
Abstract
Background:
When performing a medial patellofemoral ligament (MPFL) reconstruction, surgeons may place the MPFL graft under higher than anatomic tension to minimize the chance of recurrent instability.
Purpose:
To investigate whether a lateral retinacular release (LRR) significantly decreases patellofemoral contact pressures after an overtensioned (OT) MPFL reconstruction.
Study Design:
Controlled laboratory study.
Methods:
Mean and peak pressure across the patellofemoral joint at 30°, 45°, and 60° of flexion was assessed in 14 cadaveric knee specimens with intact MPFL, transected MPFL, reconstructed MPFL with graft OT, and OT MPFL with LRR. The Wilcoxon signed rank test was used to determine differences across states, with W and C values calculated when possible.
Results:
Mean pressure decreased significantly after MPFL transection compared with intact at 30° (456.9 ± 116.8 vs 410.9 ± 109.4 N, P = .006, W < 7) and 45° (404.9 ± 91.7 vs 369.4 ± 85.3 N, P = .005, W < 5) and increased significantly from intact to OT graft at 30° (456.9 ± 116.8 vs 563.0 ± 11.2 N, P = .003, W < 7), 45° (404.9 ± 91.7 vs 481.4 ± 14.8 N, P = .005, W < 5), and 60° (272.9 ± 139.0 vs 367.0 ± 53.7 N, P = .007, W < 3). Peak pressure increased significantly between intact and OT graft at 30° (1364.0 ± 478.2 vs 2094.4 ± 619.8 N, P = .002, W < 9), 45° (1224.7 ± 491.5 vs 1676.7 ± 779.1 N, P = .005, W < 5), and 60° (1117.7 ± 566.8 vs 1604.2 ± 772.9 N, W < 3). In knees with significantly increased mean pressure after overtensioning, mean pressure increased by 23.3% (11/14 knees) at 30°, 18.3% (10/14 knees) at 45°, and 35.0% (10/14 knees) at 60°. Peak pressure increased significantly by 35.3% (30°), 25.2% (45°), and 29.3% (60°). A significant decrease in mean pressure, toward but not to baseline, was observed between the OT and LRR states at 30° (563.0 ± 11.2 vs 501.5 ± 9.3 N, W < 7) and 60° (367.0 ± 53.7 vs 302.0 ± 13.8 N, W < 5) and a decrease in peak pressure at 30° (2094.4 ± 619.8 vs 1886.5 ± 655.3 N; W < 9).
Conclusion:
LRR led to a statistically significant decrease in pressure across the patellofemoral joint in knees that demonstrated increased contact pressures after an OT MPFL graft.
Clinical Relevance:
LRR after an MPFL reconstruction in which the MPFL graft has been OT may help reduce patellofemoral contact pressures at the time of surgery.
Keywords
Medial patellofemoral ligament (MPFL) reconstruction is a commonly performed surgery for recurrent patella dislocation. 4,12 The ultimate goal of this surgical procedure is to restore the primary medial soft tissue restraint to resist laterally directed forces on the patella, thereby preventing lateral dislocation of the patella. Establishing appropriate graft tension in MPFL reconstruction has proven to be difficult. 1 –5 Proper surgical technique should adequately restore the medial restraint to resist lateral subluxation of the patella and prevent recurrent patellar dislocation while avoiding overconstraint of the patellofemoral joint (PFJ) and increasing patellofemoral contact pressures. 1 –5 The challenge is compounded by the lack of a reliable and reproducible method to tension the MPFL graft. Biomechanical studies have demonstrated a force of 2 N during MPFL reconstruction can restore contact pressures and lateral restraint to a near anatomic state. 1,5,15 However, graft malposition, trochlea dysplasia, changes in graft tension over time, and initial graft maltensioning are potential risk factors for surgical failure. 3,8,13 Surgeons may choose to place the MPFL graft under greater tension than the native MPFL to minimize the risk of recurrent patellar instability. 7
The risk of an overtensioned (OT) MPFL graft is that it can overconstrain the patella, leading to an alteration in PFJ kinematics. 16 One study demonstrated that pressure under a graft after reconstruction is higher than that of the native MPFL. 18 Both biomechanical and computational models have demonstrated that loads exceeding 10 N tension at the time of reconstruction can lead to medialization of the center of pressure and significantly increase contact pressure across the PFJ. 2,7 Some speculate that this may result in patellofemoral degenerative changes and/or pain. A lateral retinacular release (LRR) could help mitigate the potential increased PFJ contact pressures from overtensioning the MPFL graft. We speculate that release of the lateral tether to the patella may relieve increased contact pressure caused by medial overconstraint (Figure 1). However, little is known regarding the use of LRR and its effect on contact pressures in the setting of an OT reconstruction.

Theoretical model illustrating increased contact pressures after overtightened MPFL reconstruction (A) followed by a decrease in pressure after lateral retinacular release (B). Large arrows (A) indicate increased pressure; small arrows (B) indicate decreased pressure after lateral ligament release. MPFL, medial patellofemoral ligament.
The aim of our research was to compare contact pressures of the PFJ in a cadaveric model with different tensioning of the MPFL. We hypothesized that overtensioning of the MPFL graft would result in significantly increased PFJ pressure compared with the intact and cut state and that LRR would result in a significant decrease in PFJ contact pressure.
Methods
Fourteen fresh-frozen cadaveric knee specimens from 10 donors (5 male, 5 female; average age, 82.6 years) were thawed for 24 hours and tested in an isometric simulation. Specimens were obtained from donations to the state anatomy board. Specimens were stripped of skin and subcutaneous tissue overlying the knee joint. Care was taken to preserve the medial and lateral capsuloligamentous structures. The quadriceps and hamstring muscles were then stripped proximally from the femur 5 cm from the superior pole of the patella, preserving muscle, capsule, and ligament distally. The semitendinosus tendon was harvested without violating medial structures. This tendon was chosen over the gracilis due to its larger caliber. A running locking suture was then placed in the quadriceps tendon to allow for attachment to the load frame. Tekscan sensors (Model No. 4000; Tekscan, Inc.) were placed into the PFJ using parapatellar tendon fenestrations in the capsule similar to extended arthroscopy portal incisions to preserve the medial and lateral capsular structures (Figure 2). The sensor was oriented to cover the articular surface of the patella and secured to the capsule using a No. 2 Ultrabraid suture superiorly and inferiorly to preserve the native MPFL and the important lateral capsuloligamentous structures. The insertion of the MPFL was determined by fluoroscopic assistance, direct visualization, and palpation of bony landmarks. The knee was secured in a custom fabricated fixture and mounted in an MTS load frame (MTS 858 Mini Bionix). The quadriceps tendon was loaded with a constant force of 200 N, which approximates knee extension against gravity and is consistent with similar MPFL models. 6, 14 Pressure measurements were obtained with the knