tunnel is created rather inferiorly and posteriorly, which leads to a shorter tunnel length and possibility of peroneal nerve injury. 10 –12
To overcome these surgical difficulties and minimize complications, the authors developed the curved dilator system (CDS; Figure 1; Kim’s Meditech Co., Ltd, Seoul, Korea). The purpose of this study was to evaluate the femoral tunnel created with CDS and report the intraoperative complications with this new system. The authors hypothesized that creating femoral tunnel at anatomic position, with sufficient length and without intraoperative complications, is possible with the CDS.
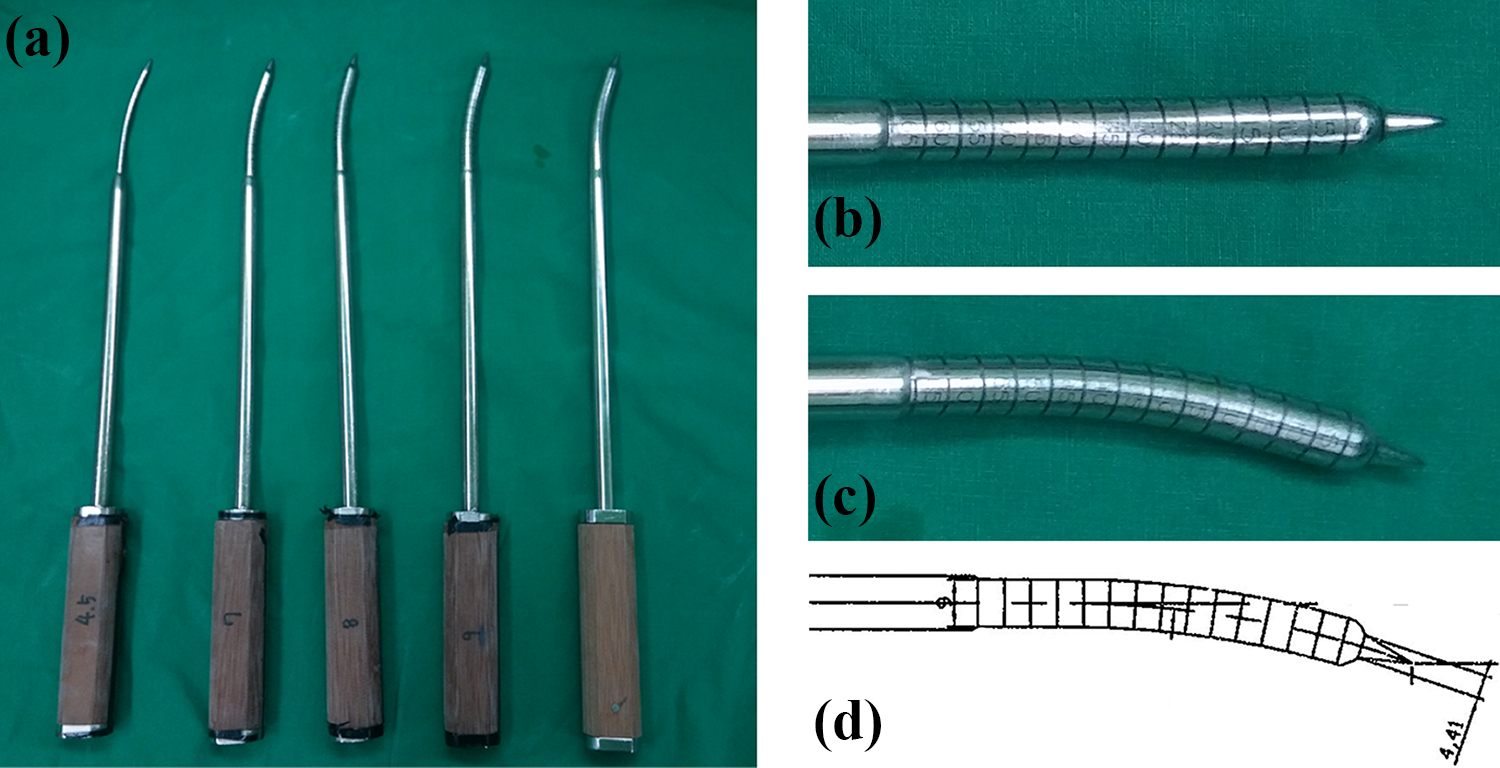
Curved dilator system. (a) Starting from the left, a 4.5 mm-diameter curved guide trocar, a 7 mm-diameter curved dilator, an 8 mm-diameter curved dilator, a 9 mm-diameter dilator, and a 10 mm-diameter dilator. The curved part is bent at 15° with respect to the shaft axis. (b) An enlarged anterior-posterior view of the 9 mm-diameter dilator tip end. (c) An enlarged lateral view of the 9 mm-diameter dilator tip end. (d) The scheme of the 9 mm-diameter dilator tip end. All the dilators have a sharp end.
