
Abstract
Background:
Anterior cruciate ligament (ACL) repair is an alternative to reconstruction; however, suture tape support may be necessary to achieve adequate outcomes.
Purposes:
To investigate the influence of suture tape augmentation (STA) of proximal ACL repair on knee kinematics and to evaluate the effect of the 2 flexion angles of suture tape fixation.
Study Design:
Controlled laboratory study.
Methods:
Fourteen cadaveric knees were tested using a 6 degrees of freedom robotic testing system under anterior tibial (AT) load, simulated pivot-shift (PS) load, and internal rotation (IR) and external rotation loads. Kinematics and in situ tissue forces were evaluated. Knee states tested were (1) ACL intact, (2) ACL cut, (3) ACL repair with suture only, (4) ACL repair with STA fixed at 0° of knee flexion, and (5) ACL repair with STA fixed at 20° of knee flexion.
Results:
ACL repair alone did not restore the intact ACL AT translation at 0°, 15°, 30°, or 60° of flexion. Adding suture tape to the repair significantly decreased AT translation at 0°, 15°, and 30° of knee flexion but not to the level of the intact ACL. With PS and IR loadings, only ACL repair with STA fixed at 20° of flexion was not significantly different from the intact state at all knee flexion angles. ACL suture repair had significantly lower in situ forces than the intact ACL with AT, PS, and IR loadings. With AT, PS, and IR loadings, adding suture tape significantly increased the in situ force in the repaired ACL at all knee flexion angles to become closer to that of the intact ACL state.
Conclusion:
For complete proximal ACL tears, suture repair alone did not restore normal knee laxity or normal ACL in situ force. However, adding suture tape to augment the repair resulted in knee laxity closer to that of the intact ACL. STA with fixation at 20° of knee flexion was superior to fixation with the knee in full extension.
Clinical Relevance:
The study findings suggest that ACL repair with STA fixed at 20° could be considered in the treatment of femoral sided ACL tears in the appropriate patient population.
Keywords
Before the 1990s, led by several case series studies 24,26,39 with good short-term results, open primary anterior cruciate ligament (ACL) repair was considered as the preferred treatment for an ACL tear. However, the mid- and long-term follow-up of these patients after ACL repair with sutures 10,40 indicated an unacceptably high rate of knee instability ranging from 50% to 94%. Around the same time, prospective randomized trials showed that ACL reconstruction had superior results compared with ACL repair combined with a synthetic augmentation procedure, 8,38 which led to ACL reconstruction’s becoming the gold standard of treatment for patients with an ACL tear. 30
Recently, there has been renewed interest in ACL repair. 6 Improved surgical techniques (arthroscopy instead of an open approach, anatomic tunnel drilling versus transtibial, better quality of suture material, and implants such as suture anchors) 17,21,23 and new rehabilitation protocols (limited immobilization, accelerated protocols focusing on early range of motion, and quadriceps muscle activation) developed for ACL reconstruction 36 may be able to positively affect the outcomes of ACL repair. 18,33,41 However, animal models suggest that some type of reinforcing structure with the ACL repair is needed to achieve reasonable results. 44 The use of a flat, braided, ultrahigh-strength 2.0-mm suture tape for augmentation, commonly referred to as “internal bracing,” has become popular for a wide variety of soft tissue repairs in the field of orthopaedic surgery 16,44,45 including ACL repair. 18,33
Small clinical studies of ACL repair have had mixed results ranging from having no failures, 4 a failure rate of 7% to 15%, 18 to almost a 50% failure rate. 14 Possible reasons for the difference in results may be patient age and type of injury, 4,33 as well as the varying surgical techniques used in the repair. 4,14,18 It is known that surgical technique can affect the outcomes of ACL reconstruction 1 so there is reason to believe that this may also be true with ACL repair. Thus, as with ACL reconstruction, there is a need to understand the effects of different ACL repairs on knee biomechanics.
Currently, there is a paucity of knowledge regarding the effect of different ACL repair techniques on knee biomechanics under external knee loads. To this point, there is concern that the relatively strong and stiff reinforcement may potentially overconstrain the knee joint. At present, the only available quantitative biomechanical studies related to repair augmentation are the testing of the strength of the suture tape or pull-out strength of the construct in a single direction and/or knee flexion angle, 2,42 knee biomechanical tests with a double suture tape augmentation (STA), 3 or tests performed with animal specimens. 11,12 There are no quantitative biomechanical studies evaluating the effect of adding a single suture tape to ACL repair on knee kinetics and kinematics. Owing to the lack of data, there is no consensus on knee flexion angle for suture tape fixation in augmented ACL repair.
