
Abstract
Background:
Previous studies have demonstrated that lateral meniscal allograft transplantation (MAT) through medial arthrotomy showed less extrusion than that of the lateral arthrotomy. However, there is a paucity of literature reporting clinical and radiological outcomes after lateral MAT through the medial arthrotomy.
Hypothesis:
Lateral MAT through a medial arthrotomy would show significantly improved clinical scores and minimal joint space narrowing compared with preoperative status.
Study Design:
Case series; Level of evidence, 4.
Methods:
Between 2001 and 2019, a retrospective chart review was conducted for all patients who underwent lateral MAT using the bony bridge technique through medial arthrotomy. Inclusion criteria were patients who underwent lateral MAT after subtotal or total meniscectomy of the lateral meniscus. A total of 27 patients who were not followed up for >4 years or had follow-up magnetic resonance imaging after surgery were excluded. At final follow-up, Lysholm scores and Tegner activity scale scores were collected. Graft extrusion, trough angle, and position of the bony bridge were measured by magnetic resonance imaging at 6 months after MAT. Joint space width (JSW) of the lateral compartment on Rosenberg view was measured and compared preoperatively and at follow-up.
Results:
A total of 28 patients were included in this study. Their mean age was 29.8 years (range, 15-48 years) with a mean follow-up of 11.4 years. Preoperative Lysholm scores and Tegner activity scale scores (66.5 ± 16.6 and 3.1 ± 1.9, respectively) significantly improved at follow-up (84.8 ± 11.1 [P < .001] and 4.4 ± 1.5 [P = .008], respectively). The JSW decreased from 6.2 ± 1.6 mm to 5.7 ± 1.4 mm (P = .014). Extrusion was 2.2 ± 1.5 mm, and trough angle was 1.5°± 8.9°. The bony bridge was positioned at 43.9% ± 4.3% from the lateral edge on the entire tibial plateau. Nine patients (32.1%) underwent subsequent procedures. Partial meniscectomies were performed in 2 patients, meniscal repairs in 2, manipulation under anesthesia in 1, and lateral capsular plication in 1. Three patients who underwent total meniscectomy or revision surgery were regarded as having a failure; therefore, 89.3% grafts survived.
Conclusion:
Lateral MAT through the medial arthrotomy demonstrated satisfactory clinical and radiological outcomes at long-term follow-up.
Meniscal allograft transplantation (MAT) is a viable treatment option for patients with meniscal deficiency. Although there is a question whether MAT can provide a chondroprotective effect, satisfactory clinical outcomes after MAT have been published extensively in the literature.14-16 Anatomical placement of the meniscal allograft is imperative to achieve satisfactory clinical outcomes. Nonanatomic horn position of the allograft increases the risk of early graft failure after MAT. 8
Lateral meniscal allograft is usually prepared using the keyhole or bony bridge technique because insertions of both anterior and posterior horns are very close. Conventionally, the lateral meniscal allograft is inserted through the lateral arthrotomy. However, drilling of a guide pin for the keyhole along the anterior and posterior horns is difficult because of a tight patellar tendon.11,17 A keyhole or bony trough may be placed laterally or obliquely. Inaccurate placement of the allograft is an important etiology of postoperative extrusion.6,10,11 Therefore, the transpatellar tendon approach and medial arthrotomy have been tried during lateral MAT to drill the guide pin accurately along the anterior and posterior horns.4,17 However, there is a paucity of literature reporting clinical and radiological outcomes after lateral MAT through the medial arthrotomy. Therefore, the purpose of this study was to report clinical scores and joint space narrowing after lateral MAT through a medial arthrotomy. It was hypothesized that lateral MAT through a medial arthrotomy would show significantly improved clinical scores and minimal joint space narrowing compared with preoperative status.
