
Abstract
Background:
Previous studies have suggested that suture tape-reinforced anterior cruciate ligament (ACL) grafts may have higher ultimate failure loads without stress-shielding. In patients at high risk for graft failure, such as adolescents, the addition of suture tape could have beneficial outcomes.
Hypothesis:
Suture tape reinforcement (STR) of ACL grafts in adolescent patients would lead to fewer graft ruptures during early recovery, without hindering subjective outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was performed on adolescent patients with a minimum 2-year follow-up after hamstring tendon autograft ACL reconstruction; enrolled were patients from both before (n = 40) and after (n = 40) a shift in surgical technique that added STR. Both the no-STR and the STR cohorts were contacted yearly to obtain patient-reported outcome data for visual analog scale (VAS; range, 0-10) for pain score, Single Assessment Numeric Evaluation, Lysholm score, Tegner activity score, patient satisfaction score (range, 0-100), and return to previous level of sport (yes/no). The cohorts were then matched based on follow-up duration, excluding those with follow-up of <2 years and >3 years to maintain consistency in duration of follow-up. Graft failure was defined as either graft rupture or recurrent instability symptoms, and failures occurring from index procedure to the 3-year mark were recorded for calculations of failure rate.
Results:
There were no differences between cohorts in mean age [STR, 15.7 years (range, 9.5-18.7 years); no STR, 14.9 years (range, 9.3-18.8 years)], follow-up duration, laterality, or graft size. While not statistically significant, 2 (5%) patients in the STR cohort experienced graft rupture compared with 7 (17.5%) patients in the no-STR cohort. The Tegner score was significantly higher in the STR cohort (P = .017); no between-group differences were seen on the other outcome scores. A subanalysis of the STR cohort comparing small-diameter grafts (<8 mm) with grafts ≥8 mm also demonstrated no difference in outcome measures, with 1 graft failure in each cohort.
Conclusion:
Study outcomes indicated that patients treated with ACL reconstruction and STR experienced a significant improvement in Tegner scores while at the same time maintaining the other subjective outcomes.
Despite best efforts, anterior cruciate ligament (ACL) injuries remain challenging to treat in the adolescent population in whom graft failure rates remain high relative to adult counterparts. 33 Many of the challenges faced in treating young athletes are nonmodifiable, as research has demonstrated that younger age, associated injury, and smaller graft size are independent risk factors for ACL graft failure. 3,15,18,19,31,33 Much of the research focus has been placed on determining the best graft choice for these patients. The most recent data from large American and Scandinavian registries consisting of thousands of patients have shown that, compared with bone-patellar tendon-bone graft (BTB), hamstring tendon grafts are more likely to require a revision surgery, with a relative risk ratio ranging from 1.4 to 2.3. 9,25,27 However, when selecting a graft for adolescent athletes, the lower failure rate of BTB grafts must be weighed against their potential drawbacks, including the risk of anterior knee pain, a less cosmetic incision, greater postoperative pain and stiffness, and potential growth disturbance associated with open physes, if present. 7
Efforts to enhance the durability of soft tissue autografts, particularly those of smaller diameter, have focused on various augmentation and reinforcement techniques. Augmentation is used here to describe the technique of creating a larger diameter graft, and reinforcement is used to describe the technique of strengthening a construct without necessarily making the graft a larger diameter. Reports of hybrid grafts using allograft tissue to augment autograft tissue have yielded equivocal results at best, with some concern for even higher rates of failure. 10,32 A recent study by Ebert and Annear evaluated the efficacy of the Ligament Augmentation and Reconstruction System in patients with hamstring tendon autografts that combines the idea of augmentation and reinforcement. 6 They reported good clinical scores, a high rate of return to sports, and low rates of secondary ruptures and contralateral ACL tears at 2 years. 6
Smith and Bley recently described a technique that utilized suture tape to primarily reinforce allograft ACL reconstructions. 30 A follow-up biomechanics study showed that a suture tape placed as reinforcement to the ACL reconstruction ex vivo provided higher ultimate failure loads without stress-shielding in small and standard diameter grafts. 2 These results are encouraging for the use of graft reinforcement constructs in adolescent patients, in whom soft tissue graft size is often a limiting factor and failure rates are generally higher. 3,18,19,31,33
There is lack of literature regarding the use of suture tape for the reinforcement of ACL hamstring tendon autografts. Accounting for the fact that hamstring tendon autografts tend to fail early in adolescent patients, with a mean time to failure reported at <12 months and nearly all failures captured by 24 months, 10 we sought to assess the utility of suture tape ACL reinforcement as a technique to prevent early failures. Our primary aim was to assess failures of adolescent ACL reconstruction grafts with suture tape reinforcement (STR) and to determine if there was any detriment to patient-reported outcomes. A secondary aim was to evaluate if the risk of failure of small graft diameter could be negated using the reinforcement technique. Our hypothesis was that reinforcing hamstring tendon autografts with a suture tape in adolescent patients would result in similar subjective outcomes, but fewer graft ruptures compared to a matched cohort of patients undergoing the same procedure without the suture tape reinforcement.
