
Abstract
Background:
Opioids are commonly used to treat postoperative pain; however, guidelines vary regarding safe opioid use after hip arthroscopy.
Purpose/Hypothesis:
The purposes were to (1) identify risk factors for persistent opioid use, (2) assess the effect of opioid use on outcomes, and (3) describe common opioid prescribing patterns after hip arthroscopy. It was hypothesized that preoperative opioid use would affect complication rates and result in greater postoperative opioid use.
Study Design:
Case-control study; Level of evidence 3.
Methods:
The Utah State All Payer Claims Database was queried for patients who underwent hip arthroscopy between January 2013 and December 2017. Included were patients ≥14 years of age at index surgery with continuous insurance. Patients were separated into acute (<3 months) and chronic (≥3 months) postoperative opioid use groups. Primary outcomes included revision surgery, complications (infection, pulmonary embolism/deep venous thrombosis, death), emergency department (ED) visits, and hospital admissions. Multivariate logistic regression was utilized to identify factors associated with the outcomes.
Results:
Included were 2835 patients (mean age, 47 years; range, 14-64 years), of whom 2544 were in the acute opioid use and 291 were in the chronic opioid use group. Notably, 91% of the patients in the chronic group took opioid medications preoperatively, and they were more than twice as likely to carry a mental health diagnosis (P < .01). Patients in the acute group had a significantly shorter initial prescription duration, took fewer opioid pills, and had fewer refills than those in the chronic group (P < .01 for all). Patients in the chronic group had a significantly higher risk of postoperative ED visits (odds ratio [OR], 2.76; P = .008), hospital admission (OR, 3.02; P = .002), and additional surgery (P = .003), as well as infection (OR, 2.55; P < .001) and hematoma (OR, 2.43; P = .030). Patients who had used opioids before hip arthroscopy were more likely to need more refills (P < .01). A formal opioid use disorder diagnosis correlated significantly with postoperative hospital admissions (OR, 3.83; P = .044) and revision hip arthroscopy (OR, 4.72; P = .003).
Conclusion:
Mental health and substance use disorders were more common in patients with chronic postoperative opioid use, and chronic postoperative opioid use was associated with greater likelihood of postoperative complications. Preoperative opioid use was significantly correlated with chronic postoperative opioid use and with increased refill requests after index arthroscopy.
Keywords
Hip arthroscopy affords surgeons the ability to treat a large variety of hip pathologies, including femoroacetabular impingement (FAI) syndrome. 30 The use of hip arthroscopy has increased substantially. 38 The common age range of patients undergoing this procedure is 20 to 30 years, 44 with the population most at risk for nonmedical use of opioids in roughly the same range. 29 In addition to local anesthetic blocks, anti-inflammatory medications, and other analgesia adjuncts, opioid medications are often a part of the pain management approach after hip arthroscopy.
The type and amount of opioid medications prescribed after surgery vary widely among surgeons. 43 A recent systematic review focused on opioid use after shoulder, knee, and hip arthroscopic procedures, identifying that opioids were overprescribed in all areas and patients had at least one-third of their prescription remaining, with only 36% receiving counseling on how to dispose of residual pain medications. 45 Patients undergoing hip arthroscopy had the highest mean morphine milligram equivalents prescribed. 45 Selley et al 44 assessed opioid usage in 2 groups of patients, finding excessive medication remaining in those prescribed more opioids with no difference in pain between the groups. Various risk factors for continued opioid use after surgery have been identified, including the use of preoperative opioids and muscle relaxants 44 and the need for additional opioid refills. 3
Misuse of opioid medications has serious implications for public health. In recent years, the nontherapeutic use of opioids has reportedly increased 3-fold. 41 The cost of opioid prescription misuse is substantial—indirect and direct costs are estimated at $53.4 billion in the United States. 20 The opioid epidemic has been addressed both at the federal government level and by the American Academy of Orthopaedic Surgeons, with a call for judicious prescribing led by evidence-based guidelines. 39 The risks associated with excessive and nonmedical use of opioids include narcotic abuse and diversion. Unfortunately, prior research has documented a correlation between prescription quantity and higher opioid consumption, with patients using 0.53 more pills for every additional pill prescribed. 27
While there are opioid prescribing targets suggested after hand and adult reconstructive surgeries, 19,33,40 there is a dearth of information regarding the appropriate use of opioids after hip arthroscopy. The aims of this study were to (1) identify the risk factors for persistent opioid use after surgery, (2) assess the effect of opioid use on outcomes after hip arthroscopy, and (3) describe the common opioid prescribing patterns after hip arthroscopy. We hypothesized that preoperative opioid use would affect outcomes and result in greater postoperative opioid use.
