
Abstract
Background:
Although arthroscopic partial meniscectomy is a widely implemented surgical procedure, studies investigating the time to return to activity (RTA) are rare.
Purpose:
To explore which factors are associated with the RTA times after arthroscopic partial meniscectomy and to investigate whether those factors can also improve short-term patient-reported outcomes.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The authors reviewed the records of patients who underwent isolated partial meniscectomy in their institution from January 2017 to December 2019. Patient and injury characteristics were documented, and time to RTA was obtained via phone interview in January 2021. Pre- and postoperative outcomes were assessed with the Lysholm score and International Knee Documentation Committee (IKDC) score. The chi-square test and independent-samples t test were used to evaluate differences in outcome scores and time to RTA according to the patient and injury characteristics, and risk factors with a P value <.1 in the univariate analysis were used in the binary regression.
Results:
Included were 215 patients (87 men and 128 women; mean age, 33.7 years [range, 24-75 years]). Of these patients, 204 provided information on time to RTA (mean, 3.3 months). By 3 months postoperatively, 49.5% (101/204) of patients could perform activities without knee-related restriction; this improved to 69.6% (142/204) at 6 months and 90.2% (184/204) at 12 months. On multivariate logistic regression analysis, age (OR, 0.39; 95% CI, 0.21-1.19; P = .044) and injury duration (OR, 0.20; 95% CI, 0.19-1.07; P = .032) were significantly associated with the time to RTA. IKDC scores improved significantly from 41.2 preoperatively to 76.7 postoperatively, and in the multivariate logistic regression model, female sex (OR, 2.67; 95% CI, 1.10-6.47; P = .030), body mass index (BMI) ≥27 kg/m2 (OR, 2.96; 95% CI, 1.02-8.66; P = .047), and medial meniscal tear (OR, 0.20; 95% CI, 0.04-1.00; P = .050) were associated with inferior outcome scores.
Conclusion:
Patients aged 40 years and younger who underwent partial meniscectomy surgery within 6 months after a meniscal tear were more likely to have a shorter time to RTA, and female patients with obesity (BMI ≥27 kg/m2), especially those with medial meniscal tears, tended to have inferior clinical outcomes.
Partial meniscectomy is a widely implemented surgical procedure when meniscal injury is present to relieve meniscal symptoms, including pain and knee locking. 1 The great concerns for patients after operation are “How long before I can return to normal daily activities or work?” and “How can I return to daily activities or work faster?” 21 Nevertheless, studies investigating the time to return to activity (RTA) after arthroscopic partial meniscectomy are rare. In a cohort study, Nawabi et al 22 found that patients with lateral meniscal tears need a mean of 7 weeks to return to the preinjury activity level, which is significantly longer than the 5 weeks of those with medial meniscal tears. However, in the study, only professional soccer players were included. In another study, 2 the authors concluded that approximately 77% of patients who underwent partial meniscectomy returned to play at a mean of 2 months postoperatively, and higher preoperative Knee injury and Osteoarthritis Outcome Score (KOOS) for pain was associated with the time of return to sports.
Another concern for patients is the extent to which they can recover after arthroscopic partial meniscectomy. A large number of studies have been performed in previous literature to investigate the predictive factors of clinical outcomes for patients who underwent partial meniscectomy. 8,9,13,16 However, we found that most of those studies either had strict inclusion criteria for participants (age-specific patients or unilateral meniscus), had a small sample size (n < 100), or evaluated the association of postoperative outcomes with a single specific factor. 9,15,24 Ghislain et al 12 performed a study with 117 patients comparing the clinical outcomes between traumatic and degenerative meniscal tears and concluded that patients with traumatic meniscal injury have better outcomes. In their study, the influence of other demographic variables on clinical outcomes was not evaluated. In addition, we found that little consensus has already been reached about which patient-related factors positively affected clinical outcomes. 4,9,17
The purpose of this study was to evaluate the association of short-term patient-reported outcomes (PROs) and RTA times with patient and injury characteristics in nonathletes after arthroscopic partial meniscectomy. We hypothesized that patients with obesity who are diagnosed with lateral meniscal tears and chronic lesions (>6 months from injury) will have inferior clinical outcomes and a longer time to RTA.
