
Abstract
Background:
A posterior tibial slope (PTS) >12° has been shown to correlate with failure of anterior cruciate ligament (ACL) reconstruction (ACLR). PTS-reducing osteotomy has been described to correct the PTS in patients with a deficient ACL, mostly after failure of primary ACLR.
Purpose:
To report radiologic indices, clinical outcomes, and postoperative complications after PTS-reducing osteotomy performed concurrently with revision ACLR (R-ACLR).
Study Design:
Case series; Level of evidence, 4.
Methods:
A review of medical records at 3 institutions was performed of patients who had undergone PTS-reducing osteotomy concurrently with R-ACLR between August 2010 and October 2020. Radiologic parameters recorded included the PTS, patellar height according to the Caton-Deschamps Index (CDI), and anterior tibial translation (ATT). Patient-reported outcomes (International Knee Documentation Committee [IKDC] and Knee injury and Osteoarthritis Outcome Score [KOOS]), reoperations, and complications were evaluated.
Results:
Included were 23 patients with a mean follow-up of 26.7 months (range, 6-84 months; median, 22.5 months). Statistically significant differences from preoperative to postoperative values were found in PTS (median [range], 14.0° [12°-18°] vs 4.0° [0°-15°], respectively; P < .001), CDI (median, 1.00 vs 1.10, respectively; P = .04) and ATT (median, 8.5 vs 3.6 mm, respectively; P = .001). At the final follow-up, the IKDC score was 52.4 ± 19.2 and the KOOS subscale scores were 81.5 ± 9.5 (Pain), 74 ± 21.6 (Symptoms), 88.5 ± 8 (Activities of Daily Living); 52.5 ± 21.6 (Sport and Recreation), and 48.8 ± 15.8 (Quality of Life). A traumatic ACL graft failure occurred in 2 patients (8.7%). Reoperations were necessary for 6 patients (26.1%) because of symptomatic hardware, and atraumatic recurrent knee instability was diagnosed in 1 patient (4.3%).
Conclusion:
Tibial slope–reducing osteotomy resulted in a significant decrease of ATT and can be considered in patients with a preoperative PTS ≥12° and ≥1 ACLR failure. In highly complex patients with multiple prior surgeries, the authors found a reasonably low graft failure rate (8.7%) when utilizing PTS-reducing osteotomy. Surgeons must be aware of potential complications in patients with multiple previous failed ACLRs.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) is the treatment of choice for patients with symptomatic instability after an ACL tear. However, the risk of ACLR failure is unacceptably high in young patients who return to contact pivoting sports. 15 While there are a multitude of factors that are associated with risk of ACLR failure, limb malalignment, in particular increased posterior tibial slope (PTS), has been identified as an independent risk factor for ACL injury and ACLR graft failure. 11,20
The normal range of PTS is described as approximately 7° to 10° in intact knees. 8 In an early study, Dejour and Bonnin 6 reported the radiologic association between increased PTS and resulting increased anterior tibial translation (ATT) in patients with a deficient ACL. Multiple studies have now shown an association between increased PTS and increased risk of ACL injury and subsequent ACLR failure. 7,18 More recently, large clinical studies have identified an increased PTS >12° to be correlated with higher graft failure rates after ACLR. 9,20 When combined with younger age (≤18 years and PTS ≥12°), the 20-year graft survivorship after ACLR using hamstring tendon grafts has been shown to be 22% in a large series from Australia. 18
The mechanism of failure is likely due to the linear relationship between PTS and the amount of ACL graft force experienced during axial loading, as demonstrated in a cadaveric model by Bernhardson et al. 2 Furthermore, in vitro biomechanical studies have proven that a PTS reduction osteotomy causes a significant decrease in ACL graft load and ATT. 2,22 Therefore, PTS correction performed concurrently with revision ACLR (R-ACLR) has the potential to protect the ACL graft, decreasing postoperative failure rates.
With the improved knowledge of the role of PTS in the risk of ACLR failure, PTS-reducing osteotomy has gained popularity over the past decade for patients with previously failed ACLR. However, there are only 3 small case series that have described the indications, surgical technique, postoperative results, and complications. 1,5,19 All the studies incorporated an anterior closing-wedge proximal tibial osteotomy technique to reduce PTS. However, there are subtle variations in the indications and specific technique utilized, particularly in relation to the level of the osteotomy and the management of the tibial tubercle.
