
Abstract
Background:
While many factors inform the choice of operative versus nonoperative treatment of injuries to the anterior cruciate ligament (ACL) of the knee, socioeconomic status influences this decision, as has been reported with other procedures.
Purpose:
To identify any associations between insurance status and likelihood of operative treatment of ACL injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The Nationwide Inpatient Sample database was queried using International Classification of Diseases, 9th Revision codes for ACL injuries and reconstruction from 2001 to 2013. Chi-square analysis was performed to determine significant predictors of operative intervention. Binary logistic regression was used to account for demographic and significant predictor variables. Results were recorded as odds ratios (ORs) and 95% CIs. Significance was defined as P < .05.
Results:
A total of 32,541 patients with ACL injuries were included in the final analysis. Overall incidence of surgical reconstruction was 85.4% (n = 27,805). Multivariable regression revealed that nonprivate insurance types were associated with lower likelihoods of operative reconstruction compared with private insurance: the lowest likelihood of operation was seen in uninsured patients (OR, 0.31; P < .01), followed by Medicare (OR, 0.33; P < .01) and Medicaid (OR, 0.51; P < .01) patients. There was also a decreased likelihood of surgery for elderly (OR, 0.0 [for age ≥75 years]; P < .01) and Black patients (OR, 0.65; P < .01). An increased likelihood of surgery was seen with female patients (OR, 1.14; P < .01). Patients in the highest median household income quartile were more likely to undergo surgery than those in the lowest (OR, 1.36; P < .01).
Conclusion:
Compared with privately insured patients, patients with nonprivate insurance had lower likelihood of surgery. Furthermore, patients in higher income quartiles were more likely to undergo operative fixation. These findings may suggest a need for more precise treatment guidelines and studies that investigate causes of such differences.
The anterior cruciate ligament (ACL) is an important translational and rotational stabilizer of the knee joint. It is most commonly injured in younger adults via a noncontact pivoting injury, where the tibia translates anteriorly in a slightly valgus and flexed knee, or through a direct lateral blow to the leg. 24,26 These injuries may be managed operatively or nonoperatively; potential benefits to operative reconstruction include decreased risks of future injury to other knee structures and posttraumatic arthritis. 1 Favorable outcomes, however, have also been shown to come from nonoperative treatment with rehabilitation, and no statistically significant difference has been demonstrated between the 2 treatment modalities in the adult population. 24 For the average adult patient, treatment guidelines are not clearly delineated because no superiority in functional outcomes has been demonstrated between the 2 treatment modalities. 7,15,24 Many sociodemographic factors also play a role in this decision-making process. Thus, the decision in how to treat ACL injuries rests with both the patient and the physician.
Disparities in surgical management based on insurance status have been demonstrated with many orthopaedic conditions, including those from traumatic and nontraumatic causes. 13,18 A recent census report revealed that 29.6 million Americans were without insurance in 2019, and another 114.3 million utilized public health insurance. 12 Disparities in health care delivery are complicated issues with ethical and economic implications that persist despite advances in health care delivery. As our population grows and compounds the economic strain on our health care system, the impact of insurance status in the discussion of operative treatment is of particular importance.
In the current study, we aimed to identify the association between insurance status and likelihood of operative reconstruction for ACL injuries. We hypothesized that those without insurance will have a lower likelihood of surgical reconstruction compared with those with private health insurance.
Methods
This study used information available in the Nationwide Inpatient Sample (NIS) database. The NIS is a national database maintained by the Healthcare Cost and Utilization Project (HCUP), which approximates a 20% sample of all discharges from US community hospitals. 10 It reports up to 25 possible diagnoses per patient and includes demographic, socioeconomic, and hospital administrative data.
We queried the NIS database for patients with ACL injuries between 2001 and 2013 using the International Classification of Diseases, 9th Revision (ICD-9) diagnostic codes 844.2 (sprain of cruciate ligament of knee) and 717.83 (old disruption of ACL). Data were weighted using HCUP-provided trend weights, which allowed the generation of national estimates. 9 Surgical treatment was determined by using ICD-9 procedural code 81.45 (other reconstruction of cruciate ligament). Although this procedural code is not restricted to ACL operative reconstruction, previous work by Lyman et al 16 demonstrated that 99.3% of procedures coded as such in a New York State database were specific to ACL reconstruction. We excluded patients with a concomitant diagnosis of posterior cruciate ligament disruption based on the presence of ICD-9 code 717.84, along with those with missing demographic, insurance, and income data.