Methods
This study protocol was approved by our institutional review board. A total of 215 patients who underwent isolated partial meniscectomy in our institution from January 2017 to December 2019 by 2 surgeons (C.X. and D.C.) were included in the current study. The inclusion criteria were (1) a meniscal tear treated with partial meniscectomy surgery, (2) no other concomitant ligament injury, and (3) contact at the last follow-up.
Injury Diagnosis and Treatment
Meniscal injury was determined by clinical examination, magnetic resonance imaging (MRI), and intraoperative findings. Surgical procedures were performed by 2 independent surgeons: one with 20 years of working experience (D.C.) and the other with 5 years of working experience (C.X.). Anterolateral and anteromedial knee portals were utilized for all patients. Under arthroscopy, the meniscal tear patterns and the site, as well as the degree of chondral lesion, were directly viewed by the surgeons. Then, the surgeon determined a suitable procedure for each patient based on the following standards: (1) the location of the meniscal tear (red-on-red, red-on-white, or white-on-white zones; ie, if the location is in a red zone, the vascularity should be adequate to enhance the healing rate of the meniscus 23 ) and (2) the severity of meniscal injury, that is, whether the remaining meniscal tissue was adequate to make repair viable. When meniscal repair was not viable, the injured meniscus was trimmed until a stable peripheral rim was achieved.
For patients who underwent repair surgery, an angle-adjustable brace was used until 4 weeks after surgery. The angle of knee flexion was less than 45° within 2 weeks after meniscal repair and reached a similar angle to the uninjured side 4 weeks after operation. Partial weightbearing was allowed until 4 weeks after surgery with the help of a crutch, and total weightbearing was encouraged 6 weeks after the operation. For patients who underwent partial meniscectomy, total weightbearing and flexion and extension were encouraged the day after the operation.
Study Data and Outcome Measures
The following patient and surgery data were obtained from the medical records: sex, age, body mass index (BMI), surgeon experience, time from injury to surgery, and intra-articular factors such as tear laterality (medial or lateral), degree of chondral lesion, and tear mechanism. The degree of chondral lesion was classified using the International Cartilage Repair Society (ICRS) grading system, which ranged from 0 (normal) to 4 (very severe lesions). Pre- and postoperative clinical outcomes were assessed with the Lysholm score and International Knee Documentation Committee (IKDC) score. We defined return to activity (RTA) as the time when patients could perform low-intensity activities, such as working, walking, and housework, without any knee-related restrictions. The PRO scores and time to RTA were obtained via phone interviews in January 2021. Patients were requested to answer all questions on the questionnaire.
For the purposes of this analysis, the Lysholm and IKDC scores were dichotomized into good and poor clinical outcomes, with their mean values (88 and 77, respectively) acting as the cutoff. Similarly, time to RTA was dichotomized into quick recovery (<3 months) and slow recovery (>3 months) according to the mean value. Based on the classifications in previous literature, 18,28,31 age was divided into older (>40 years) and younger (≤40 years), BMI was classified into 3 groups (<24, 24-27, and ≥27 kg/m2), and time from injury to surgery was defined as delayed (>6 months) and early (≤6 months). The mechanism of injury was divided into acute and nonacute according to the presence of previous known trauma history.
Statistical Analysis
In the univariate analysis, the chi-square test was used to determine the differences in patient and injury characteristics between RTA (fast vs slow) and PRO scores (good vs poor). When the PRO scores were regarded as continuous variables, an independent-samples t test was used. Risk factors with a P value <.1 in the univariate analysis were used in the multivariate analysis. In the multivariate analysis, we used binary regression to determine the independent risk factors for better postoperative outcomes. Statistical analyses were performed with SPSS version 23.0 (IBN Corp). A P value <.05 indicated statistical significance.
