
Abstract
Background:
Sex-specific quantification of cam morphology in patients with femoroacetabular impingement syndrome may improve diagnostics, surgical planning, and outcomes.
Purpose:
To (1) examine differences between men and women with symptomatic cam deformities based on deformity location, magnitude, and extent; (2) assess the association between cam deformity and labral pathology; and (3) evaluate the relationship between cam deformity and patient-reported outcome measures after hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Computed tomography (CT) scans were acquired in 98 consecutive patients before hip arthroscopy for femoroacetabular impingement syndrome. Custom software was used to generate 3-dimensional bone models and align them to a standard coordinate system. The alpha angle was measured at the 12-, 1-, 2-, and 3-o’clock positions, with 12 and 3 o’clock corresponding to the superior and anterior aspects of the femur, respectively. These alpha angle measurements were used to define the cam midpoint and extent. The labral tear midpoint and extent were evaluated intraoperatively. Bivariate correlation analysis was used to evaluate the association between the cam and labral tear midpoints and between the extent of the cam morphology and labral tearing.
Results:
The 3-dimensional models were analyzed in a cohort of 69 female and 29 male patients. Male patients were older (mean ± SD, 38.9 ± 12.6 vs 30.7 ± 12.2 years, P = .006) and had a greater body mass index (27.8 ± 4.4 vs 25.3 ± 5.6 kg/m2, P = .005). Male patients had greater alpha angle measures at 12, 1, and 3 o’clock (P < .05) and a greater maximum alpha angle (69.0° ± 18.8° vs 62.1° ± 21.0°, P = .031); the location of their maximum cam impingement was also significantly different (P < .05) when compared with female patients. Cam impingement (2:06 ± 1:09 vs 1:33 ± 1:16 clockfaces, P = .032) and labral tearing (3:02 ± 0:35 vs 2:34 ± 0:53 clockfaces, P = .003) in men extended over a greater region of the femoral clockface when compared with women. Significant correlations were demonstrated between the cam and labral tear midpoint locations (r = 0.190, P = .032) and the extent of the cam deformity and labral tearing (r = 0.203, P = .024). There were no sex-based differences in patient-reported outcome measures at baseline or 2-year follow-up.
Conclusion:
Male patients possessed greater cam deformity magnitude and extent when compared with female patients. Cam pathomorphology was associated with the location and extent of labral tearing.
Femoroacetabular impingement syndrome (FAIS) has become increasingly recognized as a common cause of disabling hip pain, functional limitations, and gait abnormalities. 3,21 Cam-type FAIS is characterized by asphericity of the femoral head, leading to a reduced head-neck offset. 16 Repetitive contact of the cam deformity at the femoral head-neck junction within the acetabulum has been shown to lead to increased risk of injury to the labrum and articular cartilage surfaces, resulting in osseous changes and the potential for early-onset hip osteoarthritis. 12,18 As a result, increased interest has been placed on hip arthroscopy procedures as a minimally invasive method to effectively treat symptomatic cam deformities and injuries to the labrum and cartilage. 6,7,44
Cam deformities are 3-dimensional (3D) deformities that have traditionally been identified and quantified by alpha angle measurements using radiographs and magnetic resonance imaging (MRI). 39 However, radiographs have been shown to be sensitive to variations in projection, resulting in poor interobserver reliability 31 and difficulty quantifying the extent of the cam, 17,37 leading to missed diagnoses, especially in women. 47 Meanwhile, MRI measurements largely rely on a best-guess technique when defining the femoral neck axis, leading to issues with quantification of deformity magnitude. 35 As a result, 3D evaluation utilizing computed tomography (CT) has been developed and validated to allow for more accurate and reliable diagnosis and characterization of cam deformities. 4,27,28 Three-dimensional analysis also permits quantification of lesion extent by dividing the femoral region in radial sections based on clockface measurements, allowing for improved deformity identification and localization. 21,46
