
Abstract
Background:
Charge and reimbursement trends for arthroscopic partial meniscectomies among orthopaedic surgeons, anesthesiologists, and hospital/surgery centers have not been formally analyzed, even though meniscectomies are the most commonly performed orthopaedic surgery.
Purpose:
To analyze Medicare charge and reimbursement trends for surgeons, anesthesiologists, and hospital/surgery centers for outpatient arthroscopic partial meniscectomies performed in the United States.
Study Design:
Economic and decision analysis; Level of evidence, 4.
Methods:
We analyzed trends in surgeon, anesthesiologist, and hospital charges and reimbursements for outpatient isolated arthroscopic partial meniscectomies from 2005 to 2014. Current Procedural Terminology codes were used to capture charge and reimbursement information using the nationally representative 5% Medicare sample. National and regional trends for charge, reimbursement, and Charlson Comorbidity Index (CCI) were evaluated using linear regression analysis.
Results:
A total of 31,717 patients were analyzed in this study. Charges across all groups increased significantly (P < .001) during the 10-year study period, with an increase of 18.4% ($2754-$3262) for surgeons, 85.5% ($802-$1480) for anesthesiologists, and 116.8% ($2743-$5947) for hospitals. Surgeon reimbursements declined by 15.5% ($504-$426; P = .072) during this period. Anesthesiologist and hospital reimbursements increased significantly during by 36.5% ($133-$182; P < .001) and 28.9% ($1540-$1984; P < .001) during the 10-year study period, respectively. The annual incidence of partial meniscectomies per 10,000 database patients decreased significantly from 18.3 to 15.6 over the course of the study (14.8% decrease; P = .009), while the CCI did not change significantly (P = .798).
Conclusion:
Hospital and anesthesiologist Medicare reimbursements for outpatient arthroscopic partial meniscectomies increased significantly, while surgeon reimbursements decreased. In 2005, hospitals were reimbursed 205% more ($1540 vs $504) than surgeons, and by 2014, they were reimbursed 365% more ($1984 vs $426), indicating that the gap between hospital and surgeon reimbursement is rising. Improved understanding of charge and reimbursement trends represents an opportunity for key stakeholders to improve financial alignment across the field of orthopaedics.
Keywords
An estimated 700,000 arthroscopic partial meniscectomies are performed annually in the United States, making it the most commonly performed orthopaedic surgery in the country. 18,29 Unsurprisingly, there has been an increased focus on the economics of arthroscopic partial meniscectomies given the sheer volume and the estimated $4 billion in annual direct costs 29 in the United States associated with performing these operations. 11,21,24,29 Health care costs represent a significant concern to Americans, and it is expected that national health expenditures will increase to 19.4% of the US gross domestic product by 2027. 30
While health care spending continues to rise dramatically, 4,17,22 Medicare reimbursements for orthopaedic surgeons have been declining for many procedures, with an inflation-adjusted average decline of 28% for the top 25 most commonly performed orthopaedic surgeries from 1998 to 2007. 13 Medicare reimbursements also decreased between 2000 and 2016 for the majority of the most common orthopaedic surgeries. 11 While orthopaedic surgeon payments have decreased, or stayed the same, for many common procedures, hospital payments have increased considerably.
Charge and reimbursement trends for arthroscopic partial meniscectomies among orthopaedic surgeons, anesthesiologists, and hospital/surgery centers have not been formally analyzed, even though it is the most commonly performed orthopaedic surgery. 18,29 The purpose of this study was to analyze regional and national Medicare charge and reimbursement trends for surgeons, anesthesiologists, and hospital/surgery centers for outpatient arthroscopic partial meniscectomies performed in the United States. It was hypothesized that hospital reimbursements for partial meniscectomies would rise significantly, while surgeon and anesthesiologist reimbursements would not.
Methods
The PearlDiver database (http://pearldiverinc.com) was retrospectively queried to identify patients who underwent outpatient isolated arthroscopic meniscectomy between 2005 and 2014. Specifically, the 5% Medicare Standard Analytical Files were analyzed. These are a nationally representative sample of 5% of all 51 million Medicare patients, and it is the only file that contains complete charge and reimbursement data for surgeons, anesthesiologists, and hospital/surgery centers. 28 The files also include important pertinent information including patient characteristics, diagnoses, procedures, and Current Procedural Terminology (CPT) codes. The most recent complete 10-year set of charge and reimbursement data in the PearlDiver Medicare system was from 2005 to 2014.