Results
From January 2017 to December 2019, 346 patients underwent arthroscopic meniscal surgery in our hospital. After excluding patients who simultaneously received other ligament reconstruction surgery or were lost to follow-up, 215 patients, including 87 men and 128 women with a mean age of 33.7 years (range, 24-75 years), were ultimately included. Of these patients, 204 patients provided the time to RTA. The patient data are shown in Tables 1 and 2.
Patient and Injury Characteristics Stratified by RTA Times a

a Data are presented as n (%). BMI, body mass index; ICRS, International Cartilage Repair Society; RTA, return to activity.
b Included in the multivariate analysis (P < .1).
Patient and Injury Characteristics Stratified by PRO Scores a

a Data are presented as n (%). BMI, body mass index; ICRS, International Cartilage Repair Society; IKDC, International Knee Documentation Committee; PRO, patient-reported outcome.
b Included in multivariate analysis (P < .1).
Time to RTA
The overall time to RTA was 3.3 months (range, 1 week–1.5 years). Preoperatively, 92% of patients had knee-related activity restriction. By 3 months postoperatively, 49.5% (101/204) of patients could perform activities without knee-related restriction; this improved to 69.6% (142/204) at 6 months and 90.2% (184/204) at 12 months. The reasons for the restriction of knee-related activity are listed in Table 3. We found that knee pain was always the main reason hampering patients from doing activities or working at both 6 months and 12 months postoperation.
Reasons for Restricted Knee-Related Activity a

a Data are presented as n (%).
In the univariate analysis, 10 variables were analyzed, and 4 of them were found to be associated with the time to RTA: sex (P = .053), age (P = .052), surgeon experience (P = .08), and injury duration (P = .06). Detailed data are displayed in Table 1. When these 4 variables were analyzed in a multivariate logistic regression model to adjust for confounding factors, we found that age (OR, 0.39; 95% CI, 0.21-1.19; P = .044) and injury duration (OR, 0.20; 95% CI, 0.19-1.07; P = .032) were significantly associated with the time to RTA (Table 4).
Multivariable Analysis of Factors Associated With the Time of Return to Activity a

a ns, nonsignificant.
Knee Functional Scores
The IKDC score improved significantly from 41.2 preoperatively to 76.7 postoperatively, and the Lysholm score improved significantly from 75.4 preoperatively to 94.6 postoperatively. No patients underwent secondary meniscal revision surgery during our study. In the univariate analysis, 10 independent variables were analyzed, and 5 of them were found to be associated with postoperative Lysholm and IKDC scores: sex (P = .054 and P = .004, respectively), age (P = .009 and P = .005), laterality of the meniscal tear (P = .052 and P = .118), BMI (P = .036 and P = .050), and injury mechanism (P = .093 and P = .023). Detailed data are displayed in Table 2. When these variables were analyzed in a multivariate logistic regression model, the results showed that female sex (OR, 3.67; 95% CI, 1.10-6.47; P = .030), BMI ≥27 kg/m2 (OR, 2.96; 95% CI, 1.02-8.66; P = .047), and medial meniscal tear (OR, 0.20; 95% CI, 0.04-1.00; P = .050) were associated with inferior PRO scores (Table 5).