Cam deformities surpassing certain alpha angle values have been shown to increase the risk for chondral 12,27,28 and labral 25 damage, with different cutoff values in men and women. 17 However, specific variables related to cam deformity location and extent, especially with regard to differences between men and women, remain relatively unknown. The purpose of this investigation was to (1) examine differences between men and women with symptomatic cam deformities undergoing hip arthroscopy based on cam deformity location, magnitude, and extent utilizing 3D CT analysis; (2) assess the association between cam deformity and labral pathology; and (3) evaluate the relationship between cam deformity and patient-reported outcome measures (PROMs) after hip arthroscopy. Our hypotheses were as follows: (1) there would be no differences in cam deformity location between the sexes 47 ; (2) men would possess larger cam deformities based on alpha angle measures 13,47 ; (3) the extent of cam morphology would be associated with the extent of intraoperative labral pathology; and (4) no differences in PROMs would be appreciated at baseline or 2-year minimum follow-up. 10,13
Methods
Patient Selection and Imaging
This study received institutional review board approval to prospectively recruit and retrospectively analyze imaging and outcomes of patients undergoing hip arthroscopy for FAIS by the senior author (S.J.N.). All patients provided informed consent before enrollment and initiation of data collection. Inclusion criteria were primary hip arthroscopy between March 2015 and July 2015 and diagnosis of FAIS based on clinical and radiographic evidence of FAIS, failure of nonoperative therapy (oral anti-inflammatories and/or intra-articular cortisone injection, physical therapy), CT imaging of the hip, and minimum 2-year follow-up. The exclusion criteria were revision hip surgery, developmental hip disorders (Legg-Calvé-Perthes disease, slipped capital femoral epiphysis), hip dysplasia (lateral center-edge angle <20°), Tönnis grade >1, concomitant gluteus medius or minimus repair, and CT imaging from an outside facility.
Preoperative CT scans were acquired on consecutive patients meeting the study criteria. In a recent 3D CT study, Zhang et al 48 demonstrated sex-specific differences in cam morphology in 43 patients (56 lesions). To reduce the risk of a type 2 error, 100 patients were prospectively enrolled, and 2 were later excluded because of image artifact. CT scans (BrightSpeed; GE Healthcare) included the left and right hips from the anterior superior iliac spine to below the lesser trochanter as well as the knee. The CT scan acquisition was based on the following parameters: 120 kV, 250 mAs, slice thickness of 0.675 mm, and an in-plane resolution <1 × 1 mm (range, 0.66-0.98 mm). All CT images were exported as DICOM (Digital Imaging and Communication in Medicine) files and stored in our institutional PACS (picture archiving and communication system).
3D Geometric Modeling of Preoperative CT Scans
Custom software (HipMap FAI Analysis; Stryker) was used for the generation of 3D osseous models (segmentation), alignment of the models according to a standard coordinate system, and anatomic measurements. Three-dimensional models of the left and right proximal femur, pelvis, and distal femur (knee) were created by semiautomated segmentation. The initial segmentation was based on a statistical shape model and random forest optimization. The segmentation was reviewed and manually edited if necessary. Alignment of the 3D models was performed to reduce the effect of inaccuracies caused by differences in patient positioning during image acquisition. 42 The 3D models were aligned by rotating around the femoral head center. For the pelvis, the coronal plane was defined by the anterior pelvic plane (left and right anterior superior iliac spine and left and right pubic protuberances) and the horizontal axis by the left and right femoral head centers. For the femur, the line from the femoral head center to the center of the posterior femoral condyles defined the vertical axis (perpendicular to the transverse plane of the pelvis), and the posterior condylar axis was used to determine the horizontal axis (perpendicular to the sagittal plane of the pelvis). All analyses were performed by an operator with a doctoral degree and extensive experience in image-based studies (F.L.). Interrater reliability was performed by additional graders with master degrees in engineering.
