
Abstract
Background:
Anatomic placement of the meniscal allograft is imperative to achieve satisfactory outcomes after meniscal allograft transplantation (MAT). Few studies have reported on the accuracy of the provisional location of the center of the anterior horn of the lateral meniscus (AHLM).
Hypothesis:
The authors hypothesized that the provisional center would not coincide with the anatomic center of the AHLM.
Study Design:
Descriptive laboratory study.
Methods:
Tibial plateaus were retrieved from 93 consecutive patients who underwent total knee arthroplasty. A complete radial cut was made 2 cm lateral to the insertion of the AHLM on the retrieved tibial plateau. While moving the stump of the anterior horn with forceps, the center of the insertion was determined, and a Kirschner wire (provisional wire) was drilled into the location. The insertion area of the AHLM was dissected carefully, and the periphery of the insertion area of the anterior horn was marked. Another Kirschner wire (anatomic wire) was drilled into the center of the dissected anterior horn. The resected tibial plateau was positioned so that the longitudinal line of the tibial plateau was aligned on a plastic ruler. The distance between the provisional and anatomic wires was measured by a digital caliper along the longitudinal and vertical axes.
Results:
The mean distance between the provisional and anatomic wires was 2.5 ± 1.2 mm. The provisional wire in 14 patients (15%) was placed at the anatomic center. In 36 patients (39%), the provisional wire was drilled anterolateral to the anatomic center, and in 18 patients (19%), the wire was drilled anteromedial to the anatomic center. In 21 patients (23%), the provisional wire was located within 2 mm of the anatomic center, and in 62 patients (67%), the wire was located within 3 mm of the anatomic center.
Conclusion:
The provisional wire was located a mean of 2.5 mm from the anatomic center, and only 23% of patients had wires that were located within 2 mm of the anatomic center. In 39% of patients, the provisional wire was drilled anterolateral to the anatomic center. This finding needs to be considered during lateral MAT.
Clinical Relevance:
Without dissection of the AHLM, the determination of the anatomic center of the anterior horn is not accurate during lateral MAT.
Meniscal allograft transplantation (MAT) has been performed to help prevent the development of arthritic changes in young, active patients after subtotal or total meniscectomy. However, a nonanatomic horn position increases the risk of early graft failure after MAT. 5 Therefore, anatomic placement of the meniscal allograft is imperative to achieve satisfactory outcomes. 2,5,10 Although some surgeons prefer to apply meniscal allografts without bone block fixation, 3 the lateral meniscal allograft is usually prepared with a bony bridge or keyhole connecting both horns because the distance between the anterior and posterior horns is very close. 2,6,19 Accurate placement of the lateral meniscal allograft depends on the position of the bony bridge or keyhole. However, errors in placement of the bony bridge or keyhole during lateral MAT can occur in the coronal, sagittal, and axial planes, resulting in midbody extrusion. 2,10
When preparing the bony keyhole in lateral MAT, a guide pin is drilled below the tibial plateau under fluoroscopic control to confirm the position of the guide pin in the coronal and sagittal planes. The guide pin is usually drilled below the lateral tibial spine, and the lateral tibial spine is used as a landmark to decide the position of the bony keyhole. 3,10,19 However, the direction of the lateral tibial spine is not coincident with the line connecting the centers of both horns of the lateral meniscus. 1 Moreover, the arthroscopic location of the center of the root of the anterior horn of the lateral meniscus (AHLM) is difficult to identify. The AHLM is braided with the tibial insertion of the anterior cruciate ligament (ACL). 8 The overlap of the ACL on the root of the AHLM averages 63.2%. 9 Therefore, it is difficult to locate the center of the insertion of the anterior horn without dissection. Some researchers mark the anterior horn sites using a radiofrequency device via arthroscopic surgery or through arthrotomy. 11 However, this provisional marking of the center of the anterior horn has not been validated yet.
There is a paucity of studies reporting the accuracy of the provisional location of the center of the AHLM. The purpose of this study was to evaluate the accuracy of the provisional location of the center of the AHLM on the tibial plateau. We hypothesized that the provisional center would not coincide with the anatomic center of the AHLM.
Methods
From January 2019 to December 2019, tibial plateaus were retrieved from 93 consecutive patients who underwent total knee arthroplasty. The inclusion criterion was a tibial plateau that showed medial compartment osteoarthritis. Exclusion criteria were osteoarthritic changes, meniscal tears, and previous fractures in the lateral compartment. A total of 93 resected tibial plateaus were used for gross evaluations in this study. All patients were informed that retrieved tibial plateaus were to be dissected for an experimental study, and they consented with a written document. The study protocol was reviewed and approved by our institutional review board.