For this reason, the aims of this study were to (1) investigate the influence of adding suture tape to ACL suture repair on knee biomechanics and (2) evaluate the effect of knee flexion fixation angle of the suture tape on knee biomechanics. It was hypothesized that (1) ACL suture repair with STA would better restore knee laxity as compared with ACL suture repair alone and (2) fixation of the suture tape construct at 20° of knee flexion would be superior to fixation in full extension (0°). Although the ultimate success or limits of ACL repair are not known, data from this study will provide immediate guidance on repair techniques that can be used in future patient treatments and studies.
Methods
After receiving approval of the study protocol, we procured 17 human cadaveric knees from our institution-approved tissue suppliers for this study. Before inclusion, gross inspection was performed and specimens with any evidence of prior surgery, significant malalignment, or obvious signs of trauma were excluded. Next, arthroscopic inspection was performed to exclude knees with more than Outerbridge grade 2 cartilage changes in any compartment, meniscal injury or (partial) absence, or evidence of any other ligamentous knee injury. After exclusion of 3 specimens, a total of 14 specimens (7 female [50%], 4 right knees [29%]) with a mean age of 48.6 ± 12.7 years were included. The knees were kept frozen at –20°C and thawed at room temperature for at least 24 hours before testing.
All soft tissues 15 cm proximal and distal to the joint line were removed. The femur and the tibia were potted in cylindrical molds with an epoxy compound for fixation in custom clamps to the robotic testing system with the femur secured to a fixed base and the tibia fixed to the end effector of the robotic arm.
Surgical Technique for ACL Repair
ACL procedures were performed arthroscopically 4,37 by the same fellowship-trained orthopaedic surgeon with >5 years of experience (J.H.), and with the assistance of a second orthopaedic surgeon with >5 years of experience (R.K.), under the supervision and direction of the senior author (C.F.E) after refining the details of the technique in a pilot study. 7 Before the testing of the ACL intact state, the portals were made (Figure 1A), a partial infrapatellar fat pad resection and debridement of the synovium between the ACL and the posterior cruciate ligament was performed to optimize visualization. For the ACL cut state, a type 1 ACL tear (proximal avulsion tear) was simulated by cutting the ACL off from the femoral footprint using a banana blade (Figure 1). 22 The anatomy of the ACL, including the femoral attachment site location and fiber orientation, was identified to ensure anatomic ACL repair augmentation.
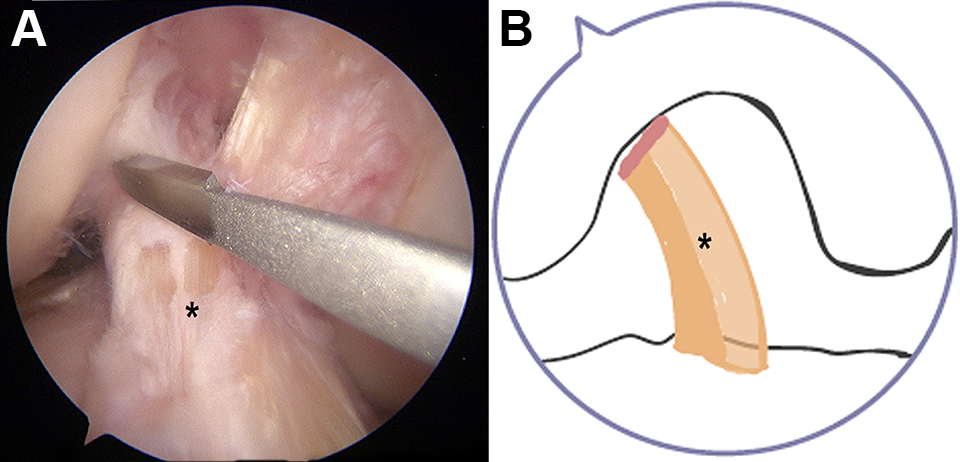
(A) Arthroscopic view of a right knee (lateral portal view at 90° of knee flexion) with the femoral insertion of the anterior cruciate ligament (ACL) cut with banana blade. (B) Type 1 proximal ACL tear model. Asterisk indicates ACL.