The purpose of this study was to report indications, early radiologic and clinical outcomes, and postoperative complications after closing-wedge PTS-reducing proximal tibial osteotomy, performed in a group of patients who underwent R-ACLR. We hypothesized that PTS-reducing proximal tibial osteotomy would represent a reproducible surgical intervention with a low risk of postoperative complications and a decrease of ATT.
Methods
A retrospective review of medical records including patients who underwent R-ACLR and associated PTS-reducing tibial osteotomy was performed at 3 centers (University of Western Ontario, University of Pittsburgh, and University of Calgary) between August 2010 and October 2020. A preoperative PTS ≥12° and previous ACLR failure were considered inclusion criteria. Therefore, the final sample included patients who underwent R-ACLR and additional PTS-reducing osteotomy with or without associated coronal alignment correction (N = 23). Approval for this study was obtained by the institutional review boards of all 3 involved centers, and written informed consent was obtained from all included patients. Demographic, radiological, and surgical data were collected on a consecutive series of patients who underwent a closing-wedge proximal tibial osteotomy to reduce PTS associated with R-ACLR. Concomitant procedures such as meniscectomy, meniscal repair, lateral extra-articular tenodesis (LET), and meniscal allograft transplantation; reoperations; and complications were recorded. Data collection was performed by 4 orthopaedic fellows (T.V., S.T., P.W.W., A.R.-S.).
R-ACLR was performed by 3 senior orthopaedic surgeons (M.H., V.M., A.M.J.G.) in a 1-stage or 2-stage procedure based on the previous tunnel positions, tunnel widening, and surgeon preferences. In the case of 2-stage revision, PTS-reducing osteotomy was performed as the first stage associated with bone grafting of the tibial and/or femoral tunnel. The PTS was corrected using a supratuberosity anterior closing-wedge proximal tibial osteotomy in 19 patients 5 and with a complete tibial tubercle osteotomy in 4 cases. 19 Osteotomies were stabilized using Richards staples (Smith & Nephew) or the TOMOFIX osteotomy system (DePuy Synthes). Techniques were based on the surgeon’s preference. Concomitant LET was performed in patients with a positive pivot-shift grade of 3 during examination under anesthesia.
Radiologic assessment was performed from 3 months onward, reporting the PTS correction after complete bone union. PTS and ATT were calculated via loadbearing lateral radiographs pre- and postoperatively. 6 Because of the dynamic component of ATT in patients with a deficient ACL, nonweightbearing radiographs were not used to measure ATT. Patellar height was measured in the lateral radiograph using the Caton-Deschamps Index (CDI) pre- and postoperatively. 3 All radiologic measurements were performed by the 4 orthopaedic clinical fellows.
Two patient-reported outcome measures (PROMs), the Knee injury and Osteoarthritis Outcome Score (KOOS; 5 subscales) and the International Knee Documentation Committee (IKDC) Subjective Knee Form, were collected at the final clinical assessment. 10,17 Postoperative joint instability and failure criteria were based on a positive pivot-shift grade ≥2.
Statistical Analysis
Statistical methods were used in data analysis through descriptive and inferential statistics. Patient, surgical, and radiographic variables were summarized using mean, range of distribution, and standard deviation for normally distributed variables and median and interquartile range (IQR) for nonnormally distributed variables. A nonparametric Wilcoxon signed-rank test was used to compare preoperative and postoperative PTS, ATT, and patellar height measurements, given the small number of participants and the inability to assume a normal distribution. Statistical significance was set at P < .05.
The intraclass correlation coefficient (ICC) and associated 95% CIs were used to assess the intrarater and interrater agreement for the radiologic measurements (PTS, ATT, and CDI). One rater performed radiographic measurements on the baseline radiographs at 2 time points several weeks apart to measure intrarater agreement. The rater was blinded to the original measurements at the time assessment was repeated. Three independent raters then measured the same radiographs to determine interrater agreement.
All analyses were performed using the SPSS (Version 23.0; IBM).