Materials and methods
Sixty-two consecutive patients who underwent ACL reconstruction with CDS between November 2013 and January 2016 were included in this study (Table 1). Surgeries were performed by two experienced surgeons (Kee Byoung Lee, Joon Kyu Lee). This study was approved by the institutional review board of our hospital, and informed consent was obtained from all participants.
Demographic data of subjects.
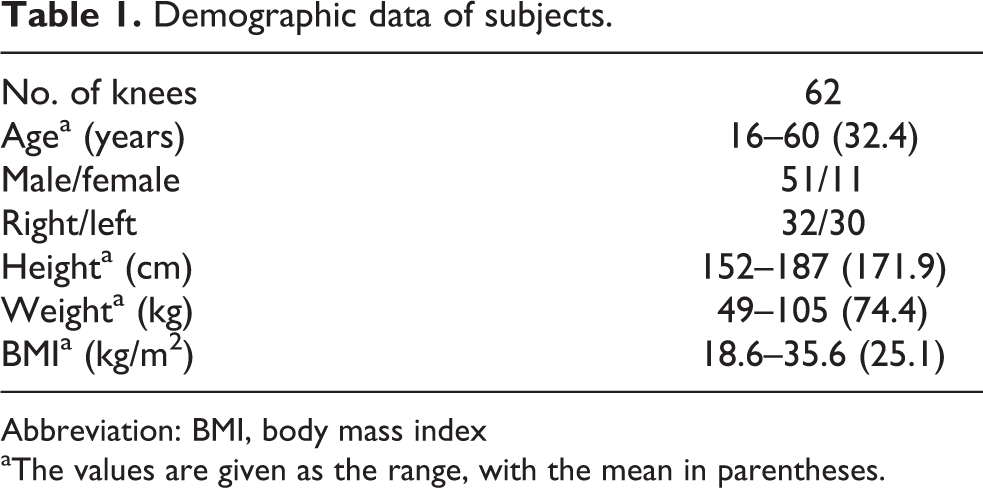
Abbreviation: BMI, body mass index
aThe values are given as the range, with the mean in parentheses.
Surgical procedure
Anterolateral, AM, and accessory anteromedial (AAM) portals were used. The AM portal was made at a slightly more proximal position than usual. The AAM portal was made at 10–15 mm medial to the medial border of the patellar tendon, which was quite lateral compared to the usual AAM portal position and quite distal at the level immediately proximal to the lateral meniscal superior surface (Figure 2).

Portals used (left knee): anteromedial (AM) portal and accessory anteromedial (AAM) portal.
For femoral tunnel creation, an arthroscopic camera was inserted through the AM portal and working devices were inserted through the AAM portal. A drill bit or an awl was first used to locate the anatomic footprint of the ACL. Then, a 4.5 mm-diameter curved guide trocar with a sharp end was inserted at the marked point with the knee flexed to slightly over 90°, which was the angle that allowed trocar passage without medial condyle cartilage damage (Figure 3). The trocar was hammered to the point where the far cortex of the lateral condyle was penetrated completely but the soft tissue was not. This was checked with a C-arm (Figure 4). Then, the trocar was removed and the tunnel length was measured with a curved depth gauge. Next, a 7 mm-diameter curved dilator was inserted at the center of the created tunnel to widen the diameter (Figure 5). The dilator was hammered to the point approximately 5–10 mm short of the far cortex. The tunnel was further widened in a step-by-step manner, increasing by 1 mm dilator diameter to match the graft diameter.

Arthroscopic image of inserting a 4.5 mm-diameter curved guide trocar to the femoral ACL insertion site marked with an awl. ACL: anterior cruciate ligament.