For the repair, 2 braided, flat, ultrahigh-strength, 1.3-mm sutures with a loop on 1 end (FiberLink SutureTape; Arthrex) were passed through and around the ACL using an arthroscopic suture passer, approximately 1 cm from where it was cut off the femur and placed in a luggage tag configuration (Figure 2). These 1.3-mm loop suture tapes were then passed into a 4-mm femoral bone tunnel located in the center of the ACL femoral attachment site and fixed at the lateral femoral cortex with an adjustable length suspensory fixation button. One braided, flat, ultrahigh-strength 2.0-mm suture was used for the STA, which was attached to the button loop, passed into a 2.4-mm tibial tunnel placed in the center of the tibial ACL footprint using an ACL drill guide set at 50°, and then fixed with a knotless suture anchor (4.75 mm diameter) at the anteromedial tibial cortex. The specimens were randomized into 0° or 20° of knee flexion STA tensioning for robotic testing and then the STA was released and tensioned at the other flexion angle and retested. Last, the STA suture tape was cut to test the suture repair–only construct.

Anterior cruciate ligament (ACL) arthroscopic repair combined with suture tape augmentation (STA) (right knee; lateral portal view at 90° of knee flexion): (A) schematic of 2, two 1.3-mm braided, flat ultrahigh-strength sutures with a loop placed in luggage tag configuration for ACL repair, (B) 2 repair sutures tensioned, (C) schematic of extracortical fixation of repair sutures and STA with anchor, and (D) ACL repair + STA. Asterisk indicates ACL.
Robotic Testing System
A 6 degrees of freedom robotic testing system (CASPAR Stäubli RX 90; Orto Maquet) was used for testing all knee specimens for kinematic and graft forces as described previously 35 and allowed for a ±0.02 mm of motion repeatability at each joint, using a Cartesian coordinate system with defined axes in the anteroposterior, mediolateral, and proximodistal directions of the tibia. The end-effector is connected to a universal force/moment sensor Model 4015; JR3 Inc) with a force and moment accuracy of ±0.2 N and ±0.1 N·m per manufacturer specifications. The intact knee undergoes a passive path determined by the robotic testing system from 0° to 90° of knee flexion, in 0.5° increments, by minimizing forces (<0.5 N) and moments (<0.25 N·m) in all remaining degrees of freedom. 47 A custom MATLAB (MathWorks Inc) program was used to perform control and data acquisition.
Five knee states were tested in each specimen: (1) intact (ACL intact), (2) proximal ACL avulsion created by cutting the ACL off the femoral attachment (ACL cut), (3) ACL repair with suture only (ACL repair), (4) ACL repair augmented with suture tape fixed at 0° (ACL repair + 0 STA), and (5) ACL repair augmented with suture tape fixed at 20° of knee flexion (ACL repair + 20 STA).
Each knee state was tested under 4 loadings: (1) 89.0-N anterior tibial (AT) loading, 5 (2) simulated pivot-shift (PS) test 19,32 consisting of a combined 7.0-N·m valgus load and then a 5.0-N·m internal rotation (IR) torque, (3) a 5.0-N·m external rotation (ER) tibial torque, and (4) a 5.0-N·m IR torque. The AT translation (ATT) under the AT was measured at 0°, 15°, 30°, 60°, and 90° of knee flexion; the ATT with PS, at the 0°, 15°, and 30° of knee flexion; and IR and ER, at 0°, 15°, and 30° of knee flexion. 34
To determine the in situ ACL tissue force, the previously recorded kinematic motion of the intact or repaired ACL knee was replayed with the ACL deficient knee and the knee forces were recorded with the universal force/moment sensor UFS. By the principle of superposition, 13,25 the change in the force measured before and after the removal of the ACL represents the in situ force in the ACL tissue.
Statistical Analysis
All data were reported as mean and standard deviation. The primary variable in this study was ATT. A prior power analysis was performed (G*power 3.1.9.2) 9 using a repeated-measures analysis of variance a significance level of .05, a power of 0.80, and an effect size of d = 1.0, based on previous data, 31 which resulted in 10 samples. In addition, although a previous study of ACL double-bundle repair had 10 samples, 3 a greater number of samples (N = 14) were used because of the paucity of biomechanical data on ACL repair. Statistical analyses were performed using SPSS Version 23.0 (IBM Corp). A repeated-measures analysis of variance was used to check for statistical differences (P < .05) between the means. This was followed with post hoc paired-samples t tests to compare the 4 knee states. The P value was adjusted within the software with a Bonferroni correction for multiple comparisons. For simplicity, the reported P values in the Results section and the figures have been adjusted in the software such that significance is still at P < .05.