Results
Of the 23 patients identified, 52.2% (n = 12) were male, with a mean (±SD) body mass index of 25.6 ± 8.6. The mean clinical follow-up was 26.7 months (range, 6-84 months; median, 22.5 months). The mean age at the last R-ACLR was 28.7 ± 9.8 years. A re-revision ACLR was performed in the majority of cases (69.6%). A 2-stage revision was performed in 7 patients (30.4%), with the R-ACLR completed after bone healing was confirmed (range, 5-11 months). Eight patients (34.8%) had a biplanar closing-wedge osteotomy to address associated coronal plane malalignment. Allograft tissue was the most common graft at the R-ACLR (39.1%).
Reoperations were necessary for 6 patients (26.1%) because of symptomatic hardware. Associated chondral debridement and manipulation under anesthesia were performed during hardware removal in 2 patients. One patient with 2 previous re-revision ACLRs developed complex regional pain syndrome. Graft failure was defined in the event of a high-grade pivot shift (grade ≥2) during clinical follow-up. A traumatic ACL graft failure occurred in 2 patients (8.7%) at 18 and 27 months postoperatively, and an atraumatic recurrent knee instability was diagnosed in 1 patient (4.3%). Concomitant treatment, alignment correction, and postoperative complications are summarized in Table 1.
Surgical Data and Postoperative Complications a

a Dashes indicate area not applicable. AF, arthrofibrosis; AG, allograft; BPTB, bone–patellar tendon–bone; CRPS, regional pain syndrome; HC, heterotopic calcification; LET, lateral extra-articular tenodesis; MAT, meniscal allograft transplantation; R-ACLR, revision anterior cruciate ligament reconstruction; QT, quadriceps tendon; SH, symptomatic hardware.
b Associated tibial tubercle osteotomy.
c Root repair.
d Anterolateral ligament reconstruction.
e Patellar tendon.
The ICCs for the PTS measurement indicated excellent intrarater agreement (ICC, 0.92-0.98) and good to excellent interrater agreement (ICC, 0.88-0.99). Excellent interrater and intrarater reliability values were achieved regarding the ATT measurement (ICC [3,1], 0.99; 95% CI, 0.97-1.00, 0.98-1.00). The ICCs regarding the CDI indicated good to excellent intrarater agreement (ICC, 0.83-0.99) and excellent interrater agreement (ICC, 0.93-0.99).
The PTS was statistically significantly reduced from the preoperative to postoperative state (median [IQR], 14.0° [2.0°] vs 4.0° [7.8°], respectively; P < .001) (Figure 1 and Table 2). Patients without a weightbearing lateral radiograph were not included in the ATT evaluation. Therefore, ATT measurements were available for 17 patients (73.9%), and a statistically significant difference between pre- and postoperative measurements was found (median [IQR], 8.5 [5.4] vs 3.6 [4.6] mm, respectively; P = .001) (Table 2). The CDI values indicated that patellar height was statistically significantly altered from preoperative values to after the PTS correction (median [IQR], 1.00 [0.42] vs 1.10 [0.35]; P = .04), yet CDI still remained within normal limits (CDI ≤1.2).