Quantifying the Alpha Angle
The 3D model–based alpha angle was measured at the 12-, 1-, 2-, and 3-o’clock positions. The femoral clockface positions were defined by using radial sequences around the axis of the femoral neck, with the 12- and 3-o’clock positions corresponding to the superior and anterior aspects of the femur, respectively (Figure 1A). The alpha angle was defined by the angle created by the femoral neck axis and the ray at which the distances from the femoral head center to the bone surface exceeded the best-fit sphere radius by 1 mm to account for scanning-resolution error (Figure 1B). The femoral neck axis was defined as the line between the 3D femoral head center (based on a sphere fit on the load-bearing portion of the femoral head) and the 3D femoral neck center (based on a surface patch and smallest cross-sectional area).

(A) Alpha angle measurement at 12, 1, 2, and 3 o’clock based on the 3-dimensional model. (B) Line A: line from center of sphere to femoral neck midpoint. Line B: line from center of best-fit sphere to location at which the femoral head loses sphericity. Line C: line from center of sphere to the location at which the femoral head-neck junction exceeds the best-fit sphere by 1 mm, accounting for resolution error. The angle between lines A and C is the 3-dimensonal–based measure of the alpha angle for this study.
Alpha Angle Measures Compared by Patient Sex
The alpha angle at the 12-, 1-, 2-, and 3-o’clock positions was determined for each patient. We also identified the maximum alpha angle and the femoral clockface plane in which each patient’s maximum alpha angle occurred.
Cam Morphology: Midpoint and Extent
The alpha angle measures on the 3D bone models were used to define the cam midpoint and extent of the deformity. The cam midpoint was defined by the location of the maximum alpha angle for each patient. To define the extent of the cam deformity, the presence of cam morphology as a binary measure at each femoral clockface was determined. A pathologic threshold >50° was used to define cam pathomorphology. 39 The cam extent was defined as the number of clockfaces with cam morphology across the femoral clockface—for example, for a patient with alpha angle measures of 12 o’clock (47.5°), 1 o’clock (53.5°), 2 o’clock (55.5°), and 3 o’clock (42.5°), the cam extent is 2 clockfaces. In addition to alpha angle measures, model-based femoral torsion measures were collected for each patient. Femoral torsion was measured as the angle between the femoral neck axis and the posterior condylar axis on the transverse plane after femoral alignment.
The intra- and interrater reliability was <1° for femoral torsion and <1° for alpha angle measures at each clockface, with a mean difference of 0.11° (12 o’clock), 0.89° (1 o’clock), 0.82° (2 o’clock), 0.77° (3 o’clock), and 0.43° (femoral torsion) among 3 raters and a mean deviation of 0.09°, 0.78°, 0.67°, 0.73°, and 0.33° among 3 time points, respectively.
Labral Tear: Midpoint and Extent
Intraoperative evaluation of labral tearing was performed on all patients by the senior author (S.J.N.) and used to define the labral tear midpoint and extent of the labral tear. The labral tear was identified, and the most posterior and anterior boundaries of the tear were recorded. The clockface was defined with 12 o’clock at the most superior aspect, 6 o’clock at the inferior aspect of the acetabular notch, and 3 o’clock at the anterior aspect of the acetabulum. 9 The tear midpoint was defined as the point equidistant from the most anterior and posterior aspects of the tear (eg, for a patient with an anterior and posterior boundary of 12 and 2, respectively, the tear midpoint is 1 o’clock). The tear extent was defined as the number of clockfaces spanned from the most anterior and posterior aspects of the tear, with the extent of tearing reported as whole number intervals—for example, for a patient with anterior and posterior boundaries of 12 and 2, respectively, the tear extent is 2 clockfaces).
Functional Outcomes
Patients completed PROMs at their preoperative visits and a minimum of 2 years after hip arthroscopy. PROMs included the Hip Outcome Score–Activities of Daily Living, 33 Hip Outcome Score–Sports Subscale, 34 modified Harris Hip Score (mHHS), 8 iHOT-12 (International Hip Outcome Tool), 19 and visual analog scale for pain and satisfaction.