Methods
Participants
All patients provided written informed consent. This retrospective study protocol was reviewed and approved by our institutional review board. Between January 2001 and December 2019, 55 lateral MATs were performed using a fresh-frozen graft by a single surgeon (N.H.C.) in a single center. Inclusion criteria were patients who underwent lateral MAT after subtotal or total meniscectomy of the lateral meniscus. They had no valgus malalignment >3°, which was confirmed using a long-leg standing radiograph. They had no diffuse grade 3 chondromalacia on the lateral compartment as rated by Outerbridge classification. The patients requiring ligament reconstructions or cartilage procedures for focal chondral lesions were included in this study. Exclusion criteria were patients with untreated ligamentous instability or age >50 years. The patients who were not followed up for >4 years or had a follow-up magnetic resonance imaging (MRI) after surgery were excluded. Thirteen patients did not undergo follow-up MRI. Eleven patients were followed <4 years after surgery. In 3 patients, the medial or lateral edge of the bony bridge was not clearly delineated. The trough angle and position of the bony trough were not measured accurately. These 3 patients were excluded.
Surgical Procedure
The meniscal allograft was sized based on coronal MRI measurements. 7 The fresh-frozen meniscal allograft was prepared utilizing a bony bridge with a width of 9 mm. The recipient meniscus was debrided using a motorized shaver to expose the meniscocapsular junction of the posterior horn and midbody. A miniarthrotomy along the medial border of the patellar tendon was performed. The infrapatellar fat pad was excised and the anterior horn of the recipient meniscus was excised. A bony trough with a width of 9 mm was made just lateral to the anterior cruciate ligament (ACL) insertion on the tibia along the line between the anterior and posterior horns of the lateral meniscus (Figure 1). The bony bridge of the allograft was inserted into the bony trough (Figure 2), and arthroscopy was used to confirm the correct position of the meniscal allograft. Meniscal repairs were performed using the outside-in technique for the anterior horn and inside-out technique for the midbody and posterior horn (Figure 3).
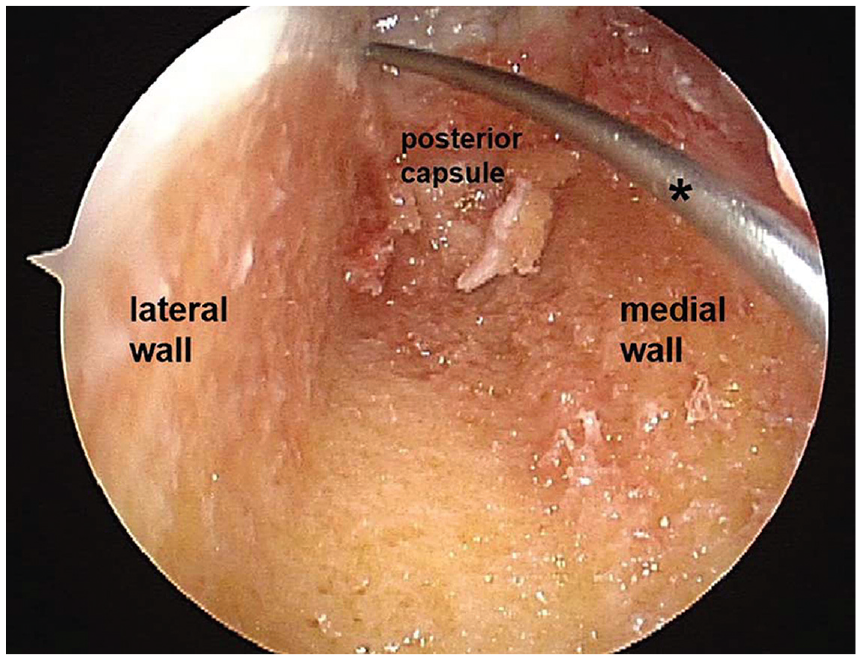
Prepared bony trough in the right knee. The posterior cortex was removed and the posterior capsule was shown. During graft preparation, an absorbable suture was placed at the posterior horn for later pulling of the graft into the lateral compartment. A flexible wire with eyelet (asterisk) was used to pull each limb of the absorbable suture as the inside-out meniscal repair technique.