Methods
After receiving institutional review board approval, we retrospectively enrolled all patients undergoing ACL reconstruction since 2012 at our institution for chart review. As part of our clinical practice, patients are contacted on a yearly basis to obtain and record their subjective outcomes, but they are not seen in person (if doing well) after the 1-year visit. Included were patients with ACL rupture requiring reconstruction who underwent hamstring tendon autograft and were aged ≤ 19 years old. Exclusion criteria consisted of multiligamentous knee injury requiring surgical intervention of the collateral ligaments or the posterior cruciate ligament, previous ACL injury requiring surgical intervention of the ipsilateral knee, or graft selection other than isolated hamstring tendon autograft. Associated pathology, including cartilage injuries and meniscal injuries, did not serve as exclusion criteria, and therefore patients with these concomitant injuries were included.
Surgical Technique
Starting February 2018, 1 of the authors (E.W.E.) converted the hamstring tendon autograft reconstruction technique to include suture tape reinforcement (STR) using FiberTape (Arthrex). Therefore, 2 cohorts were created: hamstring tendon autograft with no STR (no-STR cohort) and hamstring tendon autograft with STR (STR cohort). To better create matching cohorts regarding follow-up period, we included only the data collected on each patient during the postoperative second and third years (inclusive of the entire 36 months) of follow-up for comparison. This was done to reduce confounding the graft failure results and outcome scores with retired athletes (given the adolescent age group), even if longer-term data were available.
No other changes to surgical technique, bracing protocol, or rehabilitation protocol were made over the study duration other than the technical advancement/changes related to tunnel creation (eg, FlipCutter I to FlipCutter II [Arthrex] changes). Hamstring harvest involved both the gracilis and the semitendinosus tendons, which were taken via closed tendon stripper after releasing the tendons from the tibial insertion and securing them via a looped suture on their distal ends. The autografts were then taken to the back table, debrided of excess muscular tissue, tubularized, and secured on a graft board under tension. The proximal end was then secured using No. 2 braided nonabsorbable suture (Tevedek II, Teleflex Medical OEM). Both grafts were then secured to an adjustable loop fixation device, the ACL TightRope (Arthrex), with the length of the graft optimized, and the limbs were then secured to each other via an absorbable braided No. 2-0 suture to prevent slippage around the loop in a 4-strand construct (regardless of the graft size). For the no-STR cohort, the graft was then sized and placed under a saline soaked sponge until the knee was ready for introduction of the graft.
For the STR cohort, the construct was created by sliding a suture tape through the eyelets of the button of the suspensory construct (Figure 1). Once in place, the graft and suture tape construct was then sized and placed under a saline-soaked sponge until the knee was ready for introduction of the graft. The femoral socket was created using an outside-in approach via a FlipCutter device (Arthrex), and the tibial tunnel was created via a guide-pin and acorn reamer. Once the tunnels were prepared, the graft in both cohorts was seated into the femoral tunnel, and the button was secured against the lateral cortex. Attention was then directed to the tibial fixation. In the STR cohort, the slack was removed from the suture tape, confirming that the button was well seated on the cortex. Tension was then placed on the graft (in both cohorts), and in the STR cohort, the suture tape was pulled in a manner to just remove the slack but without applying tension on the suture tape. This was done so that the suture tape would not over constrain the joint or stress-shield the autograft. The knee was then cycled, maintaining tension on the autograft portion of the construct, with the knee held at 25° to 30° of flexion, and interference screw placement then completed the reconstruction. After screw fixation, the 2 limbs of the suture tape were then tied together to create a knot on the outer cortex of the screw, and the sutures creating the adjustable loop on the femoral side were also knotted to reduce risk of slippage. Figures 2 demonstrates the appearance of the autograft with and without suture tape inclusion after fixation of the graft in the knee. Figure 3 demonstrates the orientation and inclusion of the suture tape in the autograft and origin/insertion sites.

Incorporation of the suture tape onto the ACL TightRope (Arthrex) button. (A) One limb placed first through the eyelet with the lead suture. (B) Second limb placed through the other eyelet. (C) Completed construct of STR with lead suture; Tightrope tightening sutures lie to the right, and suture tape and Tightrope loop lie to the left. Asterisk, pull suture; white arrow, STR; black arrow, adjustable loop suture. ACL, anterior cruciate ligament; STR, suture tape reinforcement.

In vivo arthroscopic images of the incorporated hamstring tendon autograft (A) with no STR and (B) with STR. STR, suture tape reinforcement.

Line drawing demonstrating the orientation and inclusion of the suture tape reinforcement within the autograft and origin/insertion sites.
Postoperative Care
Postoperative care consisted of approximately 6 weeks of full weightbearing in a range of motion brace. Restrictions to range of motion were related to meniscal repair, not flexing past 90° during this first phase but continued weightbearing as tolerated in a locked brace. When patients could perform an intact straight-leg raise, they transitioned to wearing a knee sleeve, which they maintain for the first 12 months postoperatively to assist with proprioception. Physical therapy was started within the first 1 to 2 weeks and continued for a minimum of 6 months, dependent on the patient passing an objective clearance test to evaluate neuromuscular control, such as proprioception and functional strength.
Data Collection
Descriptive data collected included sex, laterality, sport played, time from injury to magnetic resonance imaging, and time from injury to surgery. All patients underwent plain radiographs and magnetic resonance imaging of the injured knee before surgery. Graft type and size were collected from operative notes. Graft failure was defined as either graft rupture or recurrent instability symptoms, as reported by the patient or during an in-person visit, if available. The graft failures occurring during the study period and those that occurred before 2 years of follow-up were included for statistical analysis of an inclusive failure rate. The following patient-reported outcome scores were collected: visual analog scale (VAS; range 0-10) for pain score, Single Assessment Numeric Evaluation (SANE), Lysholm score, Tegner activity score, and patient satisfaction score (range, 0-100). In addition, patients were queried on whether they were able to return to their previous level of sport.
Graft size was compared as a continuous interval variable and secondarily grouped into a dichotomous variable to examine small diameter graft sizes (<8 mm) to those larger in diameter (≥8 mm), based on previous literature cutoffs. 3,18,19,31,33 This was done to determine whether graft size would ultimately influence outcomes despite the utilization of the STR or whether there would be a deleterious effect of reinforcing these smaller grafts with the STR.
Statistical Analysis
Variables were assessed for normality via numerical and graphical methods. Shapiro-Wilk test confirmed data were not distributed normally, and nonparametric analyses were used. Continuous variables were compared using the Mann-Whitney U test. Categorical variables were compared between groups using the chi-square test. Analyses were performed using SPSS for Windows Version 26 (IBM Corp), and alpha was set to P < .05 to declare significance.
Results
Patient Characteristics
A total of 64 patients underwent ACL reconstruction with STR, and 40 (62.5%) had a minimum of 2-year follow-up at the time of study. The no-STR cohort initially had 83 patients who met criteria with complete datasets during the desired timeframe. After criteria were applied and then follow-up range was matched, the 2 cohorts each consisted of 40 adolescents (Figure 4). The characteristics of each group are summarized in Table 1. When comparing patients with no STR with those with STR, we observed no significant differences on any characteristic.

Flowchart detailing the inclusion and exclusion of patients. ACL, anterior cruciate ligament; BTB, bone-patellar tendon-bone graft; Quad, quadriceps tendon graft; ITB, iliotibial band graft; STR, suture tape reinforcement.