Methods
After receiving institutional review board approval for this study, we queried the Utah State All Payer Claims Database (APCD) for patients who underwent hip arthroscopy between January 2013 and December 2017. Utah’s state-mandated APCD contains comprehensive claims data from private and public payers (Medicare Advantage and Medicaid) representing 2.4 million persons and 80% of the Utah population beginning in the year 2013. 47,48 The APCD consists of medical claims, pharmacy claims, dental claims, and enrollment files that are contributed by the payers in Utah. In this study, patients who were covered by Medicaid were excluded because of concerns for higher inherent opioid use in this population. 18
Patient Selection
Hip arthroscopy was identified using Current Procedural Terminology (CPT) codes, and the index date was defined as the surgical date anytime between July 2013 and December 2016. Patients who were ≥14 to 64 years of age at index date and continuously insured 6 months before surgery and 1 year after surgery were included to ensure complete data were available for query. Exclusion criteria were patients with Medicare insurance as well as those <14 years of age at the index date of surgery to eliminate skeletally immature patients, given the correlation of FAI syndrome with skeletal maturity, while including skeletally mature patients who become symptomatic and require early intervention.
Outcomes and Covariates
Revision hip arthroscopy, conversion to total hip arthroplasty, lumbosacral surgery, and abdominal surgery were identified via CPT codes after the index surgery; they were included to capture procedures that could indicate a failure of the index surgery to satisfactorily relieve symptoms or identify multifactorial symptoms that could be related to other pain origins or syndromes. In addition, all-cause emergency department (ED) visits and hospital admissions were identified using place of service, revenue codes, and CPT codes after surgery. The outcome of death was identified using International Classification of Diseases, Revision 10 (ICD-10) codes (see Supplemental Table S1). Other complications—such as infection and pulmonary embolism (PE)/deep venous thrombosis (DVT)—were identified via ICD-10 code (Supplemental Table S1). Additional covariates, including age at index surgery, sex, Elixhauser Comorbidity Index, 1 comorbid conditions, 8 pain medication use, other medication use, and presence of mental health disorders, were also collected (Table 1). Supplemental Table S2 includes relevant medications.
Covariates Included in Analysis

Determining Opioid Use
Opioid prescriptions 7 were identified using National Drug Code (NDC) 17 in the pharmacy claims in the APCD. Using days supplied for 1 year after the index surgery, we classified the patients into 2 groups depending on their postoperative opioid use: those with <3 months (acute opioid use) or ≥3 months (chronic opioid use) of prescriptions. 15 Preoperative opioid use was also assessed using NDC within 6 months before the index hip arthroscopy date.
Statistical Analysis
Descriptive statistics including mean, SD, frequency, and percentage were used to describe the sample. We used the t test for the continuous variables and chi-square test for the categorical variables to compare the baseline characteristics of the acute versus chronic opioid use groups. Multivariate logistic regression was used to identify factors that were associated with the outcomes; odds ratios (ORs) and P values were reported in the regression tables. Stata statistical software (Version 14; StataCorp) was used, and the significance level was set at .05 for all analyses. 47
Results
A total of 2835 patients were included in analysis. The average age at the time of index hip arthroscopy was 46.5 years (range, 14-64 years), 56.4% were women, and 87.1% lived in an urban area. 47 Overall, 10% of the patients in the cohort (n = 291) used opioids chronically. Table 2 includes the comparison of characteristics between the patients in the acute (<3 months) versus chronic (≥3 months) postoperative opioid use groups. Notably, 91% of the chronic group took opioid medications preoperatively (within 6 months of index hip arthroscopy) compared with 23% of the acute group. Patients with chronic postoperative opioid use were also more than twice as likely as those with acute opioid use to carry a formal mental health diagnosis 7 (Table 1). Obesity, diabetes mellitus, and a preoperative diagnosis of opioid use disorder were all more common in patients with chronic postoperative opioid use.