Patients who underwent outpatient arthroscopic partial meniscectomies were identified by searching for the CPT codes 29880 (arthroscopy, knee, surgical; with meniscectomy [medial AND lateral, including any meniscal shaving]) and 29881 (arthroscopy, knee, surgical; with meniscectomy [medial OR lateral, including any meniscal shaving]). Five anesthesia CPT codes were analyzed: 01382, anesthesia for arthroscopies of the knee joint; 01320, anesthesia for procedures on the knee or popliteal area; 01400 and 01402, anesthesia for open or arthroscopic procedures on the knee joint; and 99100, qualifying circumstances for anesthesia, age >70 years. Additional surgical CPT codes (29866, 29867, 29868, 29871, 29882, 29883, 29884, and 29885) were used to exclude patients who had infections or underwent concomitant procedures beyond an isolated partial meniscectomy, such as osteochondral allograft transfer, meniscal repair, lysis of adhesions, bone grafting, or ligamentous reconstruction. Medicare uses CPT codes only for outpatient procedures, so CPT codes were used to define charges and reimbursements in this study.
Exclusion criteria included patients with additional concomitant procedures as well as patients with incomplete charge or reimbursement data (physician CPT codes and surgery center CPT codes). Patients who underwent inpatient meniscectomy were also excluded because of the increased costs associated with an inpatient stay. Financial data were compiled by filtering CPT codes to separate physician and surgical center charges and reimbursements. Characteristic information including patient age range, sex, geographic region, Charlson Comorbidity Index (CCI), 6 and the number of meniscectomies per year were also collected (Table 1). For geographic regions, patients were separated into 4 regions: Northeast, South, Midwest, and West. The data in this study were publicly available and deidentified; therefore, institutional review board approval was not needed.
Arthroscopic Partial Meniscectomy Characteristics by Year a

a Data are reported as n (%) unless otherwise indicated. CCI, Charlson Comorbidity Index.
b Difference between years was not significant (P = .798).
Linear regression analysis was used to compare trends using JMP Pro (V14.1.0; SAS Institute). Two ratios, the charge multiplier and the payment multiplier, were calculated to compare differences in charge and reimbursement trends between surgeons and hospitals. 5,19 The charge multiplier ratio is the ratio of surgeon charges to hospital/surgery center charges, and the payment multiplier ratio is the ratio of surgeon reimbursements to hospital/surgery center reimbursements. This method of comparing charge multiplier and payment multiplier has been previously described in the literature as a way to control for inflation and regional differences. 5 Linear regression analysis was used for statistical analyses, and P values < .05 were considered to represent statistical significance.
Results
There were 34,251 patients initially analyzed; however, 2534 of those patients were excluded due to incomplete charge and reimbursement data. This resulted in a final count of 31,717 patients who met all inclusion criteria for this study. Data regarding patient characteristics, CCI, and volume of arthroscopic partial meniscectomies are listed in Table 1. The CCI did not change significantly during the 10-year period (P = .798). The annual incidence of partial meniscectomies per 10,000 database patients decreased significantly from 18.3 to 15.6 over the course of the study (14.8% decrease; P = .009).