A radial cut was made 2 cm lateral to the insertion of the AHLM of the retrieved tibial plateau. While moving the stump of the anterior horn with forceps, the center of the insertion was determined, and a Kirschner wire (provisional wire) was drilled into the location. The insertion area of the AHLM was dissected carefully. The periphery of the insertion area of the anterior horn was marked with a sharp marking pen. Another Kirschner wire (anatomic wire) was drilled into the center of the dissected anterior horn (Figure 1). The resected tibial plateau was positioned so that the longitudinal line of the tibial plateau was aligned on a plastic ruler. Another ruler was placed vertically to the longitudinal line of the tibial plateau. The distance between the provisional and anatomic wires was measured along the longitudinal and vertical axes using a Digimatic Caliper (Mitutoyo).
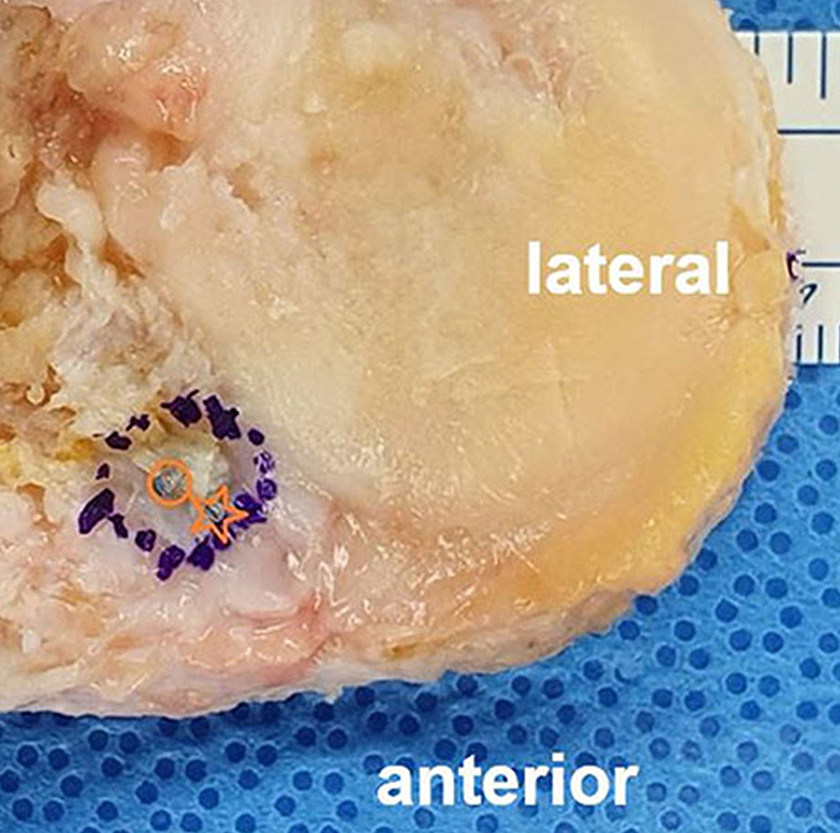
A tibial plateau from a left knee showing the positions of the provisional wire (star) and anatomic wire (circle). The blue dashed circle indicates the periphery of the anterior horn insertion.
Results
The mean distance between the provisional and anatomic wires was 2.47 ± 1.23 mm. The provisional wire in 14 patients (15%) was placed at the anatomic center. In 36 patients (39%), the provisional wire was drilled anterolateral to the anatomic center, and in 18 patients (19%), the wire was drilled anteromedial to the anatomic center. Additionally, in 11 patients (12%), the provisional wire was placed posterolateral to the anatomic center, and in 9 patients (10%), the wire was placed posteromedial to the anatomic center. The provisional wire was located just anterior to the anatomic center in 3 patients. Further, the provisional wire was located just posterior to the anatomic center in 1 patient and medial to the anatomic center in 1 patient. In 21 patients (23%), the provisional wire was located within 2 mm of the anatomic center, and in 62 patients (67%), the wire was located within 3 mm of the anatomic center (Figure 2).

Scatter plot showing the position of each provisional wire in the mediolateral and anteroposterior directions. The anatomic wire is located at the origin.
Discussion
The most important finding of this study was that the provisional wire was located a mean of 2.5 mm from the anatomic center and that only 23% of patients had wires that were located within 2 mm of the anatomic center. In 39% of patients, the provisional wire was drilled anterolateral to the anatomic center. Without dissection of the AHLM, the arthroscopic location of the center of the anterior horn is difficult and inaccurate to identify.