Results
Kinematics
The ATT laxity of ACL repair alone versus ACL intact under AT loading at 15° and 30° of knee flexion were 10.6 ± 2.5 versus 4.9 ± 0.7 mm and 10.0 ± 2.1 versus 5.3 ± 1.0 mm, respectively. ACL suture repair alone (ACL repair) did not restore ATT to the ACL intact state. Compared with ACL repair alone, augmentation of the repair with suture tape at 0° of flexion resulted in decreased ATT at 0° (P < .001), 15° (P = .018), and 30° (P = .003) of knee flexion, and augmentation of the repair with suture tape at 20° of flexion resulted in decreased ATT at 0° (P = .002), 15° (P = .034), and 30° (P = .005) of knee flexion (Figure 3). When comparing fixing the STA reconstructions at 0° versus 20° of knee flexion, ACL repair + 20 STA resulted in decreased ATT at both 0° (P = .022) and 30° (P = .025) of knee flexion. The ATT laxity under AT loading at 15° of knee flexion in ACL repair + 20 STA and ACL intact were 6.4 ± 1.1 and 4.9 ± 0.7 mm, respectively. The ATT laxity under AT loading at 30° of knee flexion in ACL repair + 20 STA and ACL intact were 5.9 ± 0.7 and 5.3 ± 1.0 mm, respectively.
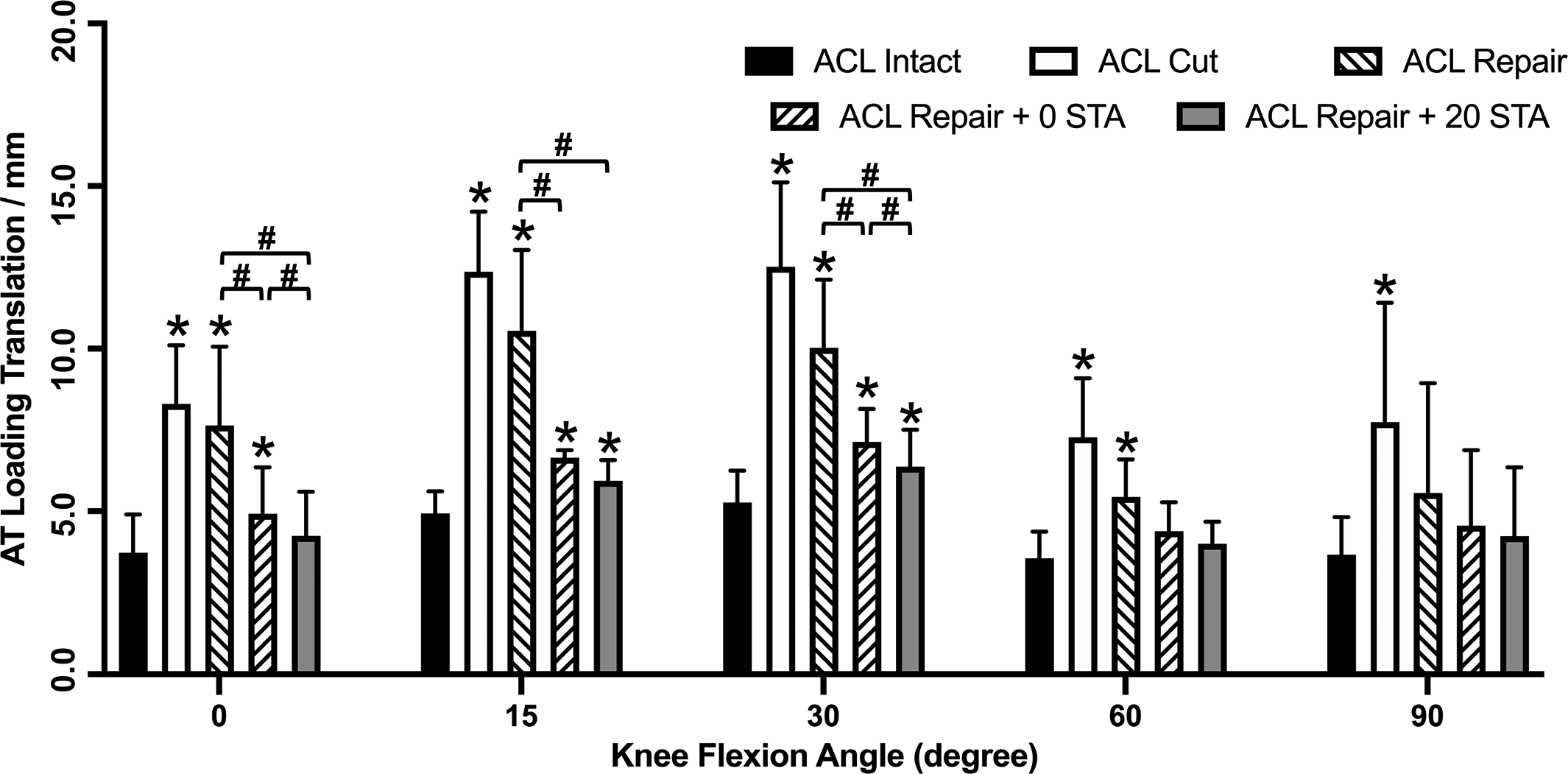
Anterior tibial translation under anterior tibial loading at different knee flexion angles. *P <.05 vs. anterior cruciate ligament (ACL) intact. # P <.05 with-in group comparison. STA, suture tape augmentation.