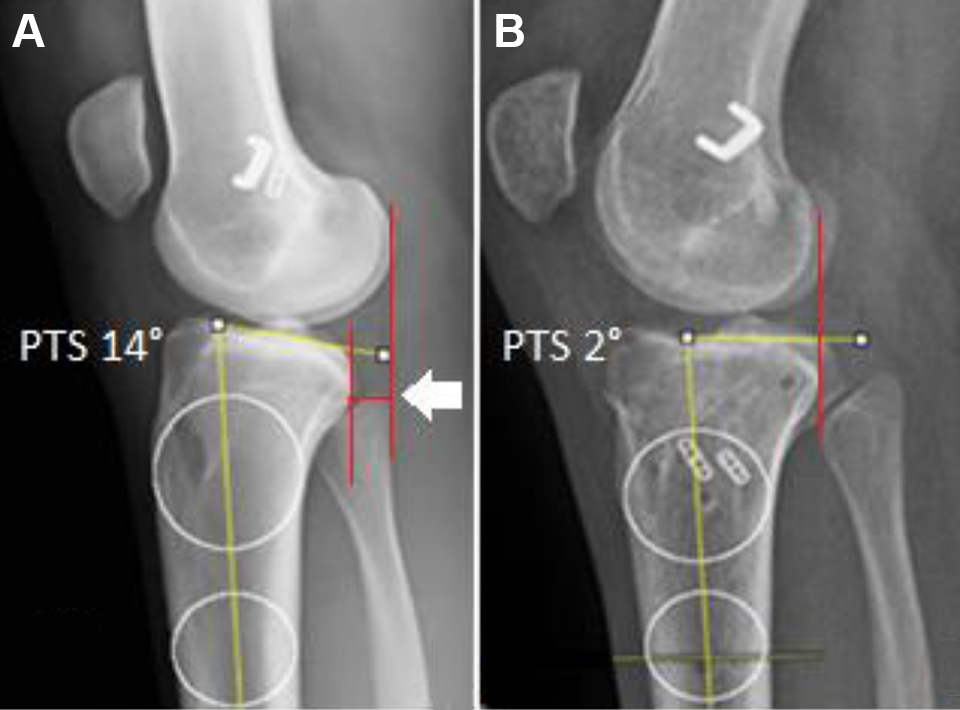
(A) Preoperative posterior tibial slope (PTS) and anterior tibial translation (ATT) (white arrow). (B) Postoperative PTS and ATT reduction after osteotomy associated with revision anterior cruciate ligament reconstruction was performed.
Radiographic Data a

a Data are reported as median [interquartile range]. Boldface P values indicate a statistically significant difference between preoperative and postoperative values (P < .05). ATT, anterior tibial translation; CDI, Caton-Deschamps Index; PTS, posterior tibial slope.
Postoperative PROM scores were available in 14 patients (60.9%) and are summarized in Table 3.
PROM Scores (n = 14 patients) a

a Data are reported as mean ± SD. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life.
Discussion
The most important finding of this study was that closing-wedge proximal tibial osteotomy proved to be a reliable method to reduce PTS and ATT in a cohort of patients who had undergone R-ACLR, with an acceptable postoperative complication profile based on the complexity of the patient population treated. Similar to 3 previously published studies, the postoperative radiographic assessment observed a significant reduction of the PTS when a closing-wedge PTO was performed, either concomitantly with R-ACLR or in a staged fashion. 1,5,19 This resulted in a reduction in ATT and satisfactory graft survivorship. There was a relatively high rate of complications observed in this cohort. However, most of these were associated with symptomatic hardware that resolved with hardware removal. More significant complications, such as arthrofibrosis and complex regional pain syndrome, were seen in patients who had previously undergone multiple R-ACLRs. This is illustrated by the reduced patient-reported outcome scores observed at the final follow-up and is an indication of the complexity of the case mix in this series. Previous studies have demonstrated that multiple graft harvestings, a high prevalence of chondral lesions, and associated meniscal resection reported in patients who had undergone R-ACLR are related to an increased risk of poor postoperative outcomes. 4,14
In the first published case series of slope-reducing PTO, Sonnery-Cottet et al 19 presented 5 cases of combined anterior closing wedge (ACW) and tibial tubercle osteotomy (TTO) with R-ACLR. Satisfactory radiographic and clinical outcomes were observed at the final follow-up. The authors suggested that PTS-reducing osteotomy should only be indicated in the re-revision ACLR scenario because of the complex technical procedure and demanding postoperative rehabilitation process. Associated TTO may allow better control of the patellar height after PTS correction, as the position of the tubercle bone block can be altered. However, we prefer to avoid TTO, as it requires a more gradual postoperative rehabilitation to avoid extensor mechanism complications, which in themselves could potentially lead to patellar tendon contracture and patella infera.
Dejour et al 5 reported satisfactory results with a case series of 9 patients who underwent 1-stage slope reduction osteotomy and concomitant R-ACLR, all of whom had ≥2 previous ACLR failures. Utilizing a similar supratuberosity osteotomy to that predominantly performed in the current study, thereby avoiding potential extensor mechanism issues, radiologic postoperative analysis showed a satisfactory correction of the PTS and improvement of the side-to-side difference in ATT. Similar to the results described in the current study, the patellar height did not change in a clinically significant manner after supratuberosity PTS-reducing osteotomy as measured by the CDI, indicating that a TTO is not always required. The difference in postoperative clinical outcomes between these 2 studies and our cohort may be explained by the multiple failures and subsequent revision reconstructions that were included in our study, as well as the large percentage of 2-stage reconstructions.