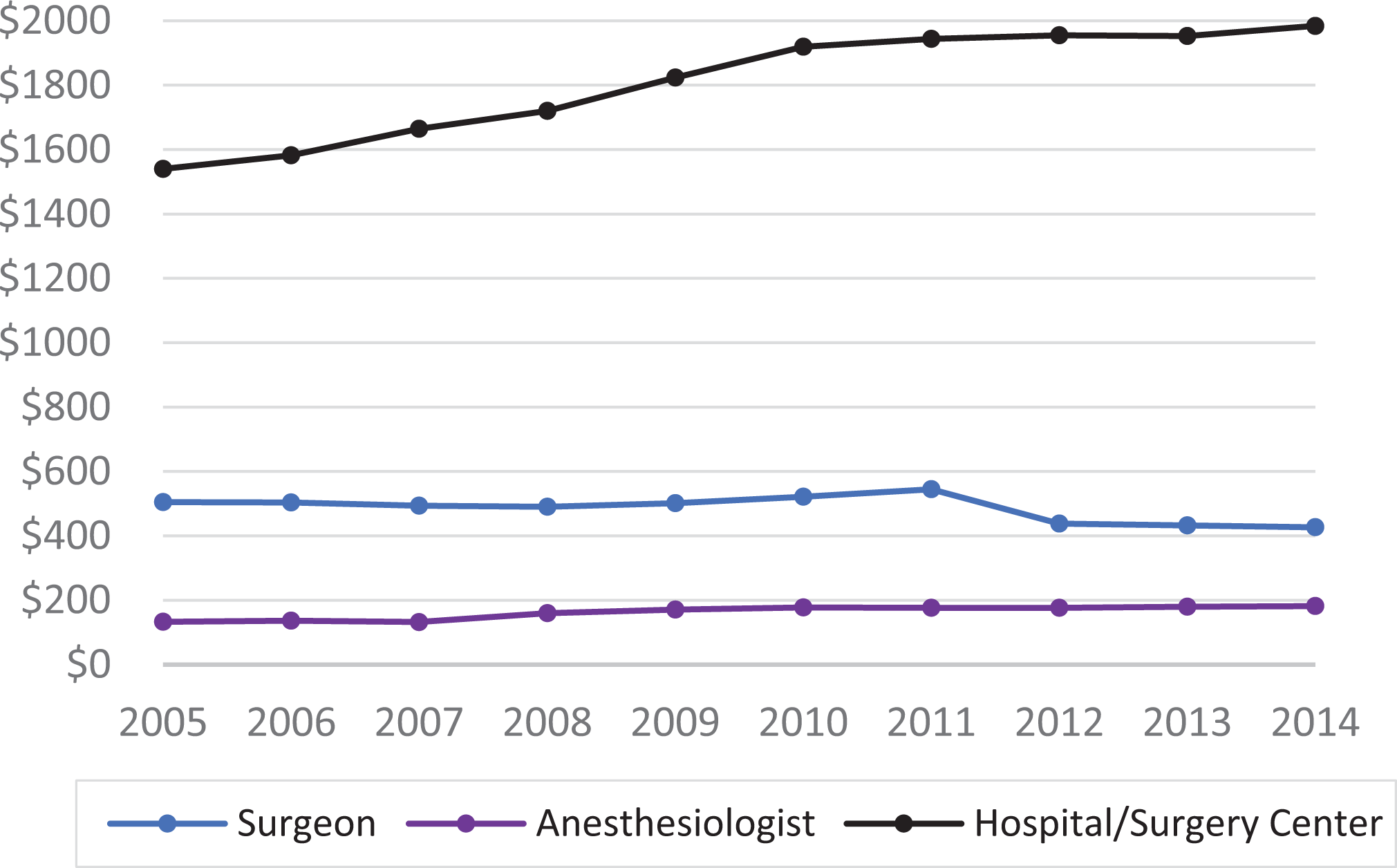
Charges across all groups (surgeons, anesthesiologists, and hospital/surgery centers) increased significantly during the 10-year period (P < .001) (Figure 1, Table 2). Surgeon charges increased from $2754 to $3262 (18.4% increase), anesthesiologist charges increased from $802 to $1480 (85.5% increase), and hospital/surgery center charges increased from $2743 to $5947 (116.8% increase) (Table 2). Hospitals charges were 0.4% lower than surgeon charges in 2005. By 2014, hospital charges were 82.3% higher than surgeon charges.

Mean charges for outpatient arthroscopic partial meniscectomy for surgeons, anesthesiologists, and hospital/surgery centers (2005-2014). Charges increased significantly across all groups (P < .001).
Charge and Reimbursement Data for Outpatient Partial Meniscectomy From 2005 to 2014 a

a Bolded P values indicate statistically significant change during the study period. Negative data indicate declines during the study period.
Surgeon reimbursements declined from $504 to $426 (15.5% decline; P = .072) (Figure 2, Table 2). Reimbursements increased significantly for anesthesiologists (from $133 to $182 [36.5%]; P < .001) and hospitals (from $1540 to $1984 [28.9%]; P < .001). Hospitals were reimbursed 205.3% more than surgeons in 2005, a number that rose to 365.4% in 2014. The total episode of care (surgeon, anesthesiologist, and hospital/surgery center reimbursements) increased from $2177 to $2593 (19.1% increase).