Baseline Characteristics of Patients With Acute Versus Chronic Opioid Use After Index Hip Arthroscopy a

a Data are reported as mean ± SD or %. Bolded P values indicate a statistically significant difference between groups (P < .05). P-value was not calculated for gender and urban versus rural location. MME, morphine milligram equivalents; NSAID, nonsteroidal anti-inflammatory drug. Dashes indicate that this value could not be calculated for the acute opioid group.
Table 3 outlines the nature of postoperative refill requests in acute and chronic postoperative opioid use groups. Patients in the acute group received a smaller initial prescription duration (5 ± 4 vs 15 ± 10 days) with fewer narcotic pills (32 ± 32 vs 76 ± 176) and had far fewer refill requests (1 ± 2) after initial prescription than those who received ≥3 months of opioids (18 ± 10). In general, patients who had used opioids within 6 months of index hip arthroscopy were much more likely to need ≥1 refills (77%) than those who had not (35%). Patients without preoperative opioid use requested a refill 35% of the time, while those with preoperative use requested a refill 77% of the time (Table 4).
Postoperative Prescription Duration and No. Refills a

a Data are reported as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). MME, morphine milligram equivalents.
Preoperative Prescriptions a

a Data are reported as n (%).
Complications, hospital admissions, ED visits, and need for additional surgery are analyzed in Table 5. Patients with chronic postoperative opioid use required significantly more ED visits (17% vs 9%; P < .01) and necessitated significantly more hospital admissions before index hip arthroscopy (13% vs 5%; P < .01). Similarly, a significantly higher proportion of patients with chronic postoperative opioid use required spine surgery (43% vs 16%; P < .01) and abdominal surgery (10% vs 6%; P = .01) within 1 year after index arthroscopy. They did not undergo a significantly higher rate of total hip replacement or revision hip arthroscopy in the year after index hip arthroscopy.
Postoperative Complications and Outcomes a

a Data are reported as n (%). Bolded P values indicate a statistically significant difference between groups (P < .05). DVT, deep venous thrombosis; ED, emergency department; OR, odds ratio; PE, pulmonary embolism.
b Preoperative refers to within 6 months preoperatively. Postoperative refers to within 1 year postoperatively.
c Within 1 year postoperatively.
Regression analysis was performed to assess the effect of preoperative opioid use, acute postoperative opioid use, and chronic postoperative opioid use on postoperative complications. Table 6 outlines the ORs for postoperative adverse events if patients had preoperative opioid use. Patients were 1.85 times more likely to require abdominal surgery (P = .004) and 1.36 times more likely to require lumbosacral surgery (P = .039) if they had used opioids before index arthroscopy. Preoperative opioid use was not significantly correlated with other adverse events after initial hip arthroscopy.
Preoperative Opioid Use and Odds of Experiencing Adverse Outcomes a
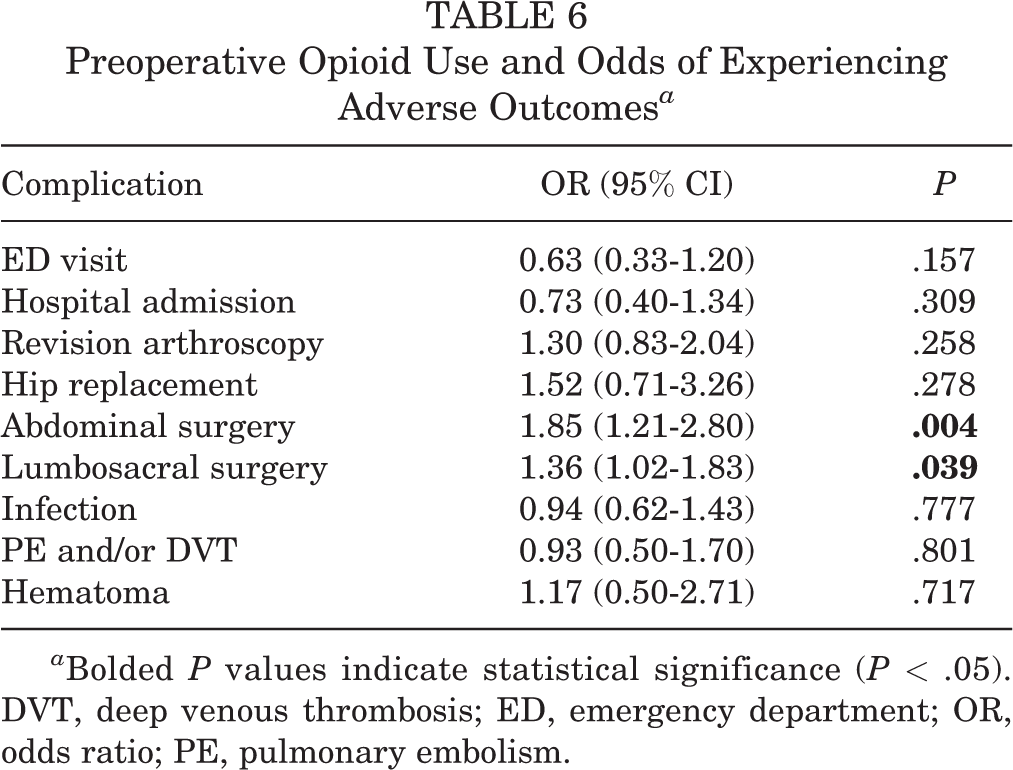
a Bolded P values indicate statistical significance (P < .05). DVT, deep venous thrombosis; ED, emergency department; OR, odds ratio; PE, pulmonary embolism.