Chi-square analysis was performed to determine significant predictors of operative intervention. Binary logistic regression was then used to account for demographic and significant predictor variables. Results were recorded as odds ratios (ORs) and 95% CIs. Significance was defined as P < .05.
Results
There were initially 33,342 inpatients with ACL injuries, and 801 patients (2.4%) were removed after exclusion criteria were applied. The final analysis included 32,541 patients. The prevalence of surgical reconstruction was 85.4%. Descriptive data of this patient sample can be found in Table 1.
Descriptive Data and Bivariate Analyses for Weighted Cases of ACL Reconstruction, NIS 2001-2013 (N = 32,541) a

a Bolded P values indicate statistically significant difference within compared groups (P < .05). ACL, anterior cruciate ligament; NIS, Nationwide Inpatient Sample; Other, not previously specified categories. Information regarding median household income quartile can be found in the Appendix Table A1.
After controlling for demographic variables, binary logistic regression revealed that patients with nonprivate insurance types were associated with lower likelihoods of operative reconstruction compared with those with private insurance as follows: the lowest likelihood of operation was seen in patients without insurance (OR, 0.31; P < .01), followed by patients with Medicare (OR, 0.33; P < .01) and Medicaid (OR, 0.51; P < .01) (Table 2).
Binary Logistic Regression Analysis of Predictors of ACL Reconstruction by Insurance Status a
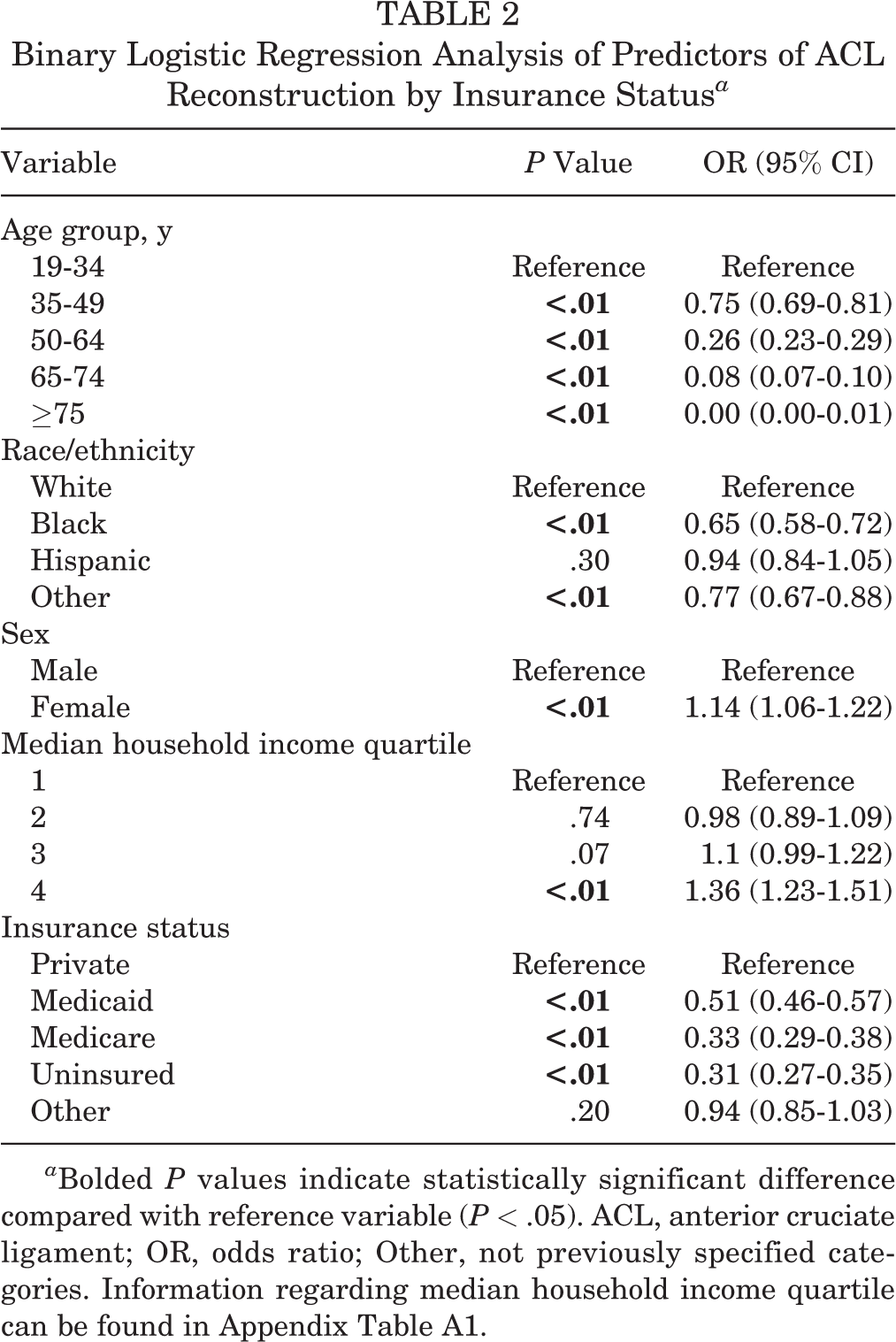
a Bolded P values indicate statistically significant difference compared with reference variable (P < .05). ACL, anterior cruciate ligament; OR, odds ratio; Other, not previously specified categories. Information regarding median household income quartile can be found in the Appendix Table A1.
A number of other factors affected operative incidence. A lower likelihood of surgery occurred with increasing age. Patients aged at least 75 years were least likely to undergo operative reconstruction (OR, 0.0; P < .01) when compared with those aged 19 to 34 years. Regarding race, Black patients (OR, 0.65; P < .01) were less likely to receive operative reconstruction than their White counterparts. Women were more likely to have a surgical reconstruction than men (OR, 1.14; P < .01). Patients in the highest median household income quartile were more likely to undergo surgery than those in the lowest (OR, 1.36; P < .01). Differences for the other income quartiles were not statistically significant.
Discussion
This database study included more than 32,000 patients to investigate the association between insurance status and likelihood of operative ACL repair. Patients with nonprivate insurance had lower likelihoods of surgical reconstruction compared with those who were privately insured. This includes those who are without insurance (OR, 0.31) or insured by Medicare (OR, 0.33) or Medicaid (OR, 0.51). This corroborates other recent studies that illustrate variances in operative fixation of other orthopaedic conditions based on insurance status. 3 Patients in higher income quartiles were also found to be more likely to undergo operative fixation.
