
Abstract
Background:
There is limited literature characterizing the incidence, variety, and effects of injuries and illnesses observed in elite swimmers.
Purpose:
To describe the epidemiology of injuries and illnesses affecting elite intercollegiate competitive swimmers.
Study Design:
Descriptive epidemiology study.
Methods:
This retrospective study utilized a deidentified injury and illness database of National Collegiate Athletic Association Division I swimmers in the Pacific Coast Conference from the academic years 2016 to 2017 and 2019 to 2020. A health event was defined as an illness or musculoskeletal injury that was identified by an athletic trainer or team physician. Musculoskeletal injuries and nonmusculoskeletal injuries and illnesses were stratified by body location. Injuries were further characterized as career-ending, season-ending, missed time but the athlete returned to sport in the same season, or those that did not cause missed time. Relative risk (RR) was used to compare the percentage of athletes affected between women and men, with statistical significance being defined by a 95% CI not including 1.
Results:
Included were 641 collegiate swimmers (301 male, 340 female). There were 1030 health events among 277 women and 173 men, with 635 (61.7%) occurring in women and 395 (38.3%) in men. There were 540 musculoskeletal injuries reported, most of which involved the shoulder (n = 126; 23.3%), spine (n = 95; 17.6%), foot/ankle/lower leg (n = 81; 15.0%), knee/thigh (n = 67; 12.4%), and hand/wrist/forearm (n = 52; 9.6%). A total of 490 nonmusculoskeletal health events were reported and included events such as respiratory tract infections (n = 119; 24.3%), unspecified medical illness (n = 93; 19.0%), concussions (n = 58; 11.8%), ear infections (n = 25; 5.1%), and gastrointestinal illnesses (n = 24; 4.9%). Compared with male swimmers, female swimmers were at a higher risk of sustaining both musculoskeletal injury (RR, 1.5; 95% CI, 1.22-1.83) and nonmusculoskeletal injury/illness (RR, 1.32; 95% CI, 1.04-1.68). There were 58 documented concussions, with 8 (13.8%) being season-ending, but not career-ending and 14 (24.1%) being career-ending. Women had a higher rate of concussion (9.1% vs 4.3% for men; RR, 2.11; 95% CI, 1.13-3.96).
Conclusion:
This retrospective study identified the most common injuries and illnesses observed among elite collegiate swimmers. Awareness of the incidence and outcome of injuries and illnesses that affect competitive swimmers may allow for more targeted analyses and injury prevention strategies.
Swimming is a unique low-impact sport involving prone positioning and hydrodynamic resistance that requires high levels of energy expenditure as well as cardiovascular training. 11,17 Thus, the injury patterns of this sport can be distinct from most other collegiate sports. Elite swimmers train an average of 2 to 4 hours a day and perform repetitive upper and lower extremity movements at high-intensity levels. 14,17,26 As a result, the observed injury patterns are thought to be largely the result of overuse and tend to occur in a training environment rather than in competition. 10,17,22,30 Despite the 12,980 women competing on 560 National Collegiate Athletic Association (NCAA) swimming teams and the 9799 men competing on 444 teams during the 2018 to 2019 academic year nationwide, the epidemiology of injury patterns and illnesses that affect elite swimmers and how they affect return to sport is largely uncharacterized. 12
Given the repetitive nature of overhead exercises associated with swimming, an overwhelming majority of the current literature has focused on assessments of joint laxity, muscle imbalances, and other biomechanical derangements of the shoulder. 5,32 This is perhaps because shoulder injuries are widely reported to be the predominant injury pattern observed in this patient population. NCAA swimmers have been reported to have low baseline shoulder functional and performance scores compared with other overhead athletes. 33,38 Furthermore, Olympic swimmers have been found to have a high prevalence of rotator cuff and biceps tendinopathy. 28 The complex static and dynamic properties of the relatively unconstrained shoulder joint, in combination with the unique cyclical biomechanics of any given competitive swimming stroke, have been the rationale for the observed hyperlaxity, scapular dyskinesis, labral damage, subacromial impingement, and glenohumeral rotational instability commonly diagnosed in the competitive swimmer. 21,32,33
Although the shoulder is the most injured body part among competitive swimmers, a variety of other injuries have also been reported. Knee injuries have been reported to comprise 3.1% to 17.7% of injuries observed among competitive swimmers and are also thought to occur due to overuse. 9,23,33 Furthermore, up to 75% of breaststroke swimmers report medial knee pain during their athletic career. 23 The technical intensity, repetitive propulsive pattern, and the inherent mechanical imbalance of the knee when performing breaststroke probably increase the risk of knee pain and injuries. 18 Lower back injuries are another relatively common reported area of injury in competitive swimmers, with some studies suggesting an even higher incidence of back injuries than shoulder injuries. 20,33 The lumbar spine is subjected to prolonged and repetitive hyperextension during all competitive swimming strokes, thus placing a tremendous load on the lumbar region, which is hypothesized to predispose these athletes to chronic lower back injuries. 25 Data on nonmusculoskeletal injuries and illnesses observed among competitive swimmers are generally limited; however, an epidemiologic study of all collegiate sports has suggested a low incidence of concussions in swimmers. 39
There has been little published epidemiologic data of injuries and illness health events among collegiate swimmers compared with athletes in other collegiate sports. As studies are often further limited by the lack of return-to-sport data, there is an identifiable need for epidemiologic studies in this patient population. This study aimed to characterize the injuries and illnesses observed among NCAA Division I male and female competitive swimming athletes and to determine which injuries and illnesses affect return to sport.