Characteristics of the Study Groups a
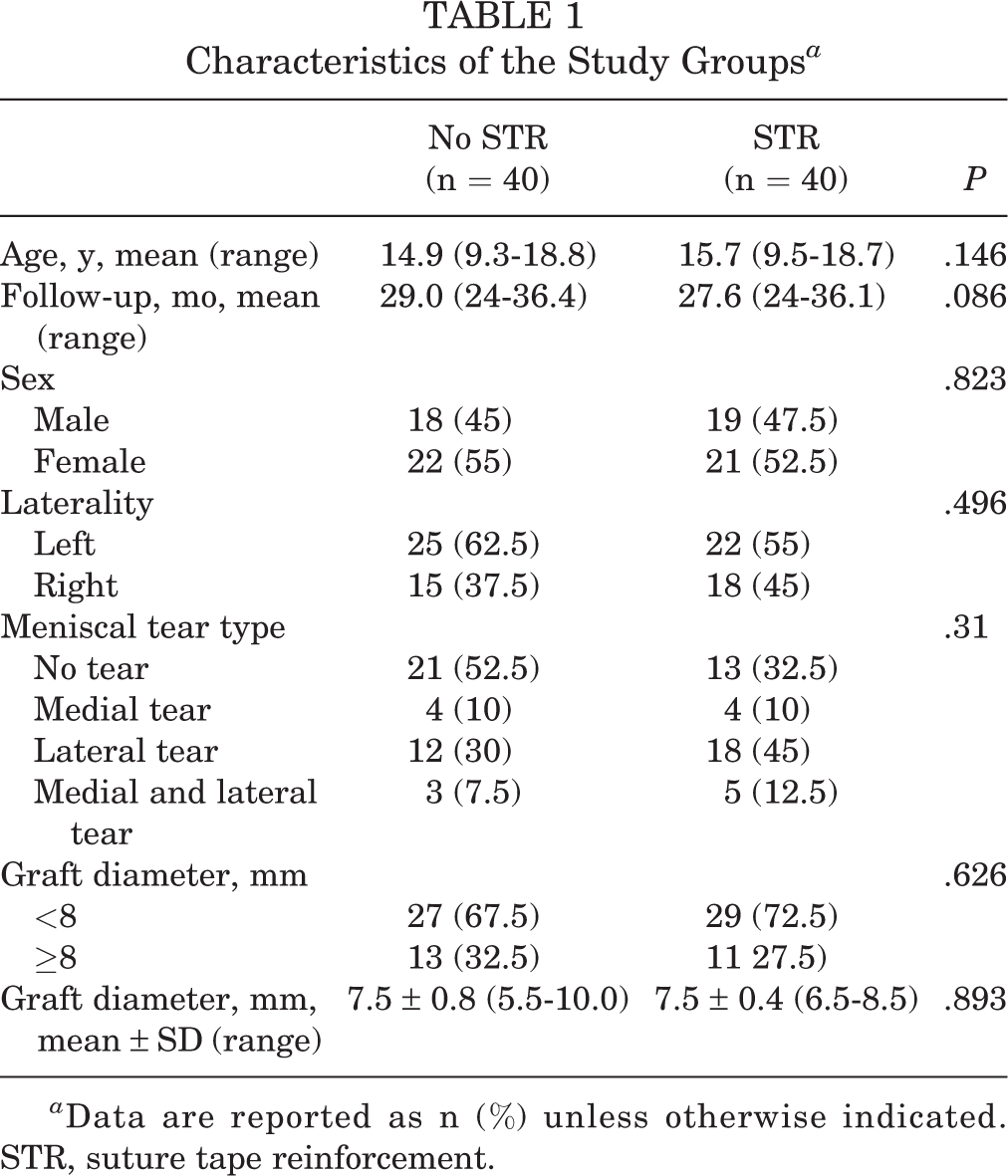
a Data are reported as n (%) unless otherwise indicated. STR, suture tape reinforcement.
