
Abstract
Background:
Increased posterior tibial slope (PTS) is a risk factor for anterior cruciate ligament (ACL) rupture and failure of ACL reconstruction (ACLR) grafts.
Purpose:
The purpose was to conduct a systematic review of literature on PTS measurements and to conduct a meta-analysis of comparable PTS measurements based on a patient’s ACL status. It was hypothesized that patients with torn ACLR grafts would have significantly larger medial and lateral PTS compared with patients with native ACLs or those who underwent primary ACLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Included were studies that reported medial and/or lateral PTS measurements, those that reported PTS measurements based on ACL status (ie, intact ACL, primary ACL tear, failed ipsilateral ACLR, or revision ACLR), and those that reported their specific PTS measurement technique. Average PTS measurements, measurement location (medial or lateral tibial plateau) and technique, imaging modality used, and ACL status were extracted from each study. Data were pooled using DerSimonian and Laird random-effects models, and results were compared using the Altman interaction test.
Results:
The literature search identified 1705 studies, of which 82 (N = 12,971 patients) were included. There were 4028 patients in the intact ACL group (31%), 7405 in the primary ACLR group (57%), and 1538 in the failed ACLR group (12%). Measurements were obtained from lateral radiographs in 31 studies (38%), from magnetic resonance imaging in 47 studies (57%), and from computed tomography in 4 studies (5%). The failed ACLR group had a significantly larger lateral PTS (9.55°; 95% CI, 8.47°-10.63°) than either the primary ACL tear (7.13°; 95% CI, 6.58°-7.67°) or intact ACL (5.57°; 95% CI, 5.03°-6.11°) groups (P < .001 for both). The failed ACLR group also had a significantly larger medial PTS (9.05°; 95% CI, 7.80°-10.30°) than the primary (6.24°; 95% CI, 5.71°-6.78°) or intact ACL (6.28°; 95% CI, 5.21°-7.35°) groups (P < .001 for both).
Conclusion:
Both lateral and medial PTS measurements were greater in patients who had failed previous ACLR than those with a primary ACL tear or an intact native ACL. The lateral PTS of patients with primary ACL tears was greater than those with an intact native ACL.
Keywords
Posterior tibial slope (PTS) is an important radiographic measurement that is defined by the sagittal angulation of the tibial plateau relative to the tibial shaft. 68 Biomechanical data suggest that anatomic variations in PTS can significantly alter biomechanical knee stability; studies have reported a linear relationship between the PTS and the amount of tension placed on native cruciate ligaments and reconstructed cruciate grafts. 7,8,49,98 Previous case series have reported that patients with primary anterior cruciate ligament (ACL) tears have steeper PTS. 58,104 Others have shown that patients with graft rupture after previous ACL reconstruction (ACLR) have greater PTS than those undergoing primary ACLR. 72,86 To protect reconstruction grafts from variations in PTS, some authors advocate the use of slope reducing, anterior closing-wedge high tibial osteotomy. 22,24,27
Measurement strategies include a variety of imaging modalities, such as standard lateral radiographs, long-leg lateral radiographs, magnetic resonance imaging (MRI), and computed tomography (CT), in addition to several different techniques including utilization of the anatomic or mechanical axis or the anterior or posterior cortex. 23,32,39,47,64,66,76,100 Previous reports have demonstrated that increases in PTS, by as little as 2°, places a clinically significant amount of increased strain on the ACL. 18
Despite numerous case series and biomechanical studies that evaluated PTS in patients with ruptured ACLs and those undergoing revision or rerevision ACLR, there are few comprehensive reviews comparing the PTS of patients with ACL pathology. As such, the purpose of the current analysis was to conduct a systematic review of literature on PTS measurements and to conduct a meta-analysis of comparable PTS measurements based on patients' ACL status/integrity (intact ACL, primary ACL tear, failed ACLR). It was hypothesized that patients with torn ACLR grafts would have significantly larger medial and lateral PTS compared with patients with native ACLs or those with primary ACLRs.
Methods
Article Identification and Selection
A systematic review was completed using the PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines on the PTS of patients undergoing primary and revision ACLR; the query was performed in May 2021 (Figure 1). The specific search terms were “Tibial Slope” AND “ACL” OR “PTS” AND “ACL” OR “Tibial Slope” AND “Revision” OR “Anterior Cruciate Ligament” AND “Revision.” This systematic review was registered in May 2021 using the PROSPERO international prospective register of systematic reviews (registration No. CRD42021256743).

PRISMA flowchart demonstrating the article selection process. ACL, anterior cruciate ligament; PRISMA Preferred Reporting Items for Systematic Meta-Analyses; PTS, posterior tibial slope.
The inclusion criteria for studies in both the systematic review and meta-analysis consisted of the following: studies written in English, studies that reported either medial or lateral PTS, studies that reported PTS measurements based on the status of a patient’s ACL (ie, intact ACL, primary ACL tear, failed ACL ipsilateral reconstruction, or revision ACLR), studies that reported their PTS measurement technique, and studies that were published during or after the year 2000. Measurements for the intact ACL group were obtained from patients who had non-ACL pathologies. These measurements were not obtained from the contralateral limb of patients with ACL tears. Exclusion criteria were ACL studies that did not include PTS measurements; studies that failed to describe the ACL status; studies that failed to differentiate measurement location (medial vs lateral PTS) or technique of PTS measurement; studies that failed to report measures of variance (eg, standard deviation or confidence interval); case studies with level V evidence; any study published before the year 2000; studies that used or compared multiple measurement techniques; studies that included posterior cruciate ligament injuries; and biomechanical, in vitro, or animal model studies. Studies that included both revision and primary ACLRs in the same cohort were not included in the meta-analysis portion of the current study. Two investigators (R.S.D., N.N.D.) independently reviewed the abstracts from all identified articles. If necessary, full-text articles were obtained for review to allow further application of the established inclusion and exclusion criteria. In addition, reference lists from the included studies were reviewed and reconciled to verify that all eligible articles were considered.
Data Extraction
The variables of interest that were extracted from each study included average PTS measurements, PTS measurement location (medial or lateral PTS), imaging modality used to measure PTS, PTS measurement technique, indications for knee imaging (for intact cohort), country of origin of study, and primary versus revision ACL tear. In addition, descriptive article information and patient demographics were extracted and recorded from each study. The country of origin was defined by the corresponding authors' listed country. Some studies separated their cohorts into subgroups that were unable to be combined; these included groupings by sex, laterality (unilateral vs bilateral), outcomes (superior vs inferior), PTS (high vs low), and laxity (high vs low). These studies were therefore included as separate entries in the meta-analysis. Patients were grouped into 1 of 3 cohorts: intact ACL, primary ACL tear, or failed ACLR. Demographic variables, country of origin, PTS measurement technique, PTS measurement modality, and article descriptive information were not evaluated in the meta-analysis portion of the current study but were reported in the systematic review. Measurement modalities were grouped into radiographs, MRI, or CT.
The measurement techniques were grouped into 1 of 4 categories, each of which has been described previously in the literature (Figure 2). The first technique used MRI and measured the vertical component of the PTS measurement using the midpoint of parallel horizontal lines at least 4 cm apart and distal in the image. 39 The second technique utilized a sagittal MRI slice to place 2 circles: a superior circle touching the anterior, posterior, and superior cortex of the tibia, and an inferior circle touching the anterior and posterior cortex. 47,77 A vertical line was then drawn between the midpoint of both circles to establish the longitudinal component of the measurement. The third technique utilized standard radiographs. 3,10,35 Points at 5 and 15 cm distal to the joint line on both the anterior and posterior tibial cortices were identified. The midpoint between the respective anterior and posterior points were then established. These midpoints were connected with a vertical line to establish the longitudinal axis of the PTS calculation. The fourth category included all other techniques, which included an adaptation of the circle measurement technique on standard radiographs, all measurements obtained on CT images, and techniques that considered the anterior or posterior tibial cortex exclusively. Based on previous studies, the minimal clinically significant difference (MCID) for PTS was defined as ≥2°, 18 which represents the difference in measurements between the different locations (medial vs lateral).