In this study, Black patients were found to have a statistically significantly lower likelihood of operative ACL reconstruction than their White counterparts. A number of recent studies have demonstrated that Black patients are affected disproportionally by poverty and lack of health insurance. 11,25 In looking at health disparities between Black and White Americans, for example, Gornick 8 found that only 31% of the difference in mortality could be accounted for by a difference in risk factors, while 38% was linked to differences in income. Regarding orthopaedics, the Health and Retirement Study looked at individuals in need of a hip or knee replacement. 25 In the subsequent 2 years, Black participants were half as likely to receive surgery for their condition. This disparity could not be explained by other factors such as sex, comorbidities, employment, or level of disability. Another study found similar results when looking at total knee arthroplasty, as both Black and Hispanic participants were less likely to undergo replacement even after adjusting for appropriateness and socioeconomic status. 2
Insurance status is another known factor in health disparities. We found that patients with private insurance were more likely to undergo surgical reconstruction of the ACL than those without insurance or insured by Medicare or Medicaid. In addition, reconstruction was more likely in those with higher income. This echoes the findings of other studies. When assessing time to operative ACL reconstruction in the pediatric population, Newman et al 19 found that privately insured and more affluent patients progressed more quickly. Access to care is particularly influenced by socioeconomic and insurance status. In one study, researchers called orthopaedic offices requesting follow-up for ankle fracture, finding that only 1 in 7 patients with Medicaid insurance secured appointments. 18 Similarly, another study found that patients with Medicaid were much less likely than those with private insurance to get an appointment at an orthopaedic surgery practice with spine specialty care, and much more likely to require a primary care physician referral. 21
While operative fixation of ACL injury may be superior in objective stability of the knee, it has not been proven to be superior in functional outcomes. 24 Reconstruction was thought to prevent posttraumatic arthritis, but recent studies have not been able to prove this decrease in risk. 6,14,15 However, a reduction in meniscal injury may be a benefit to early operative treatment of these injuries. 4,5 At either end of the spectrum, treatment of these injuries may be more clear cut---a young professional athlete versus an older sedentary patient. 22 It is in the middle---a middle-aged recreational athlete, for example---where clear, evidence-based guidelines are needed.