Surgical Technique
All hip arthroscopies were performed at a high-volume academic center by a fellowship-trained hip arthroscopic surgeon (S.J.N.), as previously described. 14,22 Briefly, an interporal capsulotomy was performed to establish access to the central compartment. Once it was established, procedures included acetabuloplasty (if indicated), labral debridement or repair (depending on labral condition), and chondral lesion debridement (to stable margins). In all cases, a vertical T-capsulotomy was performed to assess cam morphology. A comprehensive cam resection was performed to address the abnormal femoral bony morphology. Under direct visualization with fluoroscopic guidance, a dynamic examination was performed to confirm complete resection of bony impingement. The T-capsulotomy was repaired using a suture-shuttling device starting at the base of the vertical portion, followed by the interporal segment. 5 Rehabilitation was initiated on postoperative day 1 and followed a 4-phase protocol as previously described. 32
Statistical Analysis
All 3D model alpha angle measurements were evaluated before analysis to determine if parametric statistical assumptions were met. The Shapiro-Wilk test was used to determine normality of data. For outlier detection, the interquartile method was performed on 3D model–based measures and radiographic measures of alpha angle. 30 All identified outliers underwent additional review. The review process consisted of independent examination of the preoperative CT and 3D models to detect potential segmentation error and/or 3D measurement error. Three authors—an orthopaedic surgeon (D.M.K.), a trained medical student (T.D.A.), and a researcher well versed in FAIS imaging studies (P.M.)—agreed that all outliers were not due to segmentation artifact or measurement error. As such, no outliers were excluded from subsequent analysis. An independent-samples t test was used for the between-group measures comparing male and female patients. In cases of parametric assumption violation, nonparametric analogue tests were used. Chi-square analysis was used to analyze categorical variables. An a priori α level was set at 0.05 to indicate statistical significance. All statistical analysis was performed using SPSS (Version 26; IBM).
Results
Patient Cohort
Three-dimensional models were analyzed among 98 patients with a mean ± SD age of 33.1 ± 12.8 years and body mass index of 26.1 ± 5.4 kg/m2. The cohort contained 69 female and 29 male patients. Male patients were older (38.9 ± 12.6 vs 30.7 ± 12.2 years, P = .006) and had a greater body mass index (27.8 ± 4.4 vs 25.3 ± 5.6 kg/m2, P = .005).
Alpha Angle Measures Based on Patient Sex
The mean radial alpha angles at the 12-, 1-, 2-, and 3-o’clock positions were 48.1° ± 16.4°, 57.4° ± 16.2°, 55.2° ± 18.4°, and 51.4° ± 23.8°, respectively (Figure 2). Alpha angle measurements overall and by sex are shown in Table 1. Male patients had significantly greater alpha angle measures at 12, 1, and 3 o’clock, although the difference at 2 o’clock was not significant (P = .078). The mean maximum alpha angle across the clockface for all patients was 64.2° ± 20.5°. Male patients had a greater mean maximum alpha angle than female patients (P = .031). The percentage of patients with maximum alpha angles at each clockface is also shown in Table 1. Chi-square analysis indicated differences between males and females in the proportion of patients with a maximum alpha angle at each clockface (P = .049).