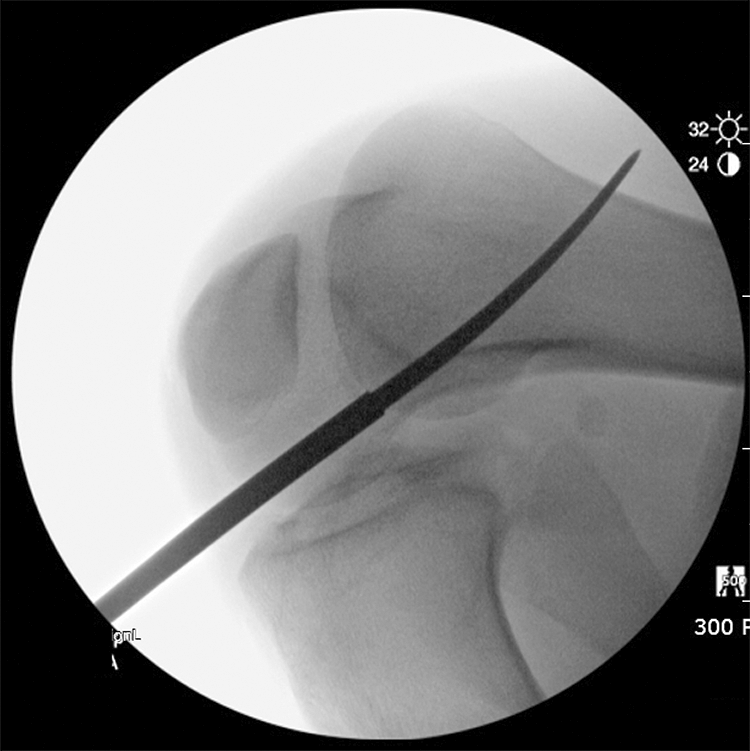
C-arm image checking the trocar penetrating the lateral femoral condyle far cortex.

Arthroscopic image of inserting a 7 mm-diameter curved dilator to the center of the created tunnel to widen the tunnel diameter.
For creating the tibial tunnel, the entry point was set at the level of the tibial tubercle, 2–3 cm medial to the tubercle, superior to the attachment site of the pes anserinus. A guide pin was inserted 55° to the tibial plateau with the use of a tibial drill guide aimed at the center of the ACL footprint. A tibial tunnel was drilled along the guide pin using the standard reamer with a diameter that matched that of the graft.
A tendon graft was passed through the tibial tunnel to the femoral tunnel. Endobutton (fixed loop, usually 15 mm) was used for femoral tunnel fixation, and a bioabsorbable screw was used for the tibial tunnel fixation, augmented by a cortical screw with a spiked washer.
Parameters evaluated
Three-dimensional computed tomographic images were obtained within 3 days after surgery to identify femoral tunnel positions (54 knees). The femoral tunnel positions were evaluated using the quadrant method. The position is defined as the ratio Df/D and Lf/L (D: total depth of the intercondylar notch; Df: distance from the pin position to the intercondylar notch; L: total length of the lateral condyle; Lf: distance from the pin position to the most superior contour of the lateral condyle) (Figure 6). 13 Femoral tunnel length was measured with the curved depth gauge during the surgery. Complications that could be observed intraoperatively, such as posterior wall blowout and cartilage damage of the femoral medial condyle, were checked for. The incidence of peroneal nerve injury was evaluated during hospital stay.

Femoral tunnel position evaluated with the use of the quadrant method from the three-dimensional reconstructed CT image. Superior-inferior position is defined as Lf/L, where L = total length of the lateral condyle, Lf = distance from the center of the femoral tunnel to the most posterior edge of the lateral condyle. Anterior-posterior position in defined as Df/D, where D = total depth of the intercondylar notch, Df = distance from the femoral tunnel to the intercondylar notch. CT: computed tomography.
Results
The mean femoral tunnel position was 32.7% ± 5.4% in the superior-inferior position and 39.1% ± 5.9% in the anterior-posterior position, which could be considered as an anatomic position. Measured length of the femoral tunnel was 39.2 ± 4.1 mm, ranging from 34 mm to 48 mm. The shortest length was 34 mm, which was sufficiently long for adequate fixation. Damage to the cartilage of the medial femoral condyle, peroneal nerve injury, and posterior wall blowout did not occur in any case.
Discussion
This study showed that anatomic femoral tunnel creation through the AM portal could be achieved successfully using CDS with sufficient tunnel length and without serious intraoperative complications.