Comparison of Outcomes
Subjective outcomes were similar in patients with STR and with no STR in all categories except for the Tegner activity score. Compared with patients without an STR, those with STR reported an increased mean of 1 point in Tegner activity scores (6.3 vs 7.4; P = .017). Ability to return to sports was also similar between the 2 cohorts (51.5% vs 69.2%; P = .124). At 2 years postoperatively, 2 (5%) patients with STR experienced graft failure compared with 7 (17.5%) patients with no STR (P = .077). Three additional patients with STR required reoperation, 2 for a medial meniscal tear and 1 for a painful implant, yielding a total reoperation rate of 12.5%. One patient with STR experienced a superficial infection that treated was successfully with oral antibiotics. Excluding reoperation for contralateral ACL tear, the no-STR cohort also had 2 additional surgeries for meniscal repairs, yielding a total reoperation rate of 22.5%. Outcome differences between no-STR and STR cohorts are summarized in Table 2.
Comparison of Outcomes Between the Study Groups a

a Data are reported as mean ± SD or n (%). Bold value indicates statistically significant difference between groups (P < .05). RTS, return to previous level of sports; SANE, self-assessment numerical evaluation; STR, suture tape reinforcement; VAS, visual analog scale.
b n = 33 for no-STR group; n = 38 for STR group.
c n = 33 for no-STR group; n = 39 for STR group.
Graft Diameter
Further analysis of the STR cohort demonstrated that 29 (72.5%) patients received a graft <8 mm and 11 (27.5%) patients received a graft ≥8 mm. There were no significant differences on any outcome score between graft sizes (Table 3), but only 9 patients had complete outcome score data; whereas, 10 total had complete return sport data and all 11 in that cohort had graft failure data. There was 1 failure (3%) in the <8 mm group and 1 failure (9.1%) in the ≥8 mm group (P = .465). In a subgroup analysis of patients with graft <8 mm, we found no significant difference in failure rates when comparing patients with STR and with no STR (Table 4).
Comparison of Outcomes in Patients With STR With Small Diameter (<8 mm) Versus Normal Diameter (≥8 mm) Grafts a
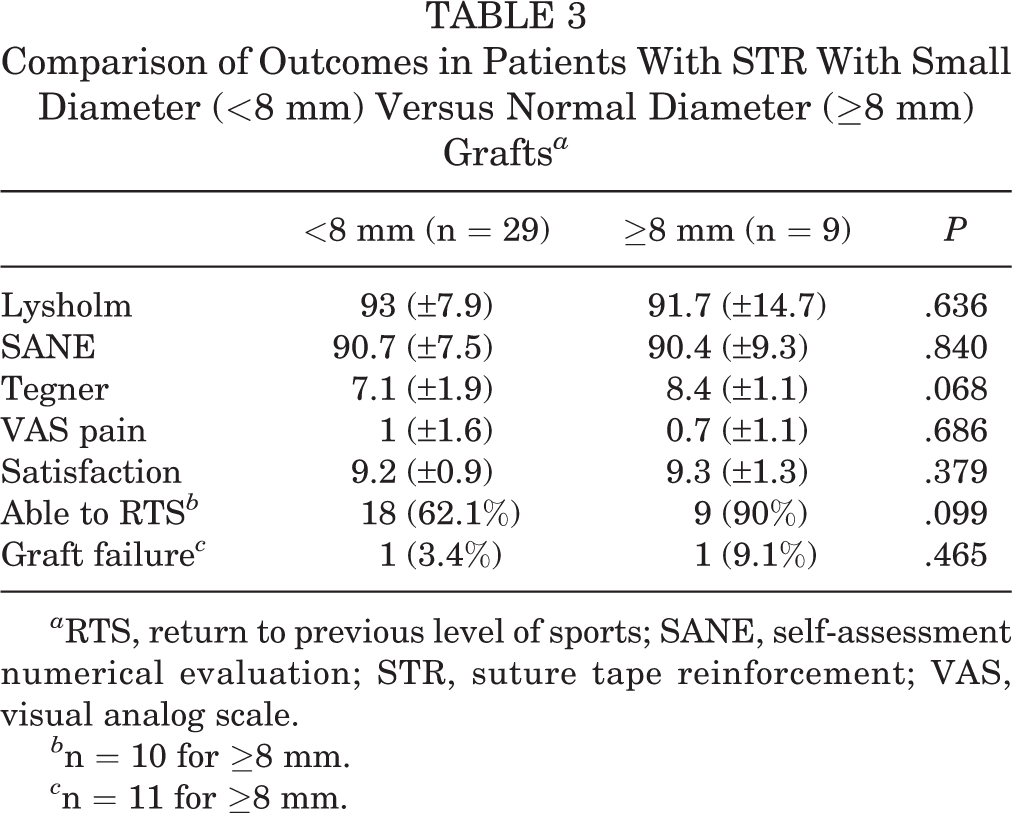
a RTS, return to previous level of sports; SANE, self-assessment numerical evaluation; STR, suture tape reinforcement; VAS, visual analog scale.
b n = 10 for ≥8 mm.
c n = 11 for ≥8 mm.