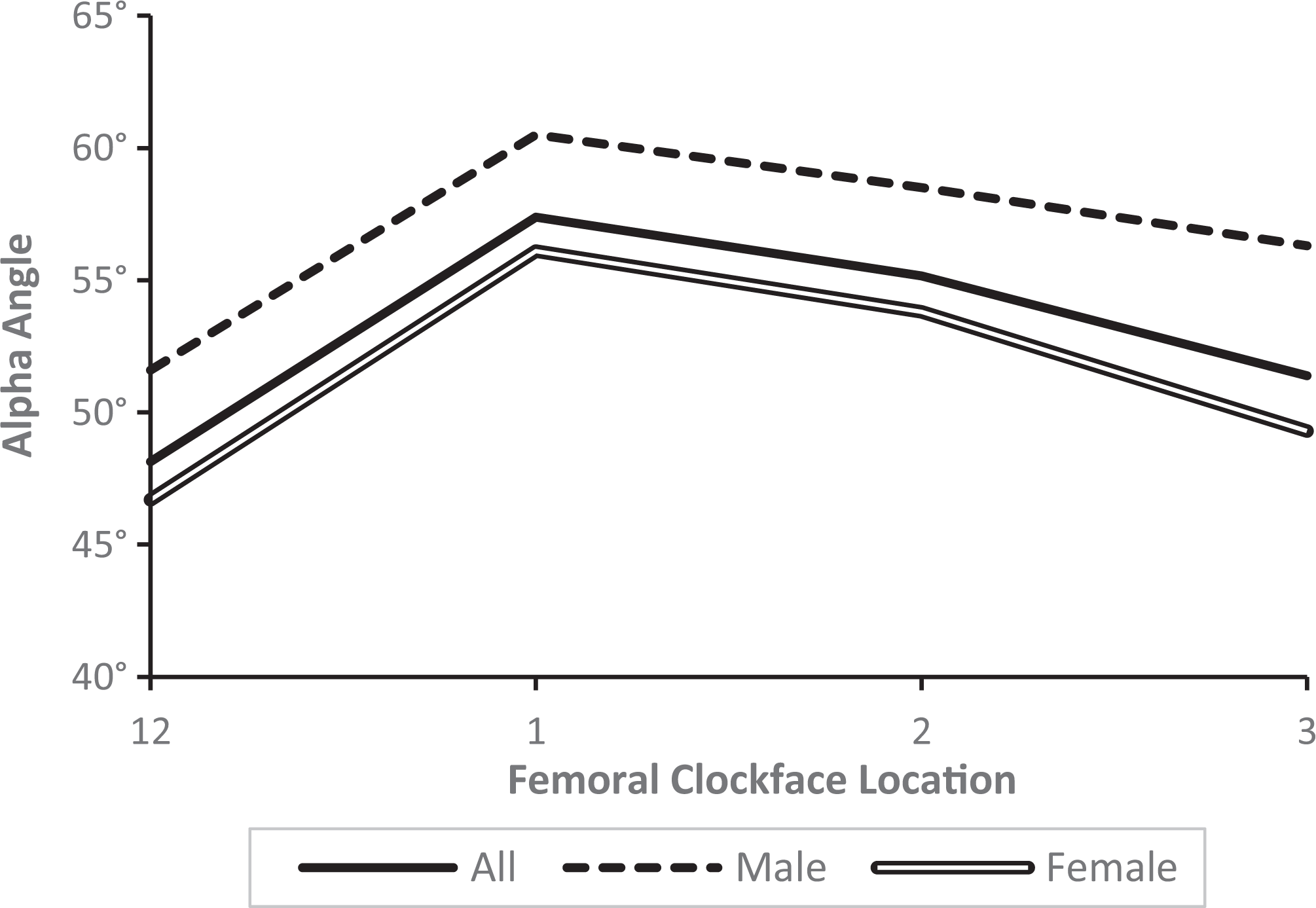
Mean alpha angle measurement on computed tomography based on 3-dimensional–reconstructed hip models according to femoral clockface.
Alpha Angles by Patient Sex: Mean, Maximum, and Location of Maximum a

a Values are presented as mean ± SD unless noted otherwise. Bold P values indicate statistically significant sex-based differences (P < .05).
Cam Morphology: Midpoint and Extent
The mean cam midpoint along the femoral clockface for all patients was 1:23 ± 0:53 o’clock. The mean cam spanned 1:43 ± 1:15 hours of the clockface. There were no differences in the cam midpoint between men (1:29 ± 1:05 o’clock) and women (1:21 ± 0:47 o’clock, P = .742) (Figure 3). However, cam deformities in male patients extended over a greater region of the femoral clockface (2:06 ± 1:09 vs 1:33 ± 1:16 clockfaces, P = .032).