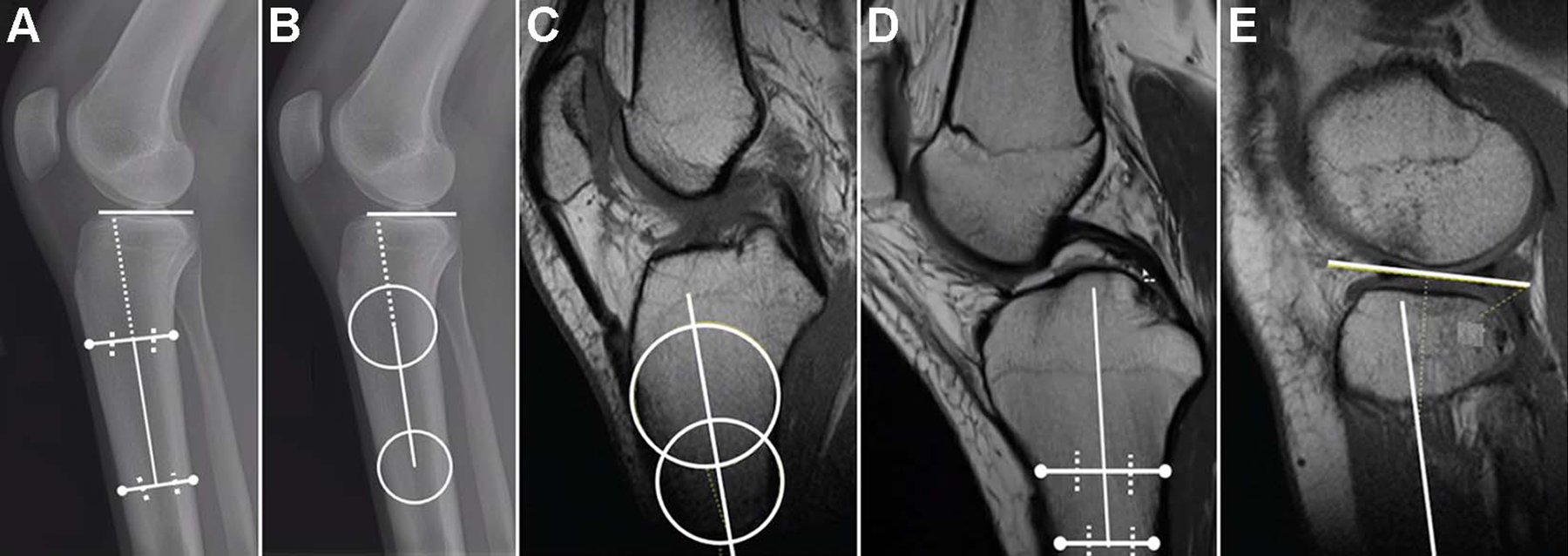
Illustrations of the PTS measurement methods considered in the current review. (A) Midpoint lines technique for measuring lateral PTS on standard radiographs previously described by Brandon et al. 13 (B) Circles measurement technique on lateral radiographs by Vyas et al. 102 (C) Circles measurement technique for establishing the vertical, anatomic axis component of the PTS measurement technique on MRI described by Hudek et al. 47 (D) Midpoint lines technique for identifying the anatomic axis of the PTS measurement technique on MRI described by Hashemi et al. 39 (E) Technique to identify the horizontal component of the lateral PTS, which is used concurrently with the techniques shown in either (C) or (D) to determine lateral PTS. MRI, magnetic resonance imaging; PTS, posterior tibial slope.
Risk-of-Bias Evaluation
All studies were reviewed for bias using the previously reported Methodological Index for Non-Randomized Studies (MINORS) tool. 89 The MINORS tool includes 12 questions to assess quality, 4 of which are applicable only to those studies that are comparative. Each of the 12 items was scored 0 to 2: 0, not reported; 1, reported but described or performed poorly or inadequately; 2, reported accurately and well described. Higher scores are associated with a lower risk of bias. Scores of at least 75% were considered high quality with low risk for bias; scores between 50% and 75% were considered medium risk for bias; scores of less than or equal to 50% were considered high risk for bias. For noncomparative studies, the maximum score was 16, 16 while the maximum score for comparative studies was 24.
Statistical Analysis
Extracted and pooled outcomes of interest and related standard error were calculated using DerSimonian and Laird random effects models. Heterogeneity between studies was quantified using the I 2 statistic, in which an I 2 value of greater than 75% was used to indicate high heterogeneity. Random-effects models were used for all analyses. The difference between PTS measurements for each subgroup was conducted using the Altman interaction test. Two-tailed P values < .05 were determined to be statistically significant. All statistical analyses were conducted using open-source R software, version 4.0.5. Forest plots were created using OpenMetaAnalyst (Brown University) using the R console package.