For ATT under simulated PS loading, only the ACL repair + 20 STA was not significantly different from the intact ACL at all flexion angles (Figure 4). With ACL repair + 0 STA, there were significant differences as compared with ACL intact at 0° and 15° of knee flexion.
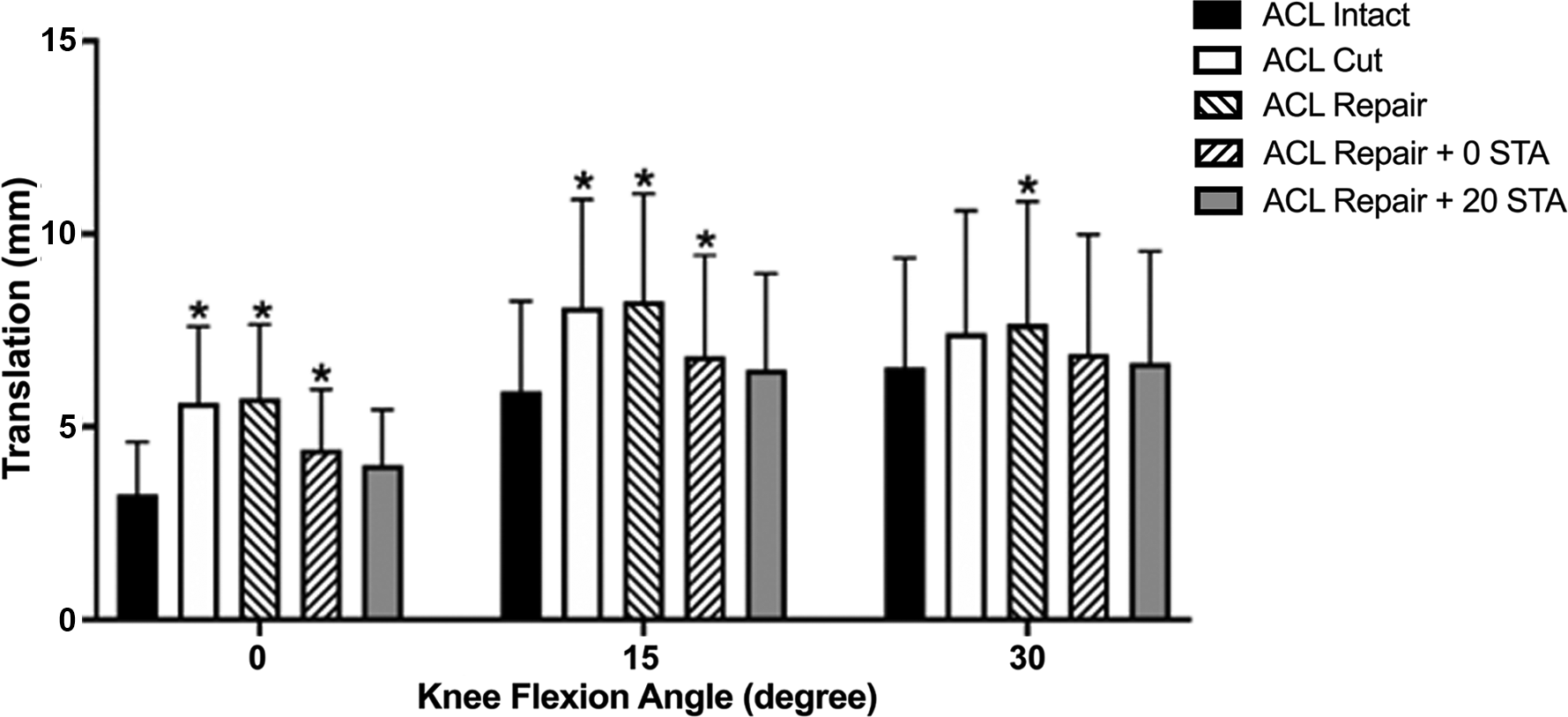
Anterior tibial translation under simulated pivot-shift loading at different knee flexion angles. *P <.05 vs. anterior cruciate ligament (ACL) intact. STA, suture tape augmentation.