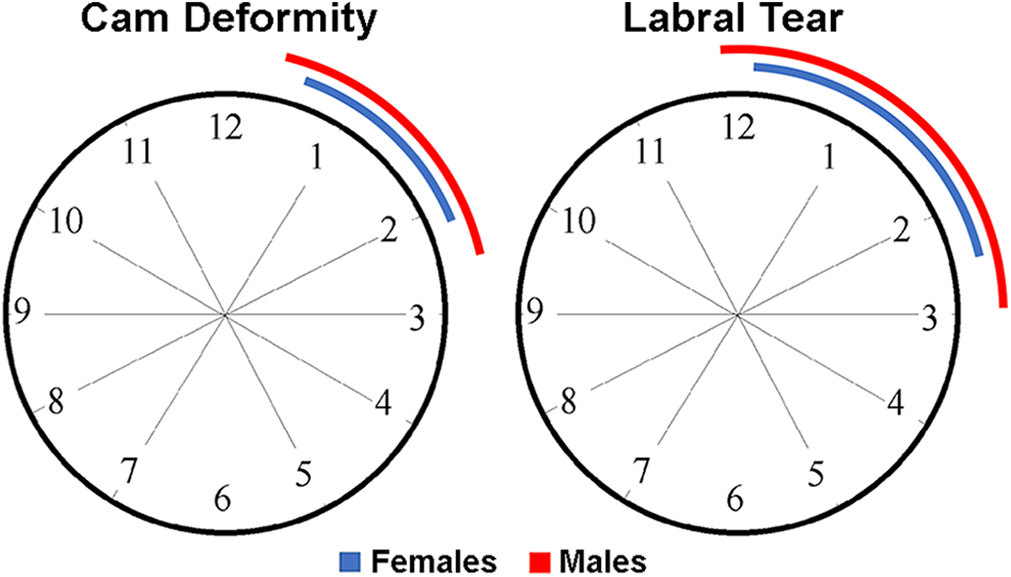
Mean midpoint and extent of cam deformity and labral tear in male and female patients.
Labral Tear: Midpoint and Extent
The mean tear midpoint along the femoral clockface for all patients was 1:24 ± 0:23 o’clock. The mean tear spanned 2:41 ± 0:50 hours of the clockface. There were no differences in the tear midpoint between men (1:24 ± 0:16 o’clock) and women (1:24 ± 0:25 o’clock, P = .897). However, labral tearing in male patients extended over a greater region of the clockface (3:02 ± 0:35 vs 2:34 ± 0:53 clockfaces, P = .003) (Figure 3).
Relationship Between Cam Morphology and Labral Pathology
Bivariate correlation analysis indicated a significant correlation between the location of the cam and labral tear midpoints (r = 0.190, P = .032). In addition, there was a significant correlation between the extent of the cam deformity and labral tear (r = 0.203, P = .024).
Femoral Torsion Measures
The mean femoral torsion for the entire cohort was 5.6° ± 9.4°. Analysis of femoral torsion revealed no difference between male (3.7° ± 8.7°) and female patients (6.4° ± 9.6°, P = .186).
Patient-Reported Outcome Measures
Of the 98 patients, 81 (81.8%) completed postoperative PROMs at 26.0 ± 2.1 months. Analysis of PROMs revealed no differences between male and female patients in Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sports Subscale, mHHS, iHOT-12, or visual analog scale for pain or satisfaction at baseline or latest follow-up (Table 2). No significant correlations were appreciated between pre- and postoperative PROMs and the size or location of the cam deformity.
Preoperative and 2-Year Patient-Reported Outcomes by Sex a

a Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Discussion
The main findings from this investigation were that male patients possessed a greater magnitude and extent of cam deformities, primarily at the 12-, 1-, and 3-o’clock positions, when compared with female patients. Alpha angle magnitude was greatest at the 1-o’clock position in men and women. The magnitude and extent of cam morphology were associated with labral pathology, while men possessed a larger extent of acetabular labral tearing. Despite differences in cam and labral pathology, no significant differences in PROMs were appreciated at baseline or at 2-year follow-up between male and female patients.