Multivariable Analysis of Factors Associated With the Short-Term Follow-up Clinical Outcomes of Partial Meniscectomy a
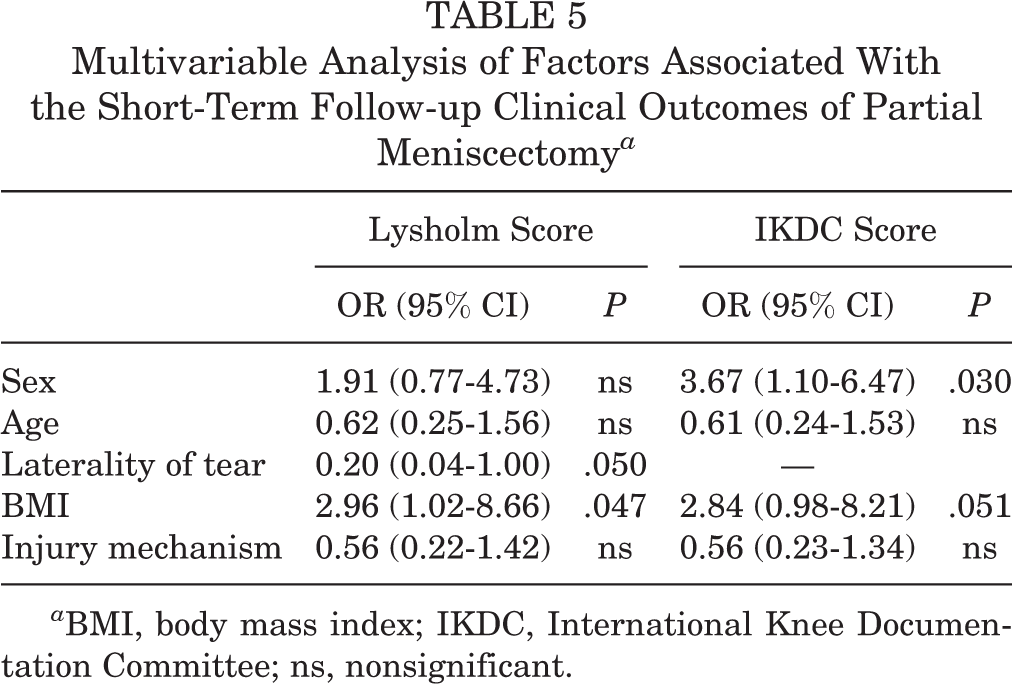
a BMI, body mass index; IKDC, International Knee Documentation Committee; ns, nonsignificant.
Discussion
In the current study, we found that patients aged 40 years and younger and those who underwent partial meniscectomy surgery within 6 months after meniscal tears were 2.56 times (P = .044) and 5.0 times (P = .20) more likely to have a shorter time to RTA, respectively. The second finding was that female patients (P = .030) with obesity (BMI, >27 kg/m2; P.047 = .047), especially those who had a medial meniscal tear (P = .050), tended to have an inferior clinical outcome.
The time to RTA is one of patients’ most concerning questions. However, there is a scarcity of studies investigating the predictive factors associated with a short time to RTA after performing arthroscopic partial meniscectomy. In a study by Aune et al 3 of 72 football players who underwent partial meniscectomy, the authors concluded that speed-position players were 4.0 times less likely to return to play than non–speed-position players, and that no other factors were associated with the time to return to play. However, the authors included only patients with lateral meniscal injury. In another study, Nawabi et al 22 compared the time to return to play among 90 soccer players and found that it was significantly longer after lateral meniscectomy than after medial meniscectomy.
In the aforementioned studies, the participants were professional athletes. However, there are many more nonathletes with meniscal injuries than athletes. Agarwalla et al 2 included 94 nonathletes in their study and found that a higher preoperative KOOS was associated with an increased rate of return to sports. However, the small sample size of their study may have weakened its statistical power. In the current study, we included 204 nonathletes. The mean time to RTA was 3.3 months, which was longer than those reported by Agarwalla et al 2 (2 months) and Lee et al 19 (7-9 weeks). This difference may be explained by the fact that rehabilitation centers are not as common in China as in Western countries; thus, when patients have knee-related symptoms, they are less likely to ask physical therapists for help, which may hinder the rehabilitation process. 20
The influence of the duration of meniscal injury symptoms on the time to RTA has rarely been reported. However, several studies have demonstrated that a shorter injury duration is associated with better postoperative PRO scores. 14,27 Haviv et al 14 concluded that patients with acute meniscal lesions (symptoms existing <3 months) had better improvement in clinical outcomes than those with chronic lesions. The explanation for this is that when partial meniscectomy was delayed, the incidence of secondary chondral damage would increase, which has been shown to be a risk factor for inferior clinical outcomes. 7,29 In our study, 6 months may not be the threshold value of injury duration that can significantly influence PRO scores, but performing surgery for patients within 6 months after meniscal injury can help them RTA quickly. In addition, when patients undergo long-standing nonoperative treatment, their quadriceps femoris muscle may become atrophic, which could negatively affect the rehabilitation process. 10,11
No consensus has been reached on whether older patients are more likely to have inferior clinical outcomes compared with younger patients. 5,6,26 Eijgenraam et al 9 performed a review of factors associated with the clinical outcomes of partial meniscectomy and concluded that 11 studies had investigated the effect of age. Five of the 11 studies found worse outcomes in older patients, and the remaining 6 studies did not find a significant association. In the current study, we found that patients aged 40 years or younger tended to have higher PRO scores, even though the effect became insignificant in the multivariate analysis. However, the time to RTA in the older group was significantly longer than that in the younger group. In a subgroup analysis of patients’ age and chondral lesion (outcomes were not listed), we found that patients aged more than 40 years were 5.21 times more likely to have a severe chondral damage (P < .001). Thus, the knee-related symptoms are less likely to be relieved in older patients because of the concomitant cartilage lesions or osteoarthritis. 30