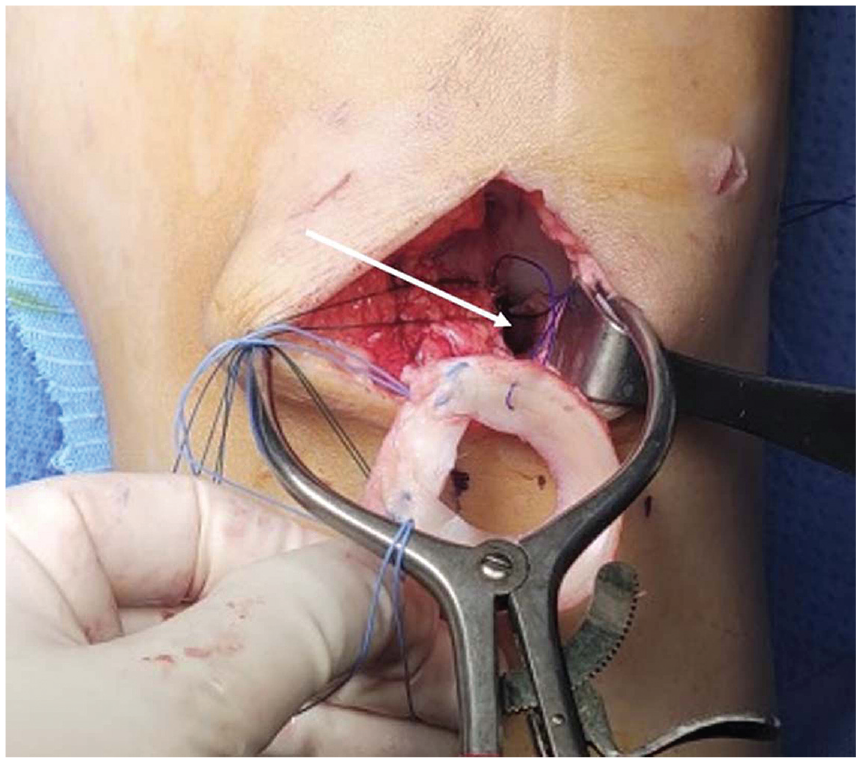
Insertion of the allograft into the prepared bony trough (white arrow) through the medial arthrotomy in a left knee. Nonabsorbable sutures were placed at both anterior and posterior horn insertions.

Transplanted lateral meniscus in the right knee.
Postoperatively, partial weightbearing was permitted as soon as tolerated. Closed kinetic chain and quadriceps strengthening exercises were started as early as possible. Full weightbearing was allowed after 6 weeks and squatting after 12 weeks. Jogging began after 4 to 5 months. Return to sports was allowed after 6 to 8 months. At final follow-up, Lysholm scores and Tegner activity scale scores were evaluated by an orthopaedic resident (D.-K.K.) who was not involved in the surgical procedure.
Postoperative Radiologic Evaluation
Joint space widths (JSWs) on the Rosenberg view were measured between the tibial and femoral surfaces at the midpoints of the lines depicting the lateral compartment preoperatively and at final follow-up. 13 MRI at 6 months after MAT was routinely recommended to evaluate extrusion on a coronal plane and position of the allograft on an axial plane. On the coronal view showing the maximum extrusion of the midbody, extrusion was measured as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the allograft (Figure 4). 4 On the axial view showing the bony bridge clearly, a longitudinal line (line B) of the bony bridge was drawn. A tangential line was drawn between the medial and lateral posterior tibial condylar cortices. Another line (A) perpendicular to the posterior tangential line was drawn. The angle (trough angle) between line A and line B was measured (Figure 5). 11 If line B was rotated externally to line A, the trough angle was designated positive. If line B was rotated internally, the trough angle was designated negative. 11 On the same axial view, the distance between the medial and lateral edges of the entire tibial plateau (DT) was measured. The distance between the outer edge of the lateral tibial plateau and the center of the bony bridge (DB) was measured. DB divided by DT was regarded as the position of the bony bridge on the axial plane (Figure 6).4,6 All measurements were performed by 2 orthopaedic residents (including D.K.K.). They repeated all measurements 4 weeks later to calculate the intraobserver and interobserver reliability.