Unraveling the various socioeconomic factors that affect the delivery of health care to patients across the country is a vast and arduous task. Factors such as race, income, education, geography, and health insurance tend to interact and affect each other in different ways. However, focusing on just 1 of these---health insurance in the case of this study---can continue to help us understand the root analysis of where these disparities exist and provide a framework for further research and implicate guidelines or policies to mitigate them. Insurance status of a patient is something surgeons are aware of prior to proceeding with surgical management. While we cannot know the decision-making process and all the elements that go into the choice of surgical versus nonsurgical treatment, the evidence that there is a difference between insured and uninsured groups warrants further investigation for its potential ethical implications.
Limitations
This study has several notable limitations. Owing to its retrospective nature, it is not possible to establish a cause-and-effect relationship between insurance status and operative treatment. In addition, limitations inherent to database analyses, such as lack of access to detailed information and impossibility of researcher oversight, are present in this study. Information such as concomitant ligamentous injury, meniscal injury, and preinjury functional status are pertinent to surgical decision-making. However, these factors are unlikely to be systematically different among patients of different insurance statuses. The ICD-9 codes used for indicating ACL injuries and operative reconstruction are not specific to the ACL, possibly allowing for the inclusion of other ligaments in our population. The work of others, however, has shown this risk is mitigated, as a previous review by Lyman et al 16 found the procedural code to be 99.3% specific to ACL reconstruction and others have shown the diagnosis code to be used reliably for ACLs. 16,17,27 Importantly, we also acknowledge that many ACL injuries are not treated in the inpatient setting but are often treated in surgery centers or in same-day procedures. Our conclusions are therefore limited only to those treated in the inpatient setting. We feel, however, that the primary question of the relationship of insurance status to operative treatment can still be addressed in this population.
Differences in patient- and surgeon-dependent factors may contribute to the described discrepancies but may also represent differences in health care utilization. Those with public insurance or no insurance have less access to health care, including subspecialty care such as orthopaedics. 23 This may lead to concerns related to postoperative follow-up and success of surgical management in this population. Further, physician reimbursement differs between private and public insurance. One study found that reimbursement for operative ACL reconstruction differed by about $3000 between private insurance and Medicaid, although this is dependent on the state. 20 These represent just a few hypotheses regarding the origin of such differences, but further investigation is necessary.
Conclusion
The results of this investigation indicated that insurance status is associated with likelihood of operative reconstruction for ACL injuries. More precise treatment guidelines for ACL injury should also be developed to minimize any physician-mediated bias in developing an appropriate treatment plan.
Footnotes
Final revision submitted October 22, 2021; accepted January 10, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G. has received education payments and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
APPENDIX TABLE A1
Median Household Income, by Year

| Year | Quartile | |||
|---|---|---|---|---|
| 1st | 2nd | 3rd | 4th | |
| 2001-2002 | $1-$24,999 | $25,000-$34,999 | $35,000-$44,999 | $45,000 or more |
| 2003 | $1-$35,999 | $36,000-$44,999 | $45,000-$59,999 | $60,000 or more |
| 2004, 2006 | $1-$35,999 | $36,000-$44,999 | $45,000-$58,999 | $59,000 or more |
| 2005 | $1-$36,999 | $37,000-$45,999 | $46,000-$60,999 | $61,000 or more |
| 2007-2013 | $1-$38,999 | $39,000-$47,999 | $48,000-$62,999 | $63,000 or more |
Source: Introduction to the HCUP Nationwide Inpatient Sample (NIS), 2001-2013. Available at https://www.hcup-us.ahrq.gov/db/nation/nis/nisarchive.jsp.