Additional regression analyses were conducted to specifically assess the effect of chronic postoperative opioid use (≥3 months) on adverse postoperative events (Table 7). Patients who were in this category were 2.76 times more likely to require an ED visit (P = .008) and 3.02 times more likely to be admitted to a hospital (P = .002). Additionally, they were more likely to undergo revision arthroscopy (OR, 2.38; P = .003), require lumbosacral surgery (OR, 1.68; P = .003), and experience infection (OR, 2.55; P < .001) or hematoma (OR, 2.43; P = .03) after their index arthroscopy.
Chronic Postoperative Opioid Use and Odds of Experiencing Adverse Events a

a Bolded P values indicate statistical significance (P < .05). DVT, deep venous thrombosis; ED, emergency department; OR, odds ratio; PE, pulmonary embolism.
A formal opioid use disorder diagnosis was present in 6% of the patients in the chronic use group, and these patients were 3.83 times more likely to require postoperative inpatient admission (P = .044) and 4.72 times more likely to undergo revision hip arthroscopy (P = .003) (Table 8). Having a diagnosis of any mental health disorder was not correlated with postoperative hospital admissions or complications. There was, however, a trend (P < .1) toward revision arthroscopy and a significant correlation with the need for abdominal surgery (OR, 1.44; P = .042).
Opioid Use and Mental Health Disorders and Odds of Experiencing Adverse Events a

a Dashes indicate insufficient sample size to complete regression. Bolded P values indicate statistical significance (P < .05). DVT, deep venous thrombosis; ED, emergency department; OR, odds ratio; PE, pulmonary embolism.
Finally, when focusing on specific pertinent postoperative complications, it is worth noting several correlations. Patients with a higher comorbidity index were 1.27 times more likely to experience a postoperative infection (P < .001). Increase in age (OR, 1.03; P = .009) and higher comorbidity index (OR, 1.36; P < .001) also increased the likelihood for hematoma.
Discussion
The effect of perioperative opioid mediations around the time of index arthroscopy is not well understood. The primary goals of this study were to assess the effect of opioid use on outcomes and to describe the common opioid prescribing patterns after hip arthroscopy. Patients using opioids before surgery were more likely to require opioid refills postoperatively and use opioids chronically after hip arthroscopy. Patients with chronic opioid use after index arthroscopy had a higher proportion of associated conditions, including mental health disorders and preoperative use of opioids. Patients with chronic postoperative opioid use received initial prescriptions of longer duration and containing more pills and requested more refills. They also were more likely to require ED visits or need hospital admission, necessitate additional surgery in the form of revision arthroscopy and lumbosacral surgery, and experience the postoperative complications of infection or hematoma after their index arthroscopy.
It is important to note that preoperative opioid use was not significantly correlated with postoperative adverse events, except for the propensity for abdominal and lumbosacral surgery. Multiple sources have discussed the relationship between preoperative opioid use before surgery and postoperative outcome. 10,25,31 Cron et al 10 documented that 21% of the patients used opioids before abdominopelvic surgery and opioid use was independently associated with increased morbidity and postoperative health care utilization. In a large study of 34,186 patients, Hilliard et al 25 found that preoperative opioid use was most common among patients undergoing orthopaedic and spinal procedures, with those undergoing lower extremity procedures as the most likely to report use. The differential diagnosis for intracapsular hip pathology includes both spinal and abdominal pathologies, 6,37 and the diagnostic process is not always simple. Patients experiencing long-term pain often intersect with the medical system on multiple occasions in an effort to control pain and obtain a diagnosis. Preoperative opioid use may serve as a reminder for the astute clinician to pay close attention to the differential diagnosis to determine the true pain origin and carefully evaluate if surgery will be beneficial.