Results
The literature search identified 1705 unique studies, of which 82 were included in the final systematic review and meta-analysis (Figure 1). There were 40 studies that reported the PTS of patients with intact ACLs (Table 1), 65 studies that reported the PTS of patients with primary ACL tears (Table 2), and 18 studies that reported the PTS of at least 1 failed ipsilateral ACLR (Table 3).
Demographics and Measurement Variables for Intact ACL Cohort a

a ACL, anterior cruciate ligament; F, female; M, male; MRI, magnetic resonance imaging; NA, not available; PTS, posterior tibial slope.
b The numbers in parentheses correspond to the various measurement techniques: (1) midpoint lines technique using MRI; (2) circles technique using MRI; (3) midpoint lines using standard radiographs; (4) other (combination of circles on radiographs, posterior tibial cortex, anterior tibial cortex).
Demographics and Measurement Variables for Primary ACL Tear Cohort a

a ACL, anterior cruciate ligament; CT, computed tomography; F, female; M, male; MRI, magnetic resonance imaging; NA, not available; PTS, posterior tibial slope.
b The numbers in parentheses correspond to the various measurement techniques: (1) midpoint lines technique using MRI; (2) circles technique using MRI; (3) midpoint lines using standard radiographs; (4) other (combination of circles on radiographs, posterior tibial cortex, anterior tibial cortex).
Demographics and Measurement Variables for Revision ACL Tear Cohort a

a ACL, anterior cruciate ligament; F, female; IQR, interquartile range; M, male; MRI, magnetic resonance imaging; NA, not available; PTS, posterior tibial slope.
b The numbers in parentheses correspond to the various measurement techniques: (1) midpoint lines technique using MRI; (2) circles technique using MRI; (3) midpoint lines using standard radiographs; (4) other (combination of circles on radiographs, posterior tibial cortex, anterior tibial cortex).
In total, there were 12,971 patients, including 4028 (31%) patients in the intact ACL group, 7405 (57%) in the primary ACLR group, and 1538 (12%) in the failed ACLR group. There were 22 studies (27%) that reported only the medial PTS, 15 studies (18%) that reported only the lateral PTS, and 45 studies (55%) that reported both medial and lateral PTS.
The mean age range of included patients was 13.1 to 51.6 years. 74,114 Among the included studies, 31 (38%) reported measurements obtained from lateral radiographs, 47 (57%) reported measurements obtained from MRI, and 4 (5%) reported measurements obtained from CT. The measurement techniques reported were as follows: studies that used the midpoint lines technique on MRI (n = 26), studies that used the midpoint lines technique on standard radiographs (n = 17), and studies that used the circles technique on MRI (n = 23). There were also 2 studies that used the anterior tibial cortex 19,97 and 3 studies that used the posterior tibial cortex for their measurement techniques. 43,44,86
Results of Meta-Analysis
The average medial and lateral PTS for each subgroup is shown in Table 4, and forest plots for each analysis are provided as supplemental material. The meta-analysis demonstrated that the failed ACLR group had the largest average lateral PTS (9.55°; 95% CI, 8.47°-10.63°) (Supplemental Figure S1), followed by the primary ACL tear group (7.13°; 95% CI, 6.58°-7.67°) (Supplemental Figure S2) and the intact ACL group (5.57°; 95% CI, 5.03°-6.11°) (Supplemental Figure S3). The differences between each of these means were found to be significant (P < .001) for each possible interaction (ie, intact ACL vs primary ACL tear, intact ACL vs revision ACL tear, primary ACL tear vs failed ACLR). An additional analysis demonstrated that the failed ACLR group had a significantly larger medial PTS (9.05°; 95% CI, 7.80°-10.30°) than the primary (6.24°; 95% CI, 5.71°-6.78°) or intact ACL (6.28°; 95% CI, 5.21°-7.35°) groups (P < .001) (Supplemental Figures S4-S6). The difference between mean medial PTS measurements from both the intact ACL and primary ACL groups compared with the failed ACLR group was found to be statistically significant (P < .001). The difference in mean medial PTS between the intact ACL and primary ACL groups was not statistically significant (6.28° vs 6.24°, respectively; P = .948).