Mean reimbursements for outpatient arthroscopic partial meniscectomy for surgeons, anesthesiologists, and hospital/surgery centers. Reimbursements declined for surgeons (P = .072). Reimbursements for anesthesiologists and hospital/surgery centers each increased significantly (P < .001).
The charge multiplier increased from 1.0 to 1.8 (P < .001) and the payment multiplier increased from 3.1 to 4.7 (P < .001) between 2005 and 2014 (Figure 3). Regional data were compared using the charge multiplier (Figure 4) and the payment multiplier (Figure 5). The West region had consistently higher charge multiplier values compared with the other regions. In comparison, the payment multiplier values were more uniform during the 10-year period.
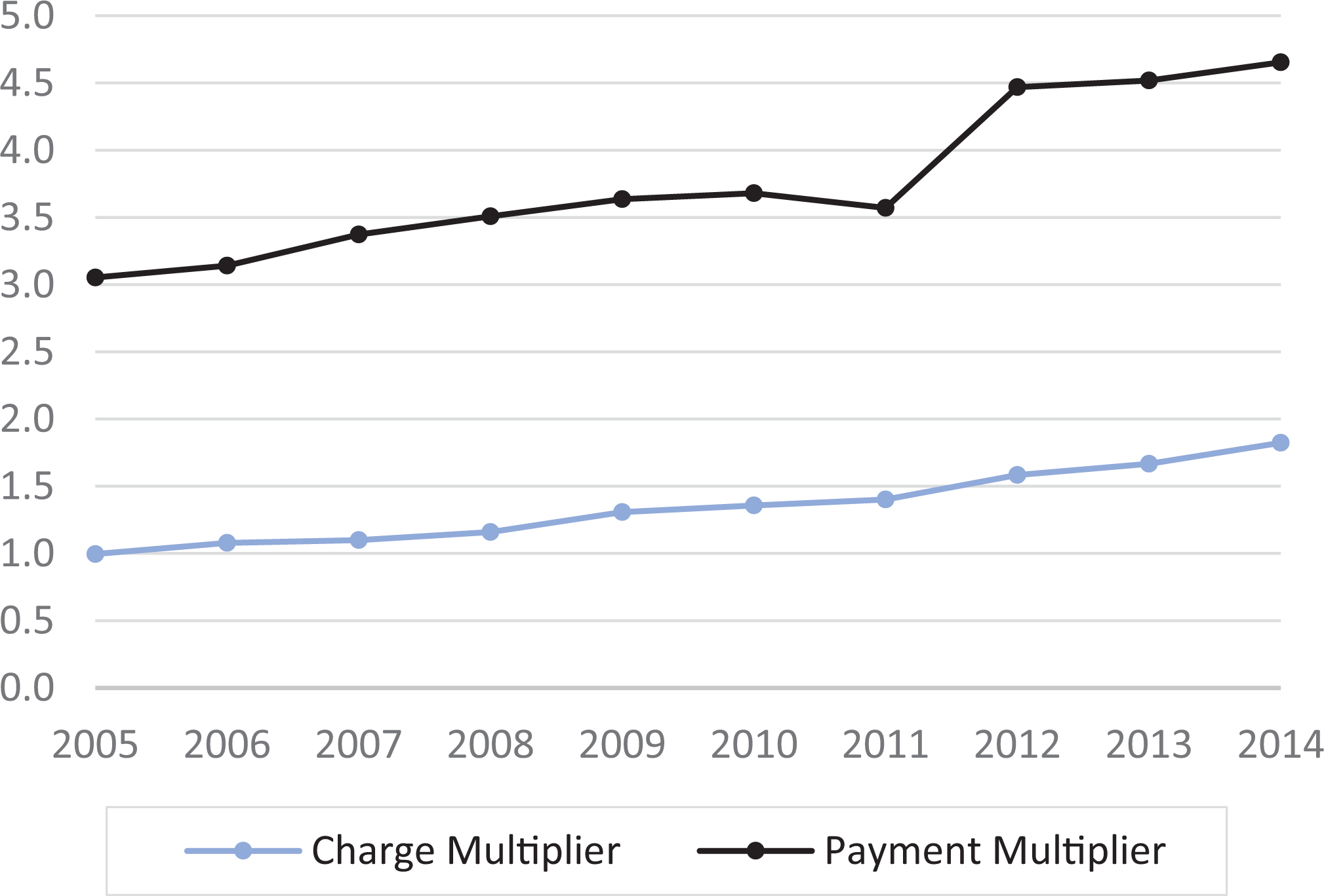
Nationwide trends for the charge and payment multipliers are illustrated. The charge multiplier is a ratio that compares hospital and surgeon charges, while the payment multiplier is a ratio that compares hospital and surgeon payments. Increases in the charge multiplier and payment multipliers were both significant (P < .001).