With IR (Figure 5A) and ER (Figure 5B) torques, only ACL repair + 20 STA resulted in no statistically significant differences in rotation compared with ACL intact at all knee flexion angles. For IR, ACL repair + 0 STA had rotational differences compared with ACL intact at 0° and 15° of knee flexion, and for ER there was a difference at 0°.
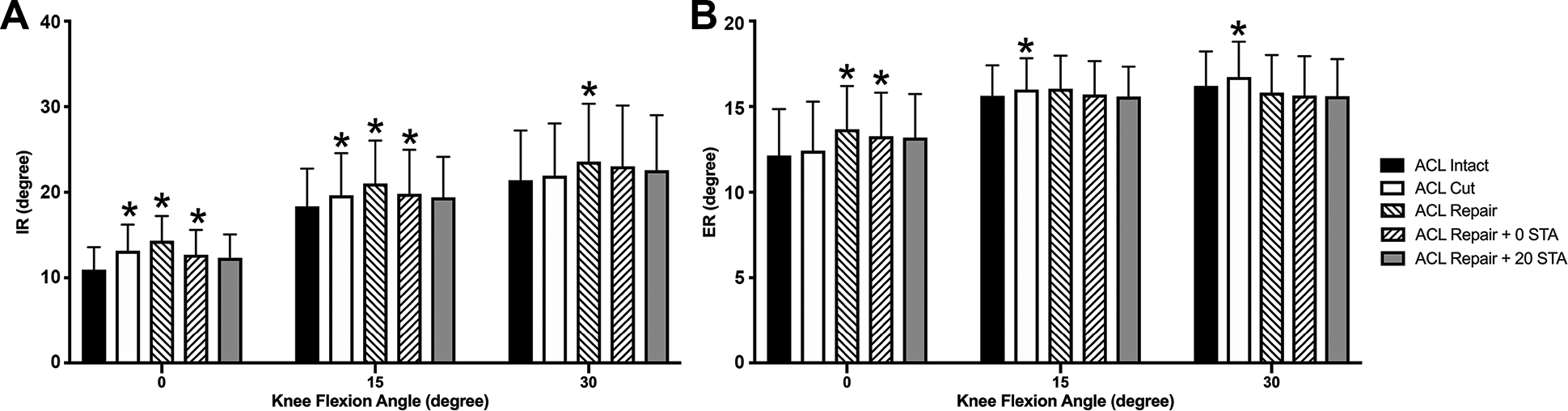
Rotation under (A) internal rotation (IR) and (B) external rotation (ER) torques as a function of knee state and flexion angle. *P <.05 vs. anterior cruciate ligament (ACL) intact. STA, suture tape augmentation.
ACL In Situ Force
Under both AT and simulated PS loads, ACL repair had significantly lower in situ forces compared with ACL intact at all flexion angles (Figure 6, A and B, respectively). Augmenting the ACL suture repair with suture tape significantly increased the ACL in situ force to repair alone at all knee flexion angles for both loading conditions. Both STAs (0° and 20°) had similar statistical comparisons to ACL intact, with the only difference being with AT load and 90° of flexion. However, ACL repair + 20 STA had an increased force for ATT under AT load at 0° and under PS loading at 15° of knee flexion when compared with ACL repair + 0 STA (P = .014 and .044, respectively). ACL repair + 20 STA did not restore tissue force under AT load to that of ACL intact at 15° (P = .032), 30° (P = .018), and 60° (P = .020) of knee flexion. ACL repair + 0 STA showed significantly lower tissue force than ACL intact at 15° (P = .002), 30° (P = .012), 60° (P = .001), and 90° (P = .011) of knee flexion.