Medial and Lateral PTS Depending on ACL Status a
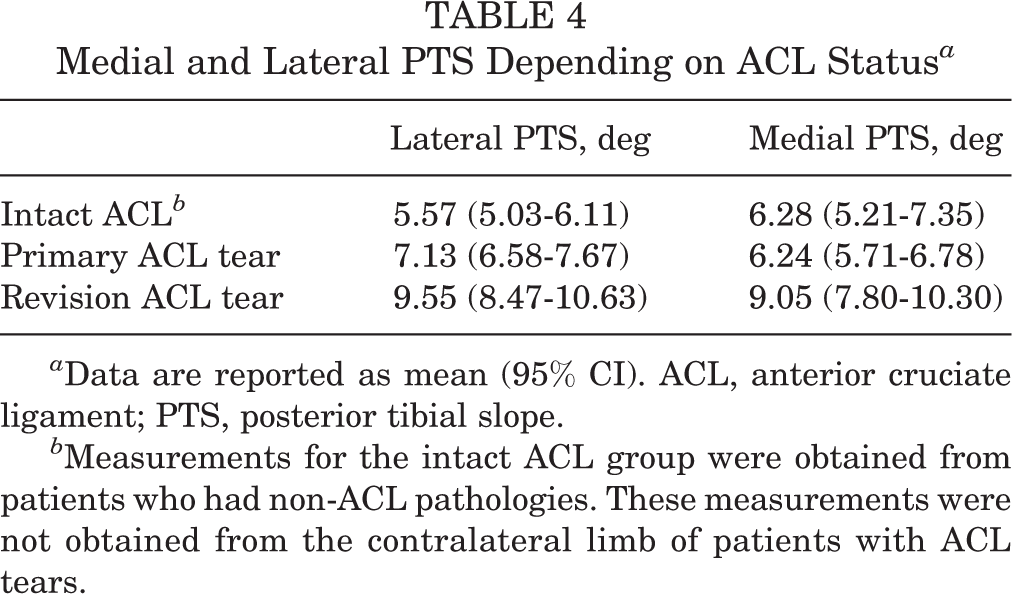
a Data are reported as mean (95% CI). ACL, anterior cruciate ligament; PTS, posterior tibial slope.
b Measurements for the intact ACL group were obtained from patients who had non-ACL pathologies. These measurements were not obtained from the contralateral limb of patients with ACL tears.
The mean slope of the failed ACLR group was more than 2° larger than either the intact or primary ACL tear group in both the medial and lateral PTS measurements, which was greater than the previously established MCID (≥2° difference). 18
Risk of Bias
Each of the studies were evaluated for quality and risk of bias using the MINORS tool. In total, there were 76 studies that were considered a low risk for bias and 6 studies with a medium risk for bias. The full results of this portion of the study can be viewed in Supplemental Table S1.
Discussion
The primary finding of this systematic review and meta-analysis was that patients with failed ACLRs had significantly greater medial and lateral PTS than those with either intact native ACLs or those that had primary ACL tears. Moreover, the difference in mean PTS between the failed ACLR group and either the intact or primary ACL tear cohorts was greater than the previously established MCID. 18 Ultimately, our hypothesis that patients with torn ACLR grafts would have significantly larger lateral PTS compared with patients with native ACLs or those with primary ACL tears was supported by the findings of the current analysis.
In the current analysis, patients in the failed ACLR cohort were found to have significantly larger medial and lateral PTS compared with patients in the intact ACL and primary ACL tear cohorts; the difference in mean PTS was greater than 2° for both medial and lateral PTS. In addition, the lateral PTS of the primary ACL tear group was significantly greater than the intact ACL cohort, whereas there was no significant difference between these subgroups with respect to medial PTS. A previous case series by Todd et al 98 included 140 total patients and concluded that patients with noncontact ACL injury had significantly larger PTS (9.39° vs 8.50°). Previous studies reached similar conclusions with respect to intact ACLs compared with torn ACLs. 14,39,80,81 Additional studies have also reported increased PTS with 1 or more patients undergoing revision ACLR compared with those undergoing primary ACLR. 20,31,72 A previous meta-analysis that included 14 studies reported greater lateral PTS in individuals with ACL injury than in those with intact ACLs. 107 However, the authors of the aforementioned meta-analysis reported that they were skeptical of this finding because of the wide variability in their included studies. We are more confident in our findings in the current review because of the large number of studies and patients, and because of the large difference in pooled means between groups that we observed.