Regional trends for the charge multiplier are depicted. The charge multiplier is a ratio that compares hospital with surgeon charges. Increases in the charge multiplier were significant for all 4 regions (P < .001). MW, Midwest; NE, Northeast; SO, South; WE, West.
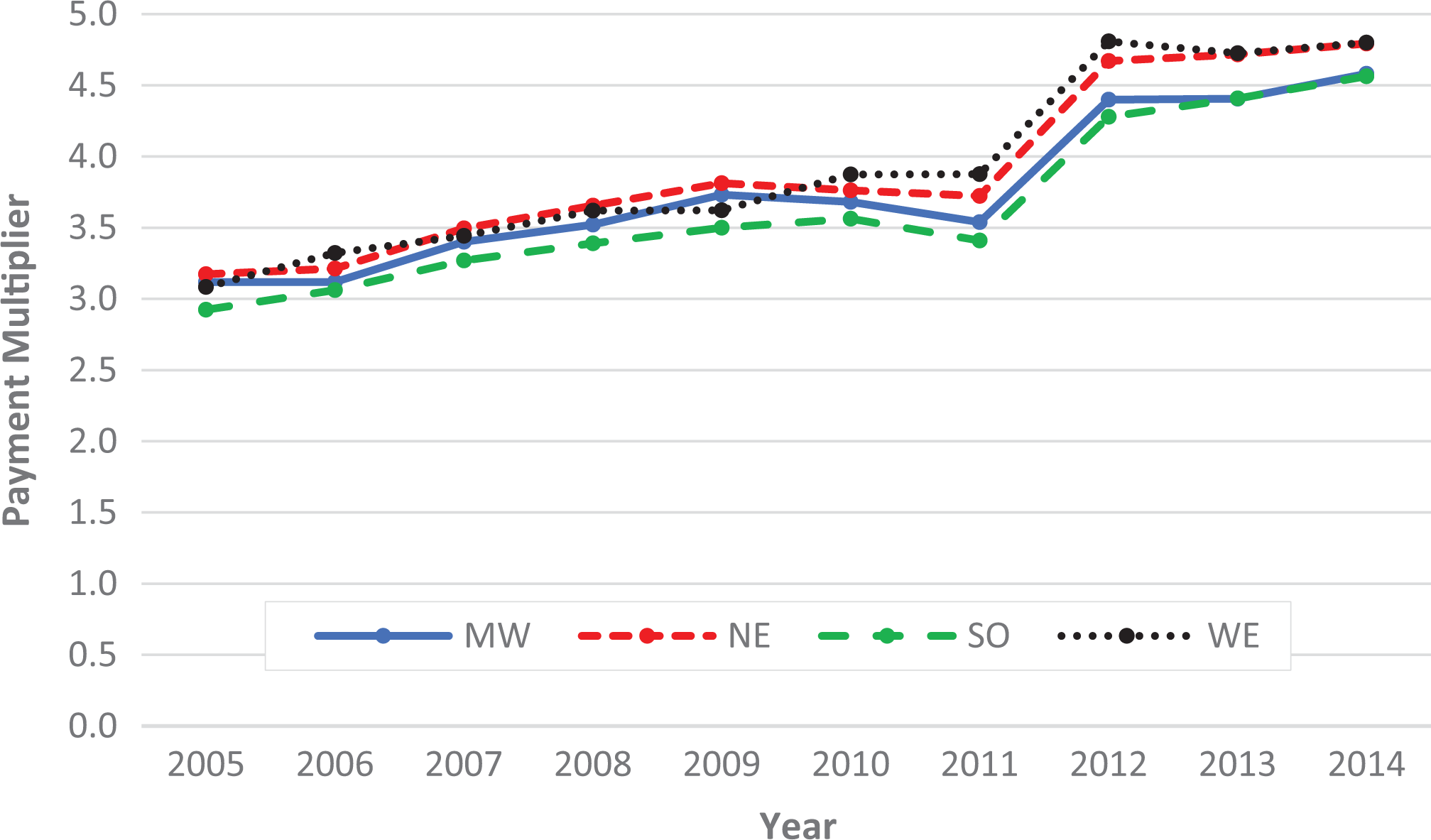
Regional trends for the payment multiplier are depicted. The payment multiplier is a ratio that compares hospital with surgeon reimbursements. Increases in payment multiplier were significant for all 4 regions (P < .001). MW, Midwest; NE, Northeast; SO, South; WE, West.