On the coronal view, extrusion (asterisk) was measured as the distance between the outer edge of the (A) articular cartilage of the lateral tibial plateau and (B) the outer edge of the meniscal allograft.

View of the right knee on axial magnetic resonance imaging. The (B) white dotted line is the longitudinal axis of the bony bridge, and the (C) line is the posterior tibial condylar tangential line. The (A) line was drawn perpendicular to the (C) line. The trough angle (asterisk) between the (A) line and the (B) dotted line was measured.
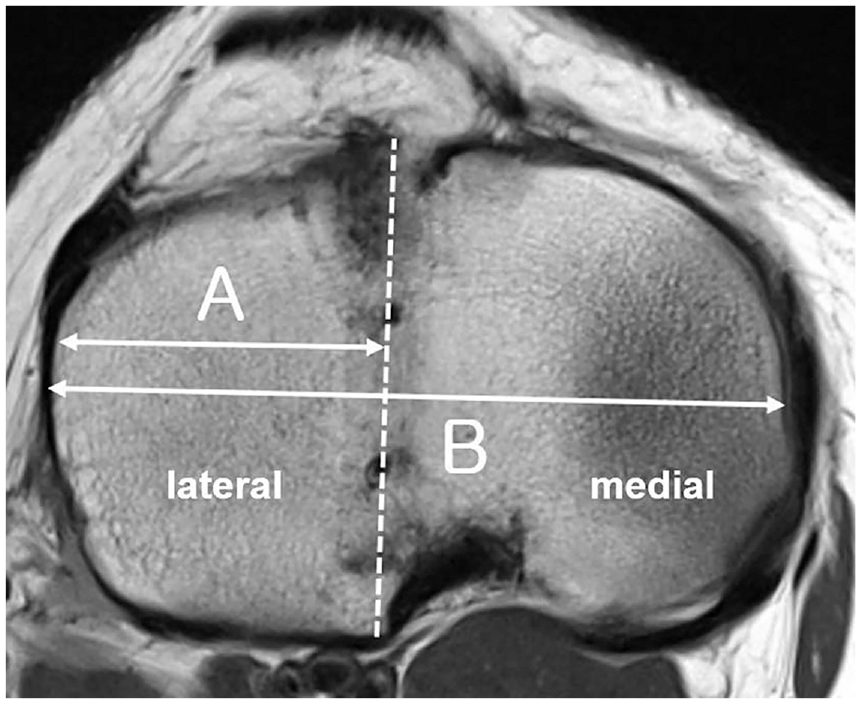
On the axial view, the (A) distance between the outer edge of the lateral tibial plateau and center of the bony bridge and the (B) distance between the medial and lateral edges of entire tibial plateau were measured.
Statistical Analysis
A paired t test and Wilcoxon signed-rank test were used to compare preoperative and follow-up values of Lysholm scores, Tegner activity scale scores, and JSW. A Pearson correlation test was performed between measured radiologic parameters and Lysholm/Tegner scores. Analysis was performed using SPSS software (SPSS Statistics 25.0; IBM) and significance was assumed at a P value of <.05.
Results
A total of 28 patients were included in this study. There were 18 male and 10 female patients. Mean age at time of the lateral meniscal tear was 29.8 years ± 9.5 years (range, 15-48 years). Two microfractures, 1 osteochondral autograft transfer, and 1 ACL revision with medial collateral ligament reconstruction were performed concomitantly at the time of lateral MAT. Mean follow-up was 137.1 ± 43.9 months. Lysholm score improved significantly at follow-up (66.5 ± 16.6 vs 84.8 ± 11.1; P < .001). Tegner activity scale scores improved significantly at follow-up (3.1 ± 1.9 vs 4.4 ± 1.5; P = .008). JSW decreased significantly at follow-up (6.2 ± 1.6 mm vs 5.7 ± 1.4 mm; P = .014). At postoperative 6 months, extrusion was 2.2 ± 1.5 mm, trough angle was 1.5°± 8.9°, and DB/DT was 43.9% ± 4.3%. Intra- and interobserver reliability for the trough angle, DB/DT, and JSW is described in Table 1. Measured radiologic parameters did not correlate with Lysholm scores or Tegner activity scale scores.