Perhaps more importantly, patients using opioids preoperatively were more likely to require opioid refills postoperatively and require ≥3 months of postoperative opioid medication. A far higher proportion of patients who used opioids preoperatively went on to request ≥2 more refills after their index arthroscopy, signifying that preoperative opioid use is a marker for potential prolonged opioid use after surgery, allowing for appropriate counseling and cessation efforts before surgery occurs. Our results reinforced what has been shown previously: preoperative opioid use before index hip arthroscopy remains one of the single most important predictors for chronic postoperative opioid use 2,11,14,21,50 and is closely tied to patient outcomes. 52
In 2020, Beck et al 3 specifically assessed the connection between refills and postoperative outcome, determining that patients requiring more refills had lower patient-reported outcomes and visual analog scale (VAS) satisfaction score averages and higher VAS pain score averages after surgery. Zusmanovich et al 52 had similar results, demonstrating that preoperative opioid use in patients undergoing hip arthroscopy is associated with inferior outcomes compared with opioid-naïve patients, as well as increased risk for continued postoperative use. In patients with preoperative opioid use, continued utilization of these mediations after hip arthroscopy has been documented to be as high as 47%. 14 When taken as a whole, mounting evidence incentivizes physicians to support opioid cessation before surgery to avoid prolonged postoperative use, complications associated with use, 4,34 opioid-induced hyperalgesia, 5 dependence, 51 and misuse. 5,49 Decreasing opioid use is particularly crucial as we navigate the ongoing opioid epidemic and define our role as surgical care providers in that setting. 21 Additionally, as is seen in our study, surgeons prescribe differing amounts of opioids to different patients, and this may represent an opportunity for standardization in practice.
When focusing on chronic postoperative opioid use, we observed that it was significantly correlated with higher risk for postoperative ED visits and hospital admissions. Readmission after hip arthroscopy has been studied on several occasions, with baseline rates between 0.5% and 1.3%. 16,23,36 Du et al 16 documented associated risks for readmission, including increasing body mass index, chronic corticosteroid use, and postoperative transfusion. In 2020, Hartwell and Tjong 24 acknowledged the role of postoperative pain in prompting visits to the ED after hip arthroscopy. Regardless of what prompts an ED visit or a hospital admission, there are notable associated costs. 28 ED presentation and readmission after total knee and total hip arthroplasty have proven to be a high burden to the health care system and have prompted discussion about patient-centered interventions that can safely intervene and prevent those outcomes. 35 Our results suggest that patients with sustained opioid use after surgery require both monitoring and judicious intervention 26 to optimize their safety and lower the risk for ED visits and hospital admissions after index arthroscopy.
Patients with ≥3 months of opioid use after chronic opioid use preoperatively are at risk for more than just additional postoperative hospital presentations. Our results indicated that these individuals were at higher risk for revision arthroscopy and lumbosacral surgery, as well as for postoperative infections and hematomas. While significant relationships between these adverse outcomes and chronic opioid use were present, this does not insinuate causality. It is possible that those patients who experience postoperative complications may have resultant pain that warrants prolonged analgesia.
Additionally, prolonged use of pain medication after index arthroscopy could be related to the presence of concomitant or misdiagnosed pathology that ultimately leads to additional surgical interventions. Finally, patient perception of pain is complicated, and discomfort is not always satisfactorily managed via surgical intervention, leaving them to pursue additional options for treatment of their concerns. However, the current study’s results are similar to prior data of Anciano Granadillo et al 2 who demonstrated prolonged postoperative opioid use was significantly associated with higher risk for revision hip arthroscopy, postoperative complications, and ED visits, as well as conversion to total hip arthroplasty. Rather than assuming a causal relationship, it may be more prudent to use chronic opioid use as a warning that patients may have unaddressed issues or need careful clinical monitoring. This is particularly important given that those with chronic opioid use in this study had more postoperative polypharmacy, with significantly greater use of pregabalin/gabapentin, hypnotics, and benzodiazepines. The use of multiple medications postoperatively is associated with increased risk for poor outcomes after surgery, including readmission. 9,22,32,42
Finally, the role of mental health disorders cannot be understated and is intertwined with substance use. 12,13 While mental health disorders were notably more prevalent in those with chronic postoperative opioid use, the presence of a mental health disorder diagnosis was not significantly correlated with adverse events after index arthroscopy. Similarly, a diagnosis of substance use disorder was not significantly correlated with increased likelihood of adverse events, with the exception of revision arthroscopy. The diagnosis of both a mental health disorder and substance use disorder has been shown to increase perioperative opioid demand and result in greater postoperative complications in the setting of a large cohort of 26,283 patients with upper extremity trauma. 13 Similar results were found after hip fracture surgery, with depression, psychoses, and substance abuse affecting opioid prescription use. 12 The results of the current study also suggest that the presence of mental health and substance use disorders may identify an individual at risk for greater postoperative opioid use, as well as adverse events.