Methods
University men’s and women’s swimming rosters from respective websites of institutions making up the Pacific Coast Conference (Pac-12) were queried to determine the total number of male and female competitive swimmers during the 2016 to 2017, 2017 to 2018, 2018 to 2019, and 2019 to 2020 academic years. Athletes who transferred institutions within the Pac-12 conference were excluded from the analysis. Care was taken to ensure that athletes who remained on the team roster for multiple years were not included more than once when determining the total number of athletes included in this database.
The study protocol received an exemption from institutional review board approval. Given our institution’s membership in the Pac-12, we were able to acquire retrospective injury and illness data for the 2016 to 2017 through 2019 to 2020 academic years from the Pac-12 Sports Injury Research Archive. This data included all male and female collegiate swimmers from Pac-12 universities who had a documented health event defined as an injury or illness as reported by athletic trainers or physicians of respective university medical staff. These data were blinded and obtained in aggregate such that the data were appropriately deidentified. Musculoskeletal injuries stratified by body part, concussions, physical illnesses, and mental health events were included for analysis. Body parts included were as follows: shoulder, chest/abdomen, knee/thigh, foot/ankle/lower leg, hip/groin/pelvis/buttock, elbow/upper arm, head/face/neck (excluding concussions), and hand/wrist/forearm. Specific injury or illness diagnoses as well as sex differences were also included in the analysis. Health events were recorded as occurring in practice, competition, or in a nonsport setting completely unrelated to swimming.
Whether or not the athlete experienced any time away from competition was recorded for each health event. It was documented if the athlete did not miss any time from sport, if he or she missed time but returned in the same season, if one did not return in the same season (season-ending), or if one did not return to sport at all (career-ending).
In a separate analysis, the top 2 performing men’s and women’s teams each year at their respective NCAA Division I Swimming and Diving Championships during the period spanning 2016 to 2020 were compared against the remaining teams to determine whether the top 2 performing teams showed any difference with regard to injury and/or illness patterns.
All statistical analyses were performed using Microsoft Excel Version 16.49 (Microsoft Corp) in consultation with the biostatistics core facility at our institution. “Athletes affected” was defined as the number of athletes having at least 1 of the recorded health events during the 4-year observation period. “Estimated athlete risk per year” was used as a surrogate for risk per athlete-year since observation periods were not known for each individual athlete due to the data being blinded. We estimated that, on average, athletes were followed for 2.3 years, which assumes an equal number of freshmen, sophomores, juniors, and seniors per year and no athletes transferring/quitting. For example, a freshman in 2016 would be followed 4 years, a senior in 2016 would be followed 1 year, a freshman in 2017 would be followed 3 years, and so forth, with 2.3 years being the weighted average. Relative risk (RR) was used to compare the percentage of athletes affected between sexes, with statistical significance being defined by a RR 95% CI not including 1 (P < .05).