Comparison of Outcomes in Patients With Small Diameter (<8 mm) Grafts With STR and With No STR a

a RTS, return to previous level of sports; SANE, self-assessment numerical evaluation; STR, suture tape reinforcement; VAS, visual analog scale.
b n = 25 (1 patient with graft failure did not provide subjective outcome data).
Discussion
In our study, STR was associated with similar (to improved) subjective outcomes scores and a lower rate of early graft failure that did not reach statistical significance. Discovery of effective methods of graft reinforcement is potentially critical in improving patient outcomes after ACL reconstruction given the high graft failure rates, smaller average graft diameter, and the constraints on native anatomy (potential open physes) in adolescent patients. 3,10,19 Our hypothesis was partially upheld in that we did see similar patient-reported outcome measures among those with STR and with no STR. Yet, the results of our primary aim to see an improvement in early graft failure rates did not meet statistical significance.
Knee ligament reconstruction with STR has been described for use in all knee ligaments, including the ACL, posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, anterolateral ligament, and patellofemoral ligaments. 16 Suture tape as a reinforcement construct has also been described as a supplement in reconstruction of the deltoid ligament of the ankle and in upper limb ligaments, including the acromioclavicular joint and anteromedial bundle of the ulnar collateral ligaments. 13,16,20,24 However, there is a paucity of literature describing outcomes after STR in ACL reconstructions, and modern techniques without STR still result in high revision rates and inconsistent return to play, especially in a younger population. 34 In this high-risk population, ACL graft rupture can be seen in 16% to 18% of patients in short-term follow-up, with almost 50% of failures occurring in the first year and almost 75% of failures in the first 2 years. 34 This trend for early failures was recently confirmed in a large retrospective review of 561 ACL reconstructions in children and adolescents, which found that hamstring tendon autografts failed at a mean of 11 months. 10
Therefore, our primary aim was to determine if STR would lead to a decreased rate of graft failure before 3 years of follow-up. Compared with the literature, our no-STR cohort had a comparable failure rate for hamstring tendon autografts with 7 (17.5%) patients experiencing ACL graft rupture. Only 2 patients (5%) with STR experienced graft failure during this early follow-up time frame. One STR failure occurred 8.5 months postoperatively while the patient was participating in soccer before surgeon and physical therapist clearance, and the other patient experienced graft rupture at 24 months and did not disclose the mechanism of injury or participate in providing patient-reported outcome measures. The grafts of 7 patients with no STR failed at a mean of 20 months. All had been cleared for full activity. Three sustained a graft rupture from a fall/jump from a rock-climbing wall, high jump competition, or staircase. The other 4 sustained injury during competition play (2 during basketball and 2 during soccer). A power analysis, based on the observed 12.5% difference in early failure, suggests that we would need 100 patients in each cohort to identify a significance of .05 with a probability of 80% during this early follow-up period. Our study was not designed to capture this number of patients; however, with a difference in 2-year failure between groups at 12%, it does appear to be feasible to design a prospective study to answer this question.