Several studies have reported on the anatomic relationship between the AHLM and the tibial attachment of the ACL. 9,15,18 Although Kusano et al 8 reported that a clear border was found histologically to be dividing the ACL and AHLM fibers and that their fibers never blend, most researchers reported that the insertion of the AHLM and the tibial insertion of the ACL are blended or overlapped. 7,9,13,15,16,18 Kohn and Moreno 7 and Siebold et al 13 reported that the anterior insertion of the lateral meniscus is blended with the tibial insertion of the ACL. Urban et al 16 reported that the insertion of the AHLM is overlapped by the insertion of the posterolateral bundle of the ACL. Overlapping of the AHLM by the tibial insertion of the ACL was quantitatively investigated; the overlap of the ACL on the root of the AHLM averages 63.2%. 9 In the coronal plane, the tibial insertion of the ACL overlapped the AHLM insertion by a mean of 41.0% ± 8.9%. In the sagittal plane, the tibial insertion of the ACL overlapped the AHLM insertion by a mean of 53.9% ± 4.3%. 15
Because the tibial insertion of the ACL considerably overlaps the center of the AHLM, the distance between the centers of the ACL and the AHLM is very close. The center of the ACL is located 5.0 mm posteromedial to the center of the root of the AHLM. 9 Other researchers reported that the center of the ACL attachment is 7.5 mm from the center of the root of the lateral meniscus. 20 In lateral MAT, an 8- or 9-mm bony trough or keyhole is prepared under the lateral tibial spine. If the keyhole or trough is placed anatomically at the center of the AHLM, a 1- to 2.5-mm distance will be left from the center of the ACL. The anterolateral portion of the tibial insertion of the ACL may be injured. The current study demonstrated that the provisional wire in 9 patients (10%) was placed posteromedial to the anatomic center. The provisional location in the posteromedial direction may carry a risk of injuries to the ACL insertion.
Without dissection of the tibial insertion of the ACL, the center of the AHLM is very difficult to locate. Rather, surrounding anatomic landmarks can be used to locate the center of the anterior horn during lateral MAT. Urban et al 16 reported that the AHLM was located 0.48 cm lateral to the tibial midline. Johnson et al 4 reported that the insertion site of the AHLM is directly anterior to the lateral tibial spine. Arthroscopic landmarks include the anterior half of the ACL tibial insertion, the lateral tibial spine, and the articular margin of the anterolateral tibial plateau. 4 A quantitative analysis demonstrated that the center of the AHLM is located 14.4 ± 2.2 mm anteromedial to the apex of the lateral tibial eminence and 7.1 ± 1.3 mm anteromedial to the closest edge of the articular cartilage of the lateral tibial plateau. 9
Anatomic placement of the allograft is imperative for long-term survival after MAT. A clinical study demonstrated that a nonanatomic horn position increases the risk of early graft failure after lateral MAT. 9 The present study showed that the provisional wire was located within 2 mm of the anatomic center in 21 patients (23%) and within 3 mm of the anatomic center in 62 patients (67%). There is a paucity of biomechanical and clinical studies on the nonanatomic location of the meniscal insertion in the literature. A biomechanical study investigated a change in resultant tension of the medial meniscus after 3-mm nonanatomic placement of the anterior horn in porcine knees. 14 Placing the horn attachment 3 mm medial to the anatomic site decreased tension at the horn attachment by 49% to 73%. Placement 3 mm lateral to the anatomic site increased tension by 28% to 68% depending on the flexion angle and femorotibial load. 14 A nonanatomic location of the posterior horn of an implanted medial meniscal autograft adversely affects the pressure distribution on the tibial plateau in a cadaveric knee and showed a higher degree of osteoarthritic changes compared with the meniscectomy group in an ovine model. 12,17 Placement of the posterior horn of a medial meniscal autograft 5 mm medially and 5 mm posteriorly caused a significant increase in the normalized maximum pressure and a posterior shift in the centroid of the contact area at all flexion angles. 12 In an ovine model, placement of the posterior horn of the medial meniscus 10 mm posteromedial to the original position and placement of the anterior horn 8 mm anteromedial to the original position induced a higher degree of osteoarthritic changes after 6 months compared with the meniscectomy group. 17
Limitations
There were limitations to this study. First, the center of the anterior horn was determined while moving the stump of the anterior horn with forceps. The diameter of the Kirschner wire used was smaller than that of the arthroscopic probe. The directions of viewing the anterior horn during arthroscopic surgery and at the time of drilling the provisional wire were different. Therefore, the method of determining the center of the AHLM in this study did not replicate real arthroscopic surgery conditions. Second, radiological and clinical outcomes after lateral MAT according to the results of the current study were not evaluated. Third, all specimens were retrieved from Asian patients. Because ethnic differences in the anatomic insertion of the AHLM may exist, caution is required in applying our results to a non-Asian population.
Conclusion
The provisional wire was located a mean of 2.5 mm from the anatomic center, and only 23% of patients had wires that were located within 2 mm of the anatomic center. In 39% of patients, the provisional wire was drilled anterolateral to the anatomic center. This finding needs to be considered during lateral MAT.
Footnotes
Final revision submitted November 20, 2021; accepted January 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.N.V. has received hospitality payments from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Nowon Eulji Medical Center (No. EMCS 2020-07-033).