Results
Between 2016 and 2020, a total of 641 collegiate swimmers competed at Pac-12 institutions and were included in our analysis, with 301 (47.0%) being male and 340 (53.0%) being female. Of those 641 athletes, 450 (70.2%) were reported to have a defined health event and were included in our analysis. Of these 450 athletes, 173 (38.4%) were male, and 277 (61.6%) were female. In total, 1030 total health events in these 450 athletes were included for analysis, with 395 (38.3%) occurring in male swimmers and 635 (61.7%) occurring in female swimmers.
Musculoskeletal injuries accounted for 540 health events, including 126 (23.3%) shoulder injuries, 95 (17.6%) spine injuries, 81 (15.0%) foot/ankle/lower leg injuries, and 67 (12.4%) knee/thigh injuries. Overall, 17.3% of collegiate swimmers were observed to be affected by a musculoskeletal injury at any point during an academic year during our observation period. These athletes were at a 6.9% risk of sustaining a shoulder injury, a 5.7% risk of sustaining a spine/back injury, and a 5.1% risk of sustaining a foot/ankle/lower leg injury (Table 1). Nonmusculoskeletal conditions accounted for 490 recorded health events, the most common of which were respiratory tract infections (n = 119; 24.3%), unspecified medical illnesses (n = 93; 19.0%), concussions (n = 58; 11.8%), ear infections (n = 25; 5.1%), and gastrointestinal illnesses (n = 24; 4.9%). Collegiate swimmers were at a 5.4% risk of having a respiratory tract infection, a 3.0% chance of sustaining a concussion, and a 1.4% chance of having an ear infection in a given year (Table 2). Of note, 50.4% of musculoskeletal injury events occurred in practice (n = 272 events); 13.5%, in the weight room (n = 73 events); 8.1%, in a non–sport related event (n = 44 events); and 3.9%, during competition (n = 21 events); and 24.1% were not specified (n = 130 events). No statistical significance was observed between the top 2 performing teams in a given year (referred to as “elite”) and the remaining teams for any musculoskeletal injury diagnoses (Table 3).
Musculoskeletal Injuries by Body Part in Collegiate Swimmers, 2016 to 2020 a

a Data are reported as n (%) unless otherwise indicated.
b Relative risk, female vs male.
c Statistical significance (P < .05).
d Excludes concussions.
Nonmusculoskeletal Illnesses in Collegiate Swimmers, 2016 to 2020 a

a Data are reported as n (%) unless otherwise indicated.
b Relative risk, female vs male.
c Detailed data to determine what kind of medical illness unavailable.
d Statistical significance (P < .05).
Top 5 Musculoskeletal Injuries and Nonmusculoskeletal Illnesses Among Elite Versus Nonelite Athletes a

a Data are reported as n (%) unless otherwise indicated.
b Relative risk, elite vs nonelite.
c Statistical significance (P < .05).
d Detailed data to determine what kind of medical illness unavailable.
A total of 44 athletes sustained 58 documented concussions, with 12 athletes (27.3%) sustaining a repeat concussion and 2 of those athletes sustaining 2 repeat concussions. Women had significantly higher rates of concussion (RR, 2.11; 95% CI, 1.13-3.96), as 31 (9.1%) out of 340 female athletes sustained a concussion as compared with 13 (4.3%) out of 301 male athletes. Women were at a 4.0% risk of sustaining a concussion in a given year, whereas men were at only a 1.9% risk. Out of 58 concussions, 34 (58.6%) resulted in missed time but with a return to sport within the same season. Out of 58 concussions observed in this series, 8 (13.8%) were season-ending injuries, whereas 14 (24.1%) out of 58 were career-ending (Table 4). Of the concussions, 11 (25.6%) out of 43 in women and 3 (20.0%) out of 15 in men were career-ending.