Discussion
The most important finding of this study was that outpatient arthroscopic partial meniscectomy reimbursements increased significantly for anesthesiologists and surgery centers while surgeon reimbursements decreased. Arthroscopic partial meniscectomy charges increased significantly across all groups, with larger increases for anesthesiologists and hospital/surgery centers. Hospitals observed their charges increased by 116.8% compared with 18.4% for surgeons, and their reimbursements increased by 28.9% compared with a 15.5% decrease for surgeons, which is highlighted by the significant increases in the charge and payment multipliers, respectively. These multipliers help control for inflation, and the significant increase demonstrates that the gap between charges and reimbursements between hospitals and surgeons grew during this period.
It is unclear what factors drove the charge increase of 116.8% for hospital/surgery centers and why the charges increased at significantly higher rates than surgeons (18.4% increase). Unlike the hospital and anesthesiologist charges, surgeon charges rose at a rate that was slightly below the inflation rate reported by the US Bureau of Labor Statistics of approximately 21% during this period. 32 It has been hypothesized that increases in the cost of materials/implants, 23,34 overhead, 8 the number of nonclinical hospital administrators, and rising hospital executive compensation could be important drivers of increased health care costs. 4,9,14,27 Isolated partial meniscectomies do not require the use of implants; however, material costs or higher overhead costs could contribute to these increased costs. Hospital administration costs represented 25.3% of all health care–related costs in 2011, a number that was more than double the rate in Canada. 14 Although it is not clear from these data, the significant increases in anesthesiologist charges (86%) and reimbursements (37%) are likely multifactorial and related to variability in the use of regional blockades, increased clerical burdening of pre- and postoperative evaluations, or increased need to reimburse support staff. Even though the increase in reimbursements was significant, the absolute increase in reimbursement was modest (from $133 to $182). There was a noticeable 1-time increase in hospital charges between 2011 and 2012. It is unclear what drove this increase; however, it may be related to the relative value unit decrease for the 2 surgical CPT codes (29880 and 29881) used in the study. 10
When compared with other surgical subspecialties, orthopaedic reimbursements have been reported to be declining at a greater rate. 11 Orthopaedic surgeons are being reimbursed less while balancing increased responsibilities tied to bundled payments, readmission penalties, and a multitude of quality metrics. 7,20 Conversely, hospital CEO compensation increased by 93% between 2005 and 2015 during a period of decreased Medicare orthopaedic surgeon reimbursement. 9,11 While surgeon reimbursement is becoming more heavily tied to patient outcomes, 7,20 hospital CEO salaries have not been reported to be positively associated with improved patient outcomes, quality performance, or hospital margins. 9,15 Lack of “physician-hospital alignment” in the orthopaedic community is often centered on financial issues. 20,25 Improving alignment between surgeons and hospitals has been shown to improve quality and reduce costs in the setting of total hip and knee arthroplasty. 8
This study also found that the combined payments to surgeons, anesthesiologists, and hospitals increased over time despite decreases in surgeon reimbursement. Marrache et al 20 showed that decreases in surgeon reimbursement for 4 orthopaedic procedures did not lead to decreases in net payment for the episodes of care because of increased hospital payments. 20 It is likely that solely reducing physician reimbursement will not stem rising operative costs on its own. Increased transparency regarding rising hospital charges and payments could present an opportunity for shared decision making between surgeons and administrators to reduce unnecessary costs.