There was no clinical or statistical difference identified between the medial PTS of the intact ACL and primary ACL tear cohorts; these were the only groups that were not significantly different. This finding is supported in the literature by several studies that have postulated that the lateral slope is a more significant risk factor for ACL injury than the medial slope. 57,72,93,104 A study by Webb et al 104 found that ACL-deficient knees had significantly greater lateral PTS (5.7° vs 3.4°, P < .001) but not medial PTS (5.4° vs 5.1°, P = .42) compared with those with intact ACLs. This conclusion is also supported by the biomechanical literature, which suggests that an increased lateral PTS is associated with greater anterior motion of the lateral compartment, which creates a net internal rotation that increases the strain on the ACL. 9,33 Despite the findings from the current study and the supporting literature that lateral PTS likely has a greater effect on overall ACL strain than does medial PTS, several studies have shown that severe inclinations at either plateau can significantly affect overall ACL strain and that both the medial and lateral PTS likely affect ACL stability. 9,67
The current meta-analysis also provides accurate, updated normative values for 3 distinct cohorts based on ACL integrity: intact ACL, primary ACL tear, and failed ACLR. Specifically, for knee surgeons and sports medicine researchers, PTS is a growing area of interest and clinicians/researchers are often forced to reference larger case series when attempting to identify the average PTS of patients. The current study provides a large meta-analysis comprising more than 12,000 patients that surmises an accumulation of recent literature to accurately represent the global averages in slope based on ACL status/integrity.
This systematic review further highlights the true variety of imaging modalities and measurement strategies used to report PTS. Although the purpose of the current analysis was not to compare these modalities statistically, this systematic review of literature brought attention to this diversity. In the current analysis, 38% of studies reported measurements from lateral radiographs and 57% used MRI. A previous study concluded that MRI measurements tended to be smaller than those obtained from radiographs. 47 In addition, 18% of studies included in the current analysis reported only lateral PTS measurements and 27% reported strictly medial PTS; the literature shows that these values are significantly different. 42 Finally, there are a variety of measurement techniques, including those that consider the anatomic axis, which is commonly identified using either the circle or midpoint lines technique; the mechanical axis; the posterior tibial cortex; or the anterior tibial cortex. Several studies have noted significant differences between measurement values from these measurement techniques. 15,23,65,108 Specifically, one study with 140 total patients reported a significant difference in PTS measurement techniques that utilized the anatomic axis from lateral long-leg tibia radiographs (11.6°) and standard lateral radiographs (11.8°) compared with those that considered the mechanical axis obtained from lateral long-leg tibia radiographs (9.5°); 55% of measurements from this study were more than 2° different when comparing the anatomic axis and mechanical axis for an individual on the same lateral radiograph. 23
We acknowledge that this systematic review and meta-analysis has some limitations. First, many of the included studies either did not include all demographic variables or did not provide measures of variation for these variables, and we were unable to include these data in the final analysis. As such, we are unable to exclude these as possible confounding variables that may have contributed to our findings. In addition, there were a variety of measurement techniques across the included studies, including 3 different imaging modalities. While all included techniques have been validated in the literature, we recognize that this could contribute to the variability within groups of the current analysis. Finally, the failed ACLR group is relatively heterogenous as many of these studies included patients who underwent multiple rerevisions and because the specific reason for ACLR failure was not always noted in the individual studies.
Conclusion
This systematic review and meta-analysis found that both lateral and medial PTS measurements are greater in patients who had failed previous ACLR than those with a primary ACL tear or with an intact native ACL. In addition, the lateral PTS of patients with primary ACL tears is greater than those with an intact native ACL. Finally, the current analysis highlights the variety of measurement techniques and modalities used in the literature and emphasizes the importance of continuity in measurement reporting and referencing.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221079380.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221079380 - Posterior Tibial Slope in Patients With Torn ACL Reconstruction Grafts Compared With Primary Tear or Native ACL: A Systematic Review and Meta-analysis
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221079380 for Posterior Tibial Slope in Patients With Torn ACL Reconstruction Grafts Compared With Primary Tear or Native ACL: A Systematic Review and Meta-analysis by Robert S. Dean, Nicholas N. DePhillipo and Robert F. LaPrade in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 20, 2021; accepted November 30, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. has received grants from Arthrex, Linvatec, Ossur, and Smith & Nephew; consulting fees from Arthrex and Smith & Nephew; speaking fees from Smith & Nephew; and royalties from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.