Return-to-Sport Data for Most Common Diagnoses for Musculoskeletal Injuries and Nonmusculoskeletal Illnesses a
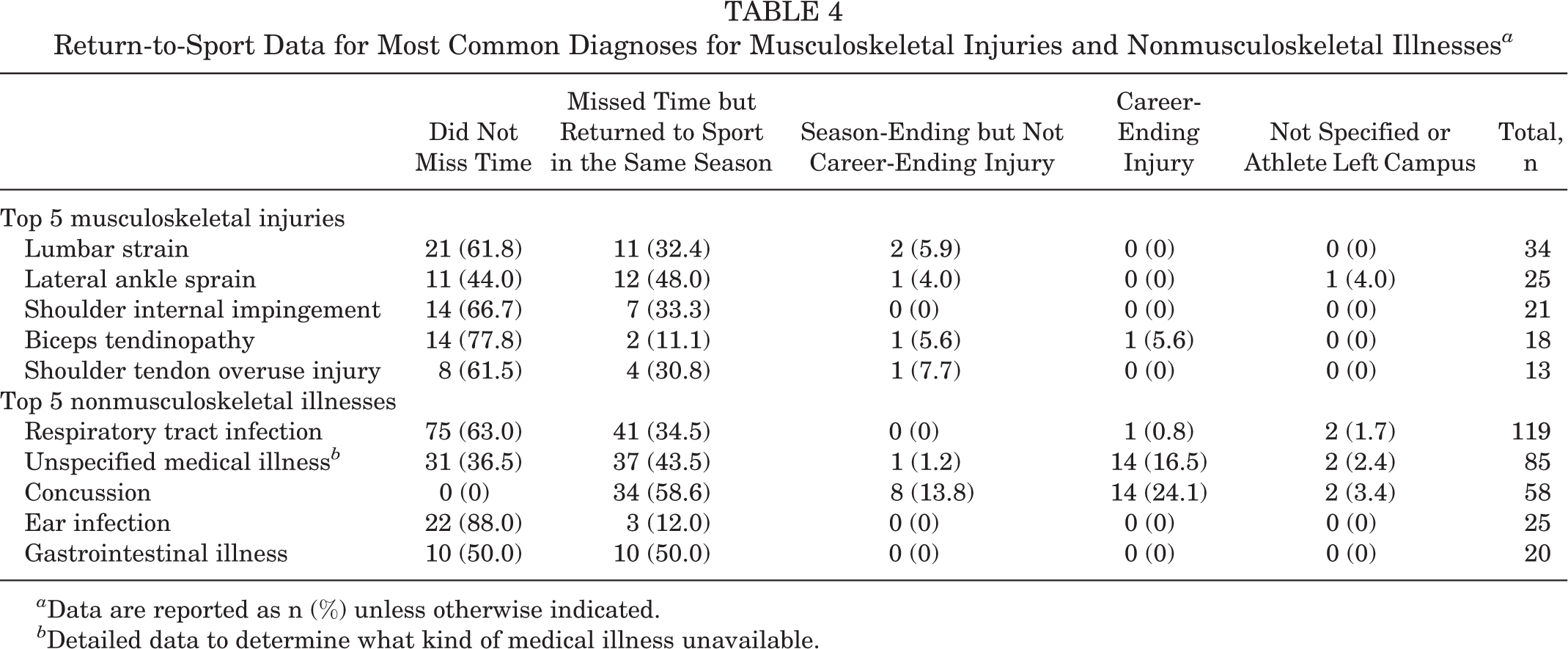
a Data are reported as n (%) unless otherwise indicated.
b Detailed data to determine what kind of medical illness unavailable.
The most common diagnoses of the 540 musculoskeletal injuries were lumbar strains (n = 34; 6.3%), lateral ankle sprains (n = 25; 4.6%), shoulder impingement (n = 21; 3.9%), biceps tendinopathy (n = 18; 3.3%), and shoulder tendon overuse injuries (n = 13; 2.4%) (Table 4). Only 3 (2.4%) out of 126 of shoulder injuries were season-ending compared with 0 out of 67 knee/thigh injuries that were season-ending. Only 1 (0.8%) out of 126 shoulder injuries were career-ending compared with 5 (7.5%) out of 67 of knee/thigh injuries that were career-ending. Table 5 represents the remaining return-to-sport data for the most common musculoskeletal injuries stratified by body part.