The maximum alpha angle was 64.2° ± 20.5°, with the greatest magnitude located predominately at the 1-o’clock position, corresponding to the superolateral area of the femoral neck. This finding is consistent with other reports regarding the anterosuperior aspect of the femoral head-neck junction possessing the largest alpha angle measurements. Gollwitzer et al 16 examined maximum alpha angle location in 1312 hips from 656 patients undergoing CT scans for disorders not related to the hip at a mean age of 61.2 years (range, 18-93 years). The authors reported that the mean maximum alpha angle was 59° ± 9.4° and located anterosuperiorly at the 1:36-o’clock position of the femur. Han et al, 21 evaluating 100 patients without hip joint pain using CT, noted the greatest mean alpha angle measurements (52.45°; range, 43.3-65.5°) at the 1-o’clock position, with the prevalence of cam deformity (alpha angle >55°) being 18% at the 1-o’clock position. Multiple other investigations have corroborated the alpha angle maximum located between the 1- and 2-o’clock positions at the anterosuperior region of the head-neck junction. 11,40,41,45 As such, when symptomatic and asymptomatic patients with FAIS are evaluated, careful assessment for bony deformity at the anterosuperior aspect is critical to allow for appropriate diagnosis and surgical planning when decompression is indicated.
Male patients possessed greater mean alpha angle measurements overall and at the 12-, 1-, and 3-o’clock positions, suggesting a lateral extension of cam morphology. Previous investigations have supported the presence of smaller alpha angles in women vs men. In a cohort study comparing pre- and postoperative outcomes in men (n = 59) and women (n = 72) undergoing hip arthroscopy for FAIS, Flores et al 13 reported significantly smaller preoperative alpha angles in women (59.1°) vs men (63.7°, P < .001). Yanke et al 47 similarly evaluated sex differences using CT quantification for 138 patients (69 male, 69 female) with hip impingement, noting cam height in men to be significantly greater (1.51 ± 0.75 mm) when compared with women (0.66 ± 0.61 mm, P < .001). Moreover, cam volume was significantly larger in men (433 ± 471 mm3) vs women (89 ± 124 mm3, P < .001), while deformities spanned a significantly larger aspect of the clockface (3:43 ± 1:29 o’clock for men vs 2:54 ± 1:09 for women, P = .02).
Halim et al 20 similarly reported significantly greater alpha angle measures in symptomatic males vs their female counterparts. The authors postulated that female patients experience symptoms despite smaller cam deformities because of the increased hip flexion during sport activity secondary to decreased muscle mass and increased ligamentous laxity when compared with male patients. As a consequence of the increased range of motion in female patients, bony impingement may occur in the setting of smaller cam lesions. Given the greater magnitude and extent of cam deformity in male patients, increased operative duration and additional intraoperative fluoroscopic images may be required to ensure a complete bony resection and restoration of normal femoral anatomy.
The present study demonstrated that the cam deformities in males extended over a greater extent of the clockface and were associated with an increase in labral tear extent in comparison with female patients. Significant correlations were appreciated between the midpoint of cam deformities and the midpoint of labral tearing as well as between the extent of deformities and the extent of labral tearing. Greater alpha angle measurements have been shown to correlate with an increased risk for chondral damage 1,39 and may account for the greater extent of acetabular labral tears in male vs female patients. Utilizing cross-table lateral radiographs in 102 consecutive patients with symptomatic FAIS undergoing hip arthroscopy, Johnston et al 25 found that increased femoral neck offset angle positively correlated with increased labral injury. Further investigations are required to elucidate the role of increased cam deformity size and other potential intra- and extra-articular variables predisposing men to increased injury in the setting of FAIS.