Several studies have reported anatomic insertion positions of ACL, with reported mean femoral insertion positions by the quadrant method ranging from 23.9% 14 to 43.1% 15 in the superior-inferior position and 28.3% 16 to 44.3% 17 in the anterior-posterior position. Comparing with these reports, femoral tunnel position of 32.7% ± 5.4% in the superior-inferior position and 39.1% ± 5.9% in the anterior-posterior position obtained in our study could be considered anatomic.
One of the well-studied disadvantages of the AM portal technique is short femoral tunnel length. 18 –20 Generally, it is believed that better healing of the graft can be achieved by longer graft tissue within the tunnel. 21 Because the loop length of the Endobutton is usually greater than 15 mm, the graft-tunnel length would be less than 15 mm, if the femoral tunnel is shorter than 30 mm. Although, there are some controversies, there are concerns whether a graft-tunnel length of less than 15 mm in the tunnel can be safe for ACL reconstruction in humans. Therefore, the tunnel length is particularly important when Endobutton is used for femoral tunnel graft fixation, and the femoral tunnel length less than 30 mm should be avoided. 20 In their meta-analysis, Lee et al. reported a mean femoral tunnel length 7.8 mm shorter with the AM portal technique than with the traditional transtibial technique. 22 Although the mean femoral tunnel length of 39.2 ± 4.1 mm in this study was slightly shorter than the reported femoral tunnel lengths with the transtibial technique in the literature (43.3 ± 5.7 mm 20 , 40.5 ± 4.2 mm 23 ), it was much longer than the reported femoral tunnel lengths with the AM portal technique (33.4 ± 6.4 mm 18 , 34.2 ± 4.7 mm 20 , 34.4 ± 2.6 mm 23 ). There was no case of femoral tunnel length less than 30 mm in our study, with a minimum measured femoral tunnel length of 34 mm. With CDS, acceptable femoral tunnel length by the AM portal technique can be achieved.
There are several well-documented possible complications with the AM portal technique during the surgery. 11,19 Because the reamer is inserted through the AM portal for femoral tunnel creation, damage to the cartilage of the medial femoral condyle is possible. In addition, the low trajectory of the guide pin for the femoral tunnel is associated with risks of peroneal nerve damage and posterior wall blowout of the lateral femoral condyle. However, with CDS, because of the curved structure of the dilator, reaching the ACL footprint on the lateral femoral condyle through the AM portal was much easier. Deep knee flexion usually was not needed and damage to the cartilage of the medial femoral condyle could be avoided. Because of the curved (usually upward) trajectory of the femoral tunnel, posterior wall blowout could also be controlled. In addition, the tunnel was widened in a step-by-step manner, which helped prevent posterior wall blowout.
Furthermore, curved tunnel creation could be helpful in double-bundle ACL reconstruction because surgeons could easily prevent overlapping of the tunnels by positioning tunnels in divergent directions. Tunnel wall condensation is another asset of this system. Because a dilator, rather than a reamer, was used in a step-by-step manner, the inner wall of the tunnel could be condensed. 24,25 Also, while reamer could apply heat to the bone, 26 the CDS did not. Because bone quality around the tunnel is a major factor in tunnel widening after surgery, this new system could have an advantage. 27 Further study regarding tunnel wall condensation using CDS is needed to confirm these issues.
Limitations
This study had some limitations. First, this was not a comparative study, so there was no control group. Therefore, we compared the results with the data from the literature. Second, because we concentrated on the device itself in the operation, we did not provide any clinical results such as knee stability and questionnaire scores. Follow-up studies regarding clinical results would be needed. Third, two different surgeons conducted surgeries. This could alter results. However, one surgeon (Joon Kyu Lee) attended all the surgeries by the other surgeon (Kee Byoung Lee). Fourth, the increment of the CDS diameter was 1 mm. Therefore, graft-tunnel mismatch could occur if the graft diameter was 7.5 mm, 8.5 mm, or 9.5 mm. However, even for the standard reamers for femoral tunnel creation with traditional techniques, the usual increment of the reamer diameter is 1 mm.
Conclusion
This study showed that ACL reconstruction with CDS resulted in anatomic positioning of the femoral tunnel and sufficient femoral tunnel length without intraoperative complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Hallym University Research Fund 2016 (HURF-2016-09).