Return-to-Sport Data for Most Common Musculoskeletal Injuries, Stratified by Body Part a
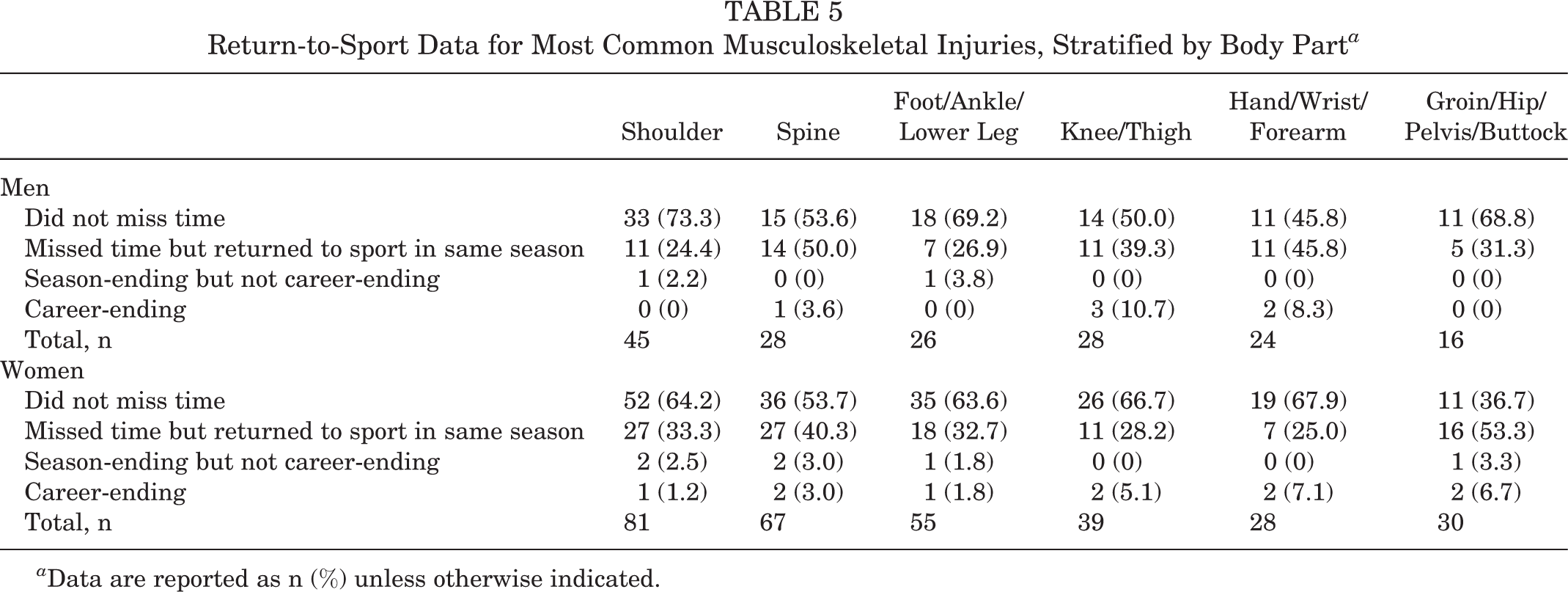
a Data are reported as n (%) unless otherwise indicated.
Discussion
The current breadth of literature analyzing injuries and return to sport among elite swimmers is limited by number of studies, methodological limitations, and/or sufficient sample size; thus, it is generally accepted that there is an identifiable current demand for research addressing this knowledge gap. 10,33,37 The current study used a health database from the Pac-12 conference to better understand the prevalence of injuries and illnesses as well as associated return to sport among male and female collegiate swimmers. Although the current study analyzed swimmers from the Pac-12 conference, the authors believe these results are comparable with all collegiate swimmers.
Shoulder injuries accounted for 126 (23.3%) out of the 540 total musculoskeletal injuries seen in this study (Table 6). Although the shoulder was expectedly the body part most commonly affected in musculoskeletal injuries, only 1 out of the total of 126 shoulder injuries was career-ending. Furthermore, only 3 other shoulder injuries were season-ending, indicating that although it is well known that shoulder conditions are highly prevalent among swimmers and shoulders were the body part most commonly injured in our study, these injuries may not significantly affect a swimmer’s ability to return to sport. Out of all 126 shoulder injuries, 85 (67.5%) did not result in any missed competition time. This is relatively consistent with findings from Wolf et al 37 demonstrating that 32 (58.2%) out of 55 shoulder injuries did not result in any missed competition time. As particular attention is paid to the shoulder in these athletes, there may be a lower threshold to diagnose such conditions, leading to the recognition of more minor injuries than otherwise may have been documented. This could be the rationale behind the relatively high return-to-sport rate observed in our study with regard to shoulder injuries.