Despite differences in alpha angle magnitude and the prevalence of cam deformities, no significant differences in PROMs were appreciated between men and women at baseline or 2-year follow-up. The equivalent baseline scores between men and women are in contrast to previous studies that cited increased preoperative disability and decreased function on patient-reported outcome surveys in women vs men. 23,24,26,38,43 Impellizzeri et al 24 speculated that women possessed worse preoperative scores because of an increased degree of soft tissue laxity, contributing to increased pain preoperatively. Meanwhile, Hetsroni et al 23 theorized that differences in muscle mass and protective dynamic stabilization of the painful hip joint may be more compromised in symptomatic female patients.
Investigations examining postoperative outcomes have similarly demonstrated the ability of men and women to experience improvement after hip arthroscopy for FAIS. Flores et al 13 reported that women had equivalent rates of achieving the minimal clinically important difference for the mHHS and SF-12 (12-Item Short Form Health Survey) as well as the patient-acceptable symptom state for the mHHS, at a minimum 2 years after surgery when compared with men. Furthermore, Cvetanovich et al 10 found no sex-based differences in minimal clinically important difference and patient acceptable symptom state in 37 adolescent and young adult patients (mean age, 17.0 ± 1.4 years) undergoing hip arthroscopy for FAIS with minimum 2-year follow-up. In a matched-group analysis, Frank et al 15 examined male and female patients undergoing hip arthroscopy for FAIS with minimum 2-year follow-up, and they noted significant improvement in all outcomes from pre- to postoperative assessments. However, women aged older than 45 years had lower outcome scores than those aged 30 to 45 years, as well as all male groups. Determination of factors beyond patient age influencing differences in outcomes at baseline and postoperative follow-up are necessary to better counsel patients indicated for hip arthroscopy on the potential for clinical improvement after surgery.
Limitations
This study is not without limitations. Despite known differences between men and women in acetabular version, 2,29 these measurements were not performed, potentially confounding the results. All hip arthroscopy procedures were performed by a single surgeon at a single institution, limiting the generalizability of the outcomes to other surgeons and institutions incorporating different surgical techniques with differing levels of technical proficiency and surgical volume. Long-term outcomes between men and women after hip arthroscopy were not evaluated—namely, the differences in the rate of revision surgery or conversion to total hip arthroplasty. Correlation of measurements to plain radiography and MRI was not performed because of the high rate of inaccuracies and variability present, as based on individual observer interpretations of proximal femoral morphology. 35,36
The alpha angle was measured from 12 to 3 o’clock and may fail to capture cam morphology outside the more typical pathologic region. Additionally, the analysis did not consider potentially associated patient-specific variables involving the hip, such as the depth or size of the femoral head. Given the limited sample size, a matched-group comparison based on patient age, activity level, and body mass index was not feasible. Moreover, no control group was included for comparison. The present study did not include nonoperative patients, which could result in selection bias. Postoperative CT scans were not performed, limiting the ability to evaluate the relationship between pre- and postoperative morphologic parameters and outcomes. Last, this 3D method of quantifying the alpha angle requires that the distance from the femoral head center to the bone surface exceed the best-fit sphere radius by 1 mm to account for resolution error. Therefore, this results in an underestimation of the alpha angle as depicted in Figure 1B.
Conclusion
Male patients possessed greater cam deformity magnitude and extent when compared with female patients, while cam pathomorphology was associated with the location and extent of labral tearing. However, no sex-specific differences in PROMs were appreciated.
Footnotes
Acknowledgment
The authors thank Haji Mohammed Kampli, Daniel Greenfeld, and Franziska Breuner for their support with the study analyses.
Final revision submitted February 9, 2022; accepted February 25, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.K. has received research support from Arthrex and education payments from Medwest and Smith & Nephew. F.L. is an employee of Stryker. J.C. has received education payments from Arthrex and Smith & Nephew; consulting fees from Arthrex, DePuy, Linvatec, and Smith & Nephew; speaking fees from Linvatec; and hospitality payments from Stryker. S.J.N. has received education payments from Elite Orthopedics and consulting fees and royalties from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush Medical Center (12022108-IRB01-CR09).