The total number of outpatient arthroscopic partial meniscectomies performed on Medicare patients declined significantly between 2005 and 2014. This is in alignment with previous studies 2,31 that have reported that the total number of arthroscopic partial meniscectomies decreased slightly after reaching a peak in 2010. This could be due to a multitude of factors, including increases in meniscal repairs and transplants, 2,31 concerns regarding the cost-effectiveness of the operation, 16,21 and the overall effectiveness of arthroscopic partial meniscectomy compared with physical therapy. 33 Meniscal repairs have increased significantly over the past 10 years because repair techniques have improved and because meniscal repair better preserves the knee joint compared with meniscectomy in appropriately selected patients. 26,31
Physician reimbursement will continue to be an important topic. The comorbidity burden is expected to rise in the United States, and the total number of Medicare patients continues to grow as the American population ages. 11,20 Medicare reimbursements are often used as benchmarks for private insurance reimbursement rates, so it is important to understand Medicare trends. 11,13 Future policy changes will likely affect physician reimbursements, 24 such as the recently announced Centers for Medicare and Medicaid Services’ proposed reduction of all orthopaedic surgery fees by approximately 5% for the 2021 calendar year. 1 Understanding the true cost of care is crucial to improving “physician-hospital alignment” 8 and allows decision makers to identify areas for cost reductions in a shared manner for all orthopaedic procedures. This study used charge data as a surrogate for cost, because the true cost of care is not widely reported by institutions and is difficult to calculate given the complexity and variability of the current health system. It is crucial that key stake holders be aware of trends regarding charge and reimbursement among surgeons, anesthesiologists, and hospitals so that they are able to make informed and sustainable financial decisions.
There were some limitations to this study that warrant discussion. Given the retrospective nature of the study, we relied on the assumption that the database’s CPT data were accurate; however, errors on the part of those performing the original coding and data entry could alter the accuracy of this study’s findings. It is important to note that this study analyzed only isolated meniscectomies, which excludes partial meniscectomies performed concomitantly with other procedures such as ligamentous reconstruction, realignment surgery, cartilage restoration, and other arthroscopic knee procedures. This may introduce some bias into the results. This study analyzed only Medicare patients, which limits the generalizability to private payors. A major limitation of the Medicare database is that the majority of patients are >65 years old, which limits the ability to study national charge and reimbursement trends for operations that are typically reserved for younger patients (ie, meniscal repairs). A recent retrospective analysis of 649,470 New York State patients undergoing meniscal procedures found that there were much higher numbers of privately insured patients compared with Medicare patients. 31 To our knowledge, there has not been a national comparison of the number of privately insured patients versus Medicare patients. Privately insured partial meniscectomy patients are likely younger and likely represent a larger volume of patients than the Medicare population; therefore, further analysis of the trends associated with privately insured patients is recommended. The cost-ineffectiveness of arthroscopic partial meniscectomies is well-established in the literature 3,29 ; however, the analysis of more cost-effective joint-preserving procedures such as meniscal repairs 12 was limited by patient age in the Medicare database because meniscal repair is typically reserved for younger patients.
Conclusion
Hospital and anesthesiologist Medicare reimbursements for outpatient arthroscopic partial meniscectomies increased significantly while surgeon reimbursements decreased. In 2005, hospitals were reimbursed 205% more ($1540 vs $504) than surgeons, and by 2014, they were reimbursed 365% more ($1984 vs $426), indicating that the gap between hospital and surgeon reimbursement is rising. Improved understanding of charge and reimbursement trends represents an opportunity for key stakeholders to improve financial alignment across the field of orthopaedics.
Footnotes
Final revision submitted December 7, 2020; accepted January 25, 2021.
This article’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). M.D.L. has a family member with the following disclosures: royalties and consulting fees from Arthrex and Ossur; consulting fees from Linvatec; and royalties, consulting fees, speaker fees, and research support from Smith & Nephew and Thieme. C.L.C. has received education payments and nonconsulting fees from Arthrex. A.J.K. is a board member for MTF and has received consulting fees, speaking fees, and royalties from Arthrex; consulting fees from JRF Ortho and Responsive Arthroscopy; and honoraria from Vericel and JRF Ortho. B.C.W. has received research support from Exactech, Flexion, and Biomet; education payments, consulting fees, and nonconsulting fees from Arthrex; hospitality payments from Integra LifeSciences; and education payments from Supreme Orthopedic Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.