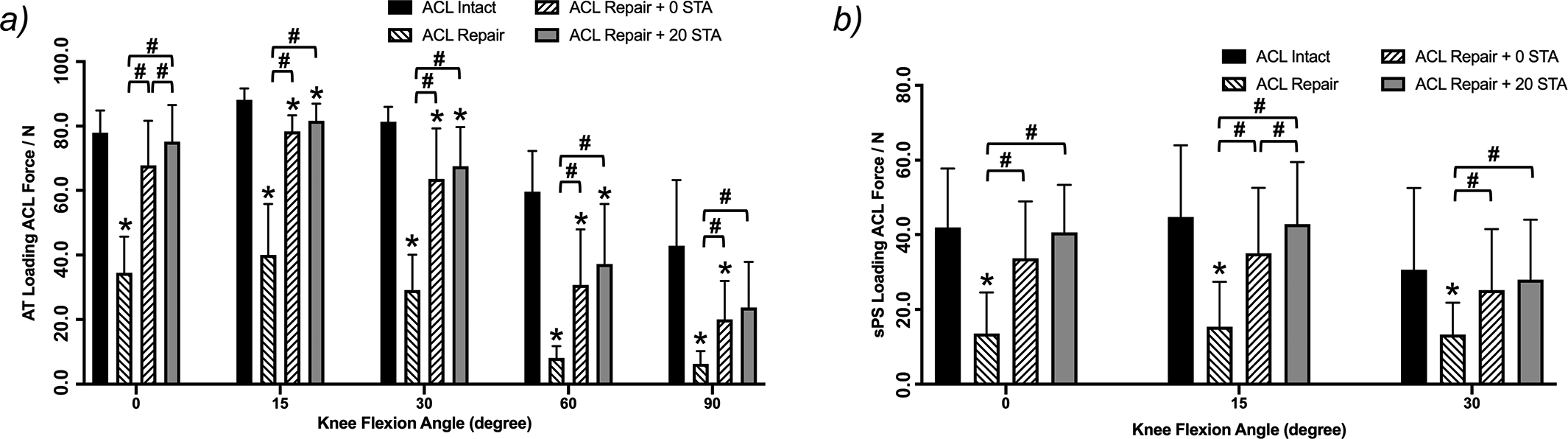
Anterior cruciate ligament (ACL) in situ force under (A) anterior tibial loading and (B) simulated pivot-shift loads as a function of knee state and flexion angle. **P <.05 vs. anterior cruciate ligament (ACL) intact. # P <.05 with-in group comparison. STA, suture tape augmentation..
ACL repair only resulted in significantly lower in situ forces compared with ACL intact at 0° (P < .001) and 15° (P = .002) of knee flexion under IR load (Figure 7A). Under IR load, except for ACL repair + 0 STA at 0° of flexion, both augmentations with suture tape increased the in situ force so that it was not significantly different from ACL intact. No differences in ACL in situ force were found between any of the tested states under ER load.

Anterior cruciate ligament (ACL) in situ force under (A) internal rotation and (B) external rotation torques as a function of knee state and flexion angle. *P <.05 vs. anterior cruciate ligament (ACL) intact. # P >.05 with-in group comparison. STA, suture tape augmentation.
Discussion
The most important finding of the present cadaveric study is that for proximal ACL tears, suture repair alone did not restore intact ACL knee laxity or intact ACL in situ force. Augmenting the repair with suture tape improved knee kinematics but not always to that of the intact ACL. Fixation of the suture tape at 20° of knee flexion was superior to fixation in full extension in improving knee kinematics.
A previous study with human knees compared the knee kinematics of ACL repair with 2 STAs (1 for each ACL bundle) with ACL reconstruction using a custom knee testing system. 3 The authors found that the ATT of the repair was not significantly different from the intact ACL, while the reconstruction had a larger ATT at 30° and 90° of knee flexion. No statistical difference was found in IR, ER, varus rotation, and valgus rotation between knees with the ACL intact, the ACL deficient, single-bundle ACL reconstruction, and ACL repair with double-bundle STA. These results differ substantially from the current study, which found significant differences in laxity between the intact ACL, deficient ACL, ACL repair, and ACL repair with STA in terms of ATT and IR/ER. Possible reasons for the difference in results is the use of a custom-built testing system versus 6 degrees of freedom robotic testing system or the use of 2 STAs in the repair, 1 for each bundle of the ACL, versus a single augmentation. 3
In a biomechanical study with porcine knees using various ACL repair techniques, Fleming et al 12 found that proximal ACL tears repaired with sutures to the femoral attachment, fixed in 60° of knee flexion, had an ATT not significantly different from that of the intact ACL, whereas fixation in 30° of knee flexion resulted in residual differences. In the porcine knee model, 30° knee flexion is full extension. The present study found that suture repair alone did not restore ATT at most flexion angles.