Subjective unsatisfactory functional clinical outcomes were also identified in previous cohorts of patients after R-ACLR. Lind et al 12 reported a reoperation rate of 30%, with 31% of those cases reporting a low KOOS Quality of Life (QOL) subscale score of 44 points. The Multicenter Orthopaedic Outcomes Network cohort reported a median of 62.5 points on the KOOS QOL score in a sample of 393 patients at a minimum of 2 years after R-ACLR. 21 When compared with primary ACLR, patients who had undergone R-ACLR achieved worse postoperative functional outcomes. 4
The low postoperative PROM scores in our cohort are in contrast to those in the study by Akoto et al, 1 who described satisfactory radiological and clinical outcomes in a case series of 22 patients who underwent 1-stage R-ACLR with associated LET and PTS-reducing osteotomy as a first R-ACLR. Those authors suggested that early management of the PTS at the first R-ACLR should be considered to avoid multiple failures and repeated operations that can be associated with unfavorable outcomes.
As seen in our study, multiple procedures may be associated with worse clinical outcome and an increased risk of arthrofibrosis and complex regional pain. In contrast, a more aggressive approach with early slope correction at the first revision as per Akoto et al 1 can result in good outcomes. However, it is important to recognize that other complications can be associated with PTS-reducing osteotomy, such as knee hyperextension, which can increase graft force and potentially increase risk of failure. 13 No symptomatic knee hyperextension was identified in our study, which we attribute to careful assessment of preoperative knee hyperextension. Preoperative hyperextension >10° is a contraindication to an anterior closing-wedge osteotomy. 16
Based on our experience and previous studies, 5,19 PTS-reducing osteotomy should be considered in patients with a PTS ≥12° who have previously had a failed primary ACLR. Lower degrees of PTS may be appropriate to treat with osteotomy if significant ATT (>10-mm side-to-side difference) is identified preoperatively in a knee that had otherwise been treated with an acceptable previous ACLR. It is our preference to perform an LET in the first revision, as this has also been shown to result in excellent outcomes without incurring the significant risks associated with osteotomy. 1 If, however, an LET was utilized in the primary ACLR, a PTO-reducing osteotomy may be a more appropriate surgical option in the first revision.
Limitations
The present study has several limitations. This is a relatively small sample size including a heterogeneous population of patients evaluated with ACLR failure. It includes a retrospective study design and incomplete PROMs with varying clinical outcomes and times of follow-up from 3 centers. However, the paucity of information pertaining to this technique in the literature necessitates this type of information to inform clinicians as to the pros and cons of such a complex surgical intervention. ATT was collected from the deficient ACL and not compared with the intact ACL knee as per previous similar studies. Additionally, not all patients had a weightbearing lateral radiograph; hence, postoperative measurement of ATT was not possible in all cases. Furthermore, postoperative sports activity level was not included in this analysis because most of the patients included were not regularly involved in sports activities preoperatively because of the complexity of their knee symptoms and presentation. Finally, 2 patients with <1 year of follow-up were included. However, the majority of complications that we saw in this patient group occurred at an early time point, and radiographic outcomes were still possible within the time frame studied.
Conclusion
Closing-wedge PTS-reducing osteotomy resulted in a significant decrease of ATT and low traumatic graft failure rate (8.7%). Unsatisfactory clinical outcomes reported are likely related to patients undergoing multiple surgeries. Surgeons must be aware of potential complications in patients with multiple previous failed ACLRs. We recommend that a tibial slope–reducing osteotomy should be a component of the R-ACLR treatment algorithm and can be considered in patients with PTS ≥12°.
Footnotes
Final revision submitted August 3, 2022; accepted September 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.J.G. has received consulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Western Ontario (reference No. 101533), the University of Pittsburgh (reference No. STUDY20050226), and the University of Calgary (reference No. E-24918).