Limitations
Our study had several limitations, including those intrinsic to retrospective design and large database analysis. The APCD allowed access to information from 6 months preoperatively and 1 year postoperatively, capturing patients who were continuously insured. However, data beyond the 1-year mark may have provided further information regarding outcomes and/or medication usage. Nevertheless, we believe that a 1-year time frame would sufficiently capture the need for most related early revisions or postoperative complications. Additionally, patients who are uninsured and who have fee-for-service Medicare may represent a subset of patients whom we could not reliably capture.
We were unable to account for any additional unprescribed substance(s) that a patient may have taken in both the pre- and postoperative setting; however, the study methodology enabled identification of pre- and postoperative pain medication and psychotropic usage using CPT codes, NDC codes, and medication names, thereby representing comprehensive prescription medication patient profiles. In theory, patients could also obtain or cancel their insurance included in the Utah APCD immediately before or after their index surgery, which would influence data accuracy. This scenario is anticipated to be less common, however, even in the setting of a patient moving to a new location, as the APCD is not restricted by state but by insurance carrier, thus allowing for capture of outcomes and medication usage in other states if collected by the same insurance carrier.
The APCD consists of and relies on CPT and ICD-9/10 coding completed by surgeons and Utah insurance billers. It is important to recognize the potential for possible coding errors. In addition, there were a number of patients who were excluded from the study because of lack of 1-year follow-up or lack of continuous insurance during the study period. However, the APCD registry comprises claims data of 2.4 million people and roughly 80% of the Utah population, 47,48 allowing for sufficient generalizability to the general population. The population captured in this large database study had an older mean age (47 years) as compared with a typical hip preservation population. This elevated age could affect the translation of the results and discussion to a younger population. However, the expanded age range of our database analysis (14-65 years) included younger patients and was designed to capture arthroscopic practice profiles and increase the generalizability of the results.
Additionally, patients with Medicaid were excluded from this study, and in doing so, we cannot generalize these results to those patients. Finally, complications and adverse events captured after hip arthroscopy were identified in the 1 year after the index surgery, and we could not confirm that they were directly caused by the procedure itself. Similarly, opioid use after hip arthroscopy could not be directly correlated to that procedure in isolation. Prescribed opioid use was specifically captured, but we were unable to collect data on illegal/unprescribed use. We were unable to identify which specific medical care provider prescribed these medications for patients or the reason for preoperative opioid use (pain origin from hip vs other disorders). Additionally, we could not identify the reasons for needing postoperative ED visits or hospital admissions.
Conclusion
Preoperative opioid use was significantly correlated with chronic postoperative opioid use as well as increased refilled requests after index arthroscopy. Additionally, ≥3 months of postoperative opioid use was associated with greater likelihood of postoperative ED visits, hospital admissions, revision arthroscopy, and lumbosacral surgery, as well as postoperative infections and hematomas. Mental health and substance use disorders were more common in those with prolonged opioid use after surgery.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211003521.
Supplemental material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221077933 - Effect of Perioperative Opioid Use on Patients Undergoing Hip Arthroscopy
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221077933 for Effect of Perioperative Opioid Use on Patients Undergoing Hip Arthroscopy by Miranda J. Rogers, Mark W. LaBelle, Jaewhan Kim, Temitope F. Adeyemi, Christopher E. Sciarretta, Christina E. Bokat and Travis G. Maak in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 10, 2021; accepted November 29, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.G.M. has received education payments, consulting fees, and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Utah (reference No. 98713).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.