Intra- and Interobserver Reliability for Measured Radiologic Parameters a

DB, distance between the outer edge of the lateral tibial plateau and the center of the bony bridge; DT, distance between the medial and lateral edges of the entire tibial plateau; ICC, intraclass correlation coefficient; JSW, joint space width.
Subsequent Surgeries
Nine patients (32.1%) underwent subsequent procedures. Partial meniscectomies were performed in 2 patients, meniscal repairs in 2, and total meniscectomy in 2. Manipulation under anesthesia was performed in 1 patient, lateral capsular placation in 1, and revision lateral MAT in 1. The 3 patients who underwent total meniscectomy or revision surgery were regarded as having a failure. Therefore, 89.3% of grafts survived at mean 11.4 years after lateral MAT. A 36-year-old female patient underwent total meniscectomy for full-thickness radial tear of the graft. A 48-year-old female patient underwent total meniscectomy for a bucket-handle tear of the graft. A 28-year-old male patient demonstrated a bucket-handle tear of the graft at 14 years after MAT. His graft was removed and revision of the lateral meniscal tear was performed.
Discussion
The most important finding of this study was that clinical outcomes improved significantly after lateral MAT through a medial arthrotomy at long-term follow-up. Although 32.1% of patients underwent subsequent procedures, 89.3% of grafts survived. Mean JSW at long-term follow-up decreased slightly, and meniscal allografts were placed accurately on the axial and coronal plane.
Anatomical placement of the lateral meniscal allograft is imperative to long-term survival. Kim et al 8 reported that the failure rate within 1 year after surgery was 11.1% in the nonanatomic horn position group (nonanatomic group) and 3.1% in the anatomic horn position group (anatomic group). They defined the failure as grade 3 signal intensities over one-third of the allograft on follow-up MRI or removal of more than one-third of the allograft. The nonanatomic group had an increased risk (odds ratio, 3.88) of early graft failure as compared with the anatomic group. Grafts of the nonanatomic group were positioned more anteriorly and laterally than the anatomic group.
Laterally placed lateral meniscal allograft on the coronal plane is a major cause of extrusion. Previous studies have investigated the relationship between the amount of extrusion and ratio of distance of the bony bridge to the entire tibial plateau. 6 There was significantly less extrusion in patients whose meniscal transplants were positioned with a ratio of DB to DT >40%. The cutoff point above which 3-mm extrusion did not occur was 42%. These findings suggest that closer positioning of the center of the bony trough to the center of the entire tibial plateau width results in less extrusion. 6 Lateral meniscal allograft may be placed nonanatomically on the sagittal plane. Because the insertion of the posterior horn of the lateral meniscus is close to the popliteal artery, incomplete osteotomy of the posterior cortex may occur, resulting in the meniscal allograft’s being positioned more anteriorly than anatomically. Lee et al 10 found that the anterior horn was placed more anteriorly to the anterior tibial margin in the MAT group than in the control group. The posterior horn of the allograft was placed more anteriorly to the posterior tibial margin than in the control group. More anteriorly placed meniscal allograft was associated with greater degree of extrusion. 10
A guide pin is inserted during preparation of the keyhole for the meniscal allograft. 12 Direction of this guide pin on sagittal and coronal planes can be decided under the fluoroscopic control. The guide pin is usually drilled along the lateral tibial spine where both the anterior and the posterior horns are inserted. However, a study using a resected tibial plateau during knee arthroplasty demonstrated that 75% of guide pins drilled along the lateral tibial spine were internally rotated to the longitudinal line along the centers of the anterior and posterior horns of the lateral meniscus. The axis of the lateral tibial spine was not a reliable marker for the bony trough in the lateral MAT. 5 Therefore, the keyhole or bony trough of the allograft may be placed obliquely on the axial plane. Oblique placement of the allograft is a cause of postoperative extrusion. Lee et al 11 measured the axial trough angle between a tangential line along the posterior tibial condyle and a longitudinal line along the center of the bony trough of the allograft. As the axial trough was more externally rotated, the graft became more extruded. The cutoff value of the axial trough angle was 5.6°.