The findings of this study are consistent with those in the clinical literature. Historically, the first clinical studies on ACL repair showed residual laxity at mid- to long-term follow-up. 8,38 The present study shows that knee kinematics and ACL in situ forces are significantly inferior to the native ACL when the repair is not structurally augmented. A difference between the early clinical studies and the present study is the transition from an open to an arthroscopic approach, more focus on restoring the native ACL anatomy and footprint orientation, improvements in rehabilitation protocols eliminating prolonged bedrest and cast immobilization of the knee joint, and technological advances such as the development of stronger nonabsorbable suture material and stronger fixation methods such as suspensory fixation buttons and suture anchors. 44
One of the reasons behind the growing, renewed interest in ACL repair is this availability of new implants, materials, and technology. 28,29 A structurally sound repair construct may allow a decreased period of immobilization, faster postoperative recovery, less pain, and possibly earlier return to work, recreational activities, and even high-level sports. 15,20,27,33,46 This is further encouraged by the promising short-term clinical results, such as those reported by van de List et al , indicating that patients experienced a dramatically easier recovery after augmented repair than after reconstruction, with their knees reportedly performing more similarly to a native knee and with fewer complications. 43,44
Although some authors have reproduced these excellent outcomes, 4 others have reported less success, with Jonkergouw et al 18 finding a 15% failure rate with repair versus 7% for repair with STA for proximal ACL tears. Gagliardi et al 14 reported an almost 50% failure rate with ACL repair with STA fixed at full extension versus a <5% failure rate with ACL reconstruction. There is no consensus on the best method for ACL repair with STA and the variation in study results may be due to differences in techniques. This study quantified knee biomechanics data for different ACL repair technique which can provide guidance for future clinical studies or the practice of ACL repair with STA.
One concern of augmented ACL suture repair is overconstraint of the knee joint. In the present study, overconstraint, as defined by reduction of ATT below that of the intact knee, was not found. The ATT with suture repair alone or after adding the STA at either flexion angle was larger than with the ACL intact at all knee flexion angles. Although 20° did not seem to overconstrain the knee past full extension in this study, as with any knee reconstruction, care should be taken to ensure that full range of motion is achieved and comparable with that of the contralateral side.
Limitations
There are several limitations of this study. As a time-zero result, this study could not assess tissue healing, the effect of a load-sharing construct on the healing ligament, or the long-term effect of a nonabsorbable suture tape material in the intra-articular knee joint, all of which are important factors in ACL repair. The mean age (48.6 years) of the cadaveric knee specimens was older than the typical participants, skeletally immature to young adults, who would undergo ACL repair. This study only evaluated 1 type of ACL repair with STA construct and did not explore other structural or scaffolding constructs.
Conclusion
In the present cadaveric study, we have found that for complete proximal ACL tears, suture repair alone did not restore the normal knee laxity or normal ACL in situ force. The addition of suture tape to augment the repair resulted in knee laxity closer to that of the intact ACL. STA with fixation at 20° of knee flexion was superior to fixation at full extension. As with any knee reconstruction, care should be taken to ensure that full range of motion is achieved and comparable with the contralateral side.
Footnotes
Acknowledgment
In memoriam and appreciation of Freddie H. Fu, MD (1950-2021).
Final revision submitted August 29, 2022; accepted October 11, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The authors acknowledge the Albert B. Ferguson, Jr, MD, Orthopaedic Fund of The Pittsburgh Foundation. The implants used for this study were provided by Arthrex through a materials transfer agreement with the University of Pittsburgh. J.H. was supported by the program of China Scholarships Council and the National Natural Science Foundation of China (No 81802208). C.F.E. has received grant support from DJO and Zimmer Biomet and education payments from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study and the use of cadaveric specimens was obtained from the University of Pittsburgh Committee for Oversight of Research and Clinical Training Involving Decedents (CORID #864)