In our study, we found that a medial meniscal tear was correlated with inferior postoperative clinical outcomes, which is contrary to the findings of a study conducted by Haviv et al. 16 In a study performed by Nawabi et al, 22 they also claimed that lateral meniscal tears were more likely to have adverse events and a slow rehabilitation process. We cannot explain the inconsistent findings between our study and those of previous literature. More studies are needed in the future to evaluate the influence of the laterality of the meniscal tear on clinical outcomes.
The effect of sex on the clinical outcomes after partial meniscectomy was accordant with that reported in previous literature. 16,25 In a study performed by Fabricant et al, 11 the authors found that women had worse knee function, which is consistent with our findings. This can be explained by the fact that women with meniscal tears in our study were older than men (48.1 vs 42.6), which has been reported as a risk factor for worse clinical outcomes. 16 In addition, performing arthroscopic meniscal surgery was more challenging for surgeons because of the smaller joint space in women. However, considering that a substantial number of studies did not find an association of sex with knee function, 9,27 more studies with comparable demographics and clinical characteristics are needed.
BMI has been widely studied in previous literature to investigate its influence on knee function scores. 6,13 In a review study performed by Eijgenraam et al, 9 7 papers observed the effect of BMI, and 5 of them concluded that patients with a BMI >27 kg/m2 are more likely to have worse outcomes, which is consistent with our findings. We explained that a high BMI may increase the stress on the meniscus.
Participation in activities is the priority for many patients. 2 However, studies investigating the predictive factors for a short time to RTA after partial meniscectomy, especially based on nonathletes, are scarce. In our study, we included 204 nonathletes and found 2 independent factors that were associated with the time to RTA, which has seldom been reported in previous literature. In addition, we evaluated the short-term follow-up PRO scores and found 3 variables that were correlated with them. However, most of those risk factors have been reported in other studies. We believe that our findings can provide further evidence for these conflicting opinions.
This study has several limitations. First, selection bias may have been present in terms of participant enrollment because some patients with inferior clinical outcomes may have declined to participate in our phone interview. However, the follow-up rate was relatively high, and the large sample size in our study may reduce the influence of selection bias on clinical outcomes. Second, all patients included in this study were nonathletes; thus, if they could perform low-intensity activities, such as working, walking, and housework, without knee-related restrictions, we regarded them as having reached the standard of return to sports. Consequently, the rate of RTA may be higher and the time to RTA may be shorter than in other studies including professional athletes. However, we believe that return to general activity is the priority for many nonathletes. Third, the time to RTA may not be absolutely accurate, as it depends on patient memory; however, we excluded all patients who were not sure or could not remember the time to RTA.
Conclusion
The mean time to return to sports after arthroscopic partial meniscectomy was 3.3 months. Patients aged 40 or younger, especially those with knee-related symptoms for less than 6 months, were more likely to have a shorter time to RTA. In addition, women with obesity, especially those who have medial meniscal tears, should be preoperatively informed about the greater possibility of having worse short-term clinical outcomes.
Footnotes
Final revision submitted October 8, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Clinical Research Project (grant number: TKKYLC20211203). The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Taikang Xianlin Drum Tower Hospital (ref No. LS20210206).