The patellar tendon is a significant obstacle in lateral MAT. The anterior horn of the lateral meniscus inserts immediately posterior to the patellar tendon. Lee et al 11 stated that the guide pin through a lateral parapatellar approach was drilled at a more lateral position than the insertion of the anterior horn of the lateral meniscus because of the tight patellar tendon. They recommended maintenance of knee extension to relieve tension of the patellar tendon during drilling of the guide pin. Yoon et al 17 reported that the insertion point of the guide pin was slightly medial to the center of the tibial tuberosity to place the lateral meniscal allograft anatomically. Correct direction of the guide pin was possible through the patellar tendon. They suggested knee extension at the time of guide pin drilling to minimize injury of the patellar tendon and to retract the patellar tendon more easily. The medial parapatellar approach rather than conventional lateral approach may be an alternative to place the lateral meniscal allograft more easily. 4
Clinical outcomes after lateral MAT through medial arthrotomy at long-term follow-up are comparable with those reported in the literature. In this current study, the mean Lysholm score was 84.8 and mean Tegner activity scale score was 4.4 at mean 11.4 years follow-up. The JSW of the lateral compartment decreased <1 mm. A long-term follow-up study 14 reported that the mean Lysholm score was 86.9 ± 10.9 at the 5-year follow-up and 77.4 ± 11.5 at the 15-year follow-up. The JSW remained unchanged until the 5-year follow-up (3.1 ± 1.7 mm). However, this JSW decreased to 1.9 ± 1.4 mm at the 15-year follow-up. Another study 3 reported that 9 of 13 athletes (69%) returned to sports at the same preinjury level. The mean Lysholm score was 72 ± 15 after MAT at a mean 9-year follow-up. In a recent systematic review, 1 6 studies reported that mean differences between preoperative and postoperative Tegner activity scale scores ranged from −3 to 2. The mean reoperation rate after MAT was 33% (range, 3.1%-80%), whereas the mean failure rate including both clinical failure and surgical failure was 16%. 1 Reoperation rate (32.1%) and failure rate (10.7%) of this current study showed similar results.
Comparison of clinical outcomes between the medial and lateral arthrotomies is rarely reported in the literature. A previous study 4 reported that lateral MAT through medial arthrotomy demonstrated less extrusion than that of the lateral arthrotomy. Seven (21.9%) patients demonstrated extrusion in the medial arthrotomy group, and 15 (65.2%) patients had extrusion in the lateral group (P = .002). The median trough angle was 0.9° (range, –8.8° to 15.8°) in the medial arthrotomy group and 11.6° (range, 3° to 19.8°) in the lateral arthrotomy group (P < .001). 4 The mean extrusion of 2.2 ± 1.5 mm and mean trough angle of 1.5°± 8.9° in this current study were less than those reported in previous studies using conventional lateral arthrotomy. Ahn et al 2 reported the mean trough angle was 5.0°± 2.8° and mean extrusion was 4.4 ± 0.8 mm in a major extrusion group. Lee et al 11 reported the mean trough angle was 7.3°± 4.3° and mean extrusion was 3.1 ± 1.2 mm in the major extrusion group.
Limitations
Several limitations of this study must be acknowledged. First was our relatively small sample size. Many patients with insufficient follow-up or absence of follow-up MRI were excluded. They could affect the results of this study. Second, there was no control group whose allografts were transplanted through the lateral arthrotomy. Third, follow-up MRI was performed 6 months after surgery. Although the positions of the bony trough and trough angles would not change, the extrusion may increase as time passes. However, a study reported that meniscal extrusion did not progress during the midterm follow-up after lateral MAT. 9 Therefore, meniscal extrusion at 6 months after surgery may be correlated with clinical outcomes in the long term.
Conclusion
Lateral MAT through the medial arthrotomy demonstrated satisfactory clinical and radiological outcomes at long-term follow-up.
Footnotes
Final revision submitted June 22, 2024; accepted July 15, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Eulji University (EMCS 2022-05-010).