Shoulder Injury Characteristics Observed Among Athletes in This Study a

a Data are reported as n (%) unless otherwise indicated.
b Relative risk, female vs male. The dashes indicate instances where either 0 females and/or 0 males were affected, which would make the RR a nonnatural number.
c Statistical significance (P < .05).
Spine/back injuries were also relatively common in our population, accounting for 95 (17.6%) of the 540 musculoskeletal injuries, with lumbar strains being the most common musculoskeletal-specific diagnosis. Back injuries are understood to be relatively common in swimmers and are thought to be from overuse. 1,13 Furthermore, overuse as well as excessive hyperextension has been indicated as a factor that predisposes swimmers to degenerative disk disease, spondylolysis, and spondylolisthesis. 24 As a result, it is not surprising that lumbar spine injuries were commonly observed in our series.
While knee injuries are thought to be the next most common body part injured in swimmers, the results of the current study suggested that injuries below the knee (foot/ankle/lower leg) accounted for 81 (15.0%) out of 540 musculoskeletal injuries and were more common than knee/thigh injuries (n = 67 out of 540; 12.4%). Matsuura et al 20 observed that an increase in the incidence of knee injuries over time corresponded to the introduction of the starting block between 2008 and 2010; they hypothesized that the kick start using these starting blocks may be the rationale behind this increase. It is possible that the load applied to the structures below the knee during this kickoff may also contribute to the relatively high rate of foot/ankle/lower leg injuries seen in this study; however, it is worth noting that track start starting blocks are used infrequently out of competition.
Several significant sex-based differences were noted in our results. Overall, women were at a significantly higher risk of sustaining any musculoskeletal injuries (RR, 1.5; 95% CI, 1.22-1.83) in a given year. Women had an 8.4% risk of sustaining a shoulder injury in a given season, which was significantly higher compared with men (5.2%) (RR, 1.6; 95% CI, 1.1-2.33). Women were also at a significantly higher risk of sustaining a spine/back injury (7.2% vs 4.1% in men) (RR, 1.77; 95% CI, 1.16-2.71) or a foot/ankle/lower leg injury (6.4% vs 3.6% in men) (RR, 1.77; 95% CI, 1.12-2.79) (Table 1). It is plausible that anatomical differences between male and female hip structures predispose female swimmers to lower body injuries. Furthermore, it has been reported that psychosocial factors can discourage men from reporting symptoms compared with women, and this could account for the sex differences we observed in this study given the relative uniformity in significantly higher risk of musculoskeletal injury in women. 15
Another interesting finding of the current study was the relative high rate of concussion. Concussions affected 44 (6.9%) of the 641 athletes included in this study (Table 7); 14 of those athletes had their career ended by these concussions. The concussion rate in this study is much higher than the 1.7% rate suggested in the limited literature on concussions in swimmers. 37 As more attention has been placed on the health effects and long-term sequelae of concussions in recent years, this difference in concussion rate may be attributed to increased recognition of concussion mechanisms and symptoms. This study also found that female swimmers were significantly more likely to sustain a concussion than were male swimmers (RR, 2.11; 95% CI, 1.13-3.96) (see Table 2). This is inconsistent with the limited literature on swimming injuries claiming that there may not be a difference in concussion rates between male and female swimmers. 3 That being said, several sex comparison studies in other sports have demonstrated that female athletes have higher rates of concussions than their male counterparts at the high school, collegiate, and professional levels have. 4,6,7,29,34,39 The rationale behind this difference is poorly understood; however, possible theories include neuroanatomical and/or biomechanical differences as well as psychosocial factors that may cause male athletes to underreport symptoms. 4,15,31 While this study could not comment on mechanisms behind the observed sex differences in concussion rates, these results also showed that women had a slightly higher incidence of concussion’s being career-ending (n = 11 out of 43; 25.6%) compared with men (n = 3 out of 15; 20.0%). A systematic review by Koerte et al 19 suggested that, although no definitive conclusions can be made regarding sex differences for sports-related concussion outcomes, the majority of evidence suggests that women generally have worse clinical and neurologic outcomes after sports-related concussion. This may explain the higher rates of concussion being career-ending in women observed in our study. While contact sports such as football and rugby get more attention with regard to concussion prevention and management, these results suggested that concussion prevention programs and treatment protocols specific to the sport of competitive swimming should be developed.