Previous work has reported reoperation rates in adolescent patients with ACL reconstruction ranging from 13% to 24%, when using a minimum of 2-year follow-up. 22,28 Soft tissue grafts are known to undergo several phases of healing in the intra-articular graft region and at the site of graft-to-bone incorporation. 14,29 This predisposes grafts to failure during the early period of recovery. 8,26 Therefore, the intent of the STR is to protect against early failures, acting as a nonbiologic checkrein until the hamstring tendon autograft has had time to incorporate and fully undergo ligamentization. This process is believed to occur in the first 12 months and is defined by even distribution of vascularity and maximization of mechanical structural properties. 5,12,23 However, it is further understood that, even though these properties are maximized at 12 months, no studies have demonstrated a return to native ACL mechanical values and that a clear endpoint to ligamentization has not yet been defined. Nagelli and Hewett 21 have even argued that most patients with ACL reconstruction would benefit from a 2-year wait before return to sports, although they noted that the first postreconstruction year remains the most tenuous. Our study design included patient follow-up data from 24 to 36 months, which we believe was sufficient time to allow for graft incorporation and healing and to provide accurate outcome scores. If the adolescent athlete can get safely past the 2-year mark without failure, then it appears that the overall odds of long-term success are improved. Continued study on the STR construct appears to be appropriate given the outcomes noted in the present study.
One concern about using a suture tape to reinforce the ACL reconstruction is that other outcomes besides graft failure could be affected, as previously unknown complications are created. For example, detractors have argued that STR may result in the graft not seeing peak forces leading to stress-shielding. 1 Nevertheless, its use has been studied in canines and prevented early failure, while allowing complete graft to bone healing and functional graft remodeling. 4 Moreover, as anticipated, the current study found that Lysholm scores, SANE scores, pain scores, satisfaction scores, and return to sports were similar among those with STR and with no STR, with the Tegner activity scores actually being higher in the STR cohort. These findings indicate that STR may not interfere with normal postoperative recovery. This suggests that the use of this construct is at least not inferior to a construct without the STR.
Rates of meniscal injury at index surgery were slightly higher among the STR cohort, with 68% documented meniscal pathology compared with 48% in the no-STR group (although this difference did not attain statistical significance). The presence of meniscal injuries is a known risk factor for poorer outcomes after ACL reconstruction. 11,17 Yet, the STR cohort remained at least noninferior to those with no STR, despite higher rates of meniscal pathology.
Much of the interest in ACL graft reinforcement has been spurred by a need to overcome the high rates of failure observed in small diameter (<8 cm) grafts. 19 Inadequate soft tissue graft size is encountered frequently, particularly in adolescent populations. 10 Biomechanical study of the STR construct yielded encouraging results for patients with small graft diameter. 2 Our subgroup analysis of patients with graft size <8 mm found no significant difference in failure rates when comparing patients with STR and without STR, but the sample size was small. Further study with a larger cohort may be able to better identify whether or not STR is an effective technique for overcoming small diameter grafts. This could be tremendously useful, especially in light of the higher rates of failure seen in allograft augmentation of the smaller grafts in the younger patient population. 18,31,33
Limitations
There are a number of inherent limitations to our study that incorporate both components of retrospective design; however, by matching the follow-up duration and not introducing other technique or rehabilitation protocols, we hope that these are minimized, particularly since all the descriptive data and graft sizes between the 2 cohorts were similar without any further intervention to match the cohorts. Another limitation is the lack of preoperative outcome scores, particularly the Tegner score, which may have been higher in the STR cohort. However, since adolescent athletes tend to progress the Tegner score with age and improved skill, we still believe that the difference noted postoperatively reflects a true clinical difference in outcomes. Finally, as this study did not require an in-person visit between the 24- and 36-month time interval being studied, we do not have physical examination or radiographic measures to compare and assess. There is the possibility, despite the similar patient-related outcome scores that there could be a difference in alignment, range of motion, or knee laxity between the cohorts.
Conclusion
In this early outcome study, no complications that are unique to the introduction of the suture tape as a reinforcement for ACL reconstruction in adolescent patients were identified. In fact, patient-reported outcomes were either similar or improved in the STR cohort compared with the no-STR cohort. At a minimum, this could demonstrate no harm in incorporating the suture tape to reinforce the construct with hamstring tendon autograft in ACL reconstructions in adolescent patients. At best, there is a suggestion that STR may lower graft rupture rate, but further study is needed to evaluate the merit of STR in providing early structural support during graft integration and ligamentization, thereby reducing graft failure, especially in this at-risk younger population.
Footnotes
Final revision submitted December 10, 2021; accepted January 10, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.M., D.J.C., M.Y.S., and R.H. have received education payments from SportsTek Medical. E.W.E. has received nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California at San Diego (ref No. 161895).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.