Concussion Characteristics Observed Among Athletes in This Study a

a Data are reported as n (%) unless otherwise indicated.
b Relative risk, female vs male. The dashes indicate instances where either 0 females and/or 0 males were affected, which would make the RR a nonnatural number.
c Statistical significance (P < .05).
Respiratory tract infections were the most common medical illnesses in our population, accounting for 119 (24.3%) out of 490 of all illnesses. Although respiratory tract infections are among the most common illnesses regardless of age or sex, swimmers have been shown to be particularly predisposed. 27 This is thought to be due to intense training in a chlorinated environment, vitamin D deficiency being common in this population, and/or sustained variations in ventilation during sport affecting the airway epithelium. 2,35 Interestingly, a review article by Falagas et al 8 suggested that, in general, male patients are likely to be more susceptible to respiratory tract infections than are female patients in all age groups. In the current study, no significant sex difference was noted with regard to respiratory tract infections (Table 2). With the relative high rates of respiratory tract infection in swimmers, routine screening procedures for these illnesses should also be a consideration.
Limitations
This study had several limitations in addition to the those inherent in a retrospective study. We only captured 4 academic years' worth of data (2016-2020) among collegiate swimmers; therefore, long-term follow-up data to determine how acute injuries/illnesses affect these athletes in the long term, including return to sport outside of intercollegiate competition, are difficult to ascertain. Using this data set, we were unable to definitively identify the reasons for an athlete’s not returning to sport after an injury or illness. Presumably, a majority of athletes did not return to sport solely due to the actual injury or illness; other factors such as personal choice or psychosocial factors could certainly also be involved. The current study was also not well equipped to stratify injuries based on mechanism, acuity, or severity as detailed injury, and treatment reports were not available. This level of detail would allow for a more comprehensive classification of the injuries and illnesses that affect collegiate swimmers. More specific to this data set, 93 (19.0%) out of 490 of nonmusculoskeletal illnesses were categorized as “unspecified,” as there were no detailed data available. Furthermore, diagnoses captured in this database could be assigned by a variety of members of the medical team, including athletic trainers, physical therapists, primary care physicians, orthopaedic surgeons, and psychologists. Thus, the diagnostic criteria and the diagnostician were undefined in this data set across multiple institutions, which presents a theoretic confounder that is challenging to quantify. The data presented in this study were also not stroke specific, which limited more nuanced, biomechanical associations with specific injury patterns. For instance, evidence has suggested that the high angular velocity at the knee associated with the breaststroke kick predisposes swimmers to medial knee injuries. 16,36 Another limitation to this study was that there were no data with regard to the number of exposures (practices, workout sessions, competitions) for each school, and it was assumed that the number of exposures between teams and genders was relatively comparable. Despite these limitations, this study remains 1 of the largest and most comprehensive epidemiologic studies characterizing injuries and illnesses among high-level competitive swimmers.
Conclusion
Most current injury prevention strategies in swimming focus on the shoulder; however, these results suggested that swimmers sustain a variety of musculoskeletal injuries and nonmusculoskeletal health events including concussions at alarming rates that warrant closer attention. Understanding the incidence of the diverse health events observed among elite competitive swimming athletes can inform clinicians regarding the natural history of common injuries and illnesses. This knowledge may help sports medicine practitioners better manage the expectation of these athletes with regard to return to sport after injury and illness, as well as allow for more targeted injury prevention strategies, that may ultimately serve to prolong the career of elite competitive swimmers.
Footnotes
Acknowledgment
Special thanks to Jeffrey Gornbein, DrPH, in the UCLA Department of Biomathematics for his assistance with the statistical analysis for this study. The authors thank the Pac-12 Health Analytics Program data custodians, including Kevin Robell, MA, ATC, for their assistance with review of the available data elements and for providing the data set. In addition, the authors thank the numerous certified athletic trainers and other allied health team members for their invaluable contributions to this work through the input of the health event data points captured in the Pac-12 Health Analytics Program database.
Final revision submitted October 19, 2021; accepted November 30, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support for T.J.K. was provided by the US Department of Veterans Affairs (project 2020-000059). T.J.K. has received education payments from Micromed, consulting fees from Heron Therapeutics, honoraria from Musculoskeletal Transplant Foundation, and hospitality payments from Fidia Pharma, RTI Surgical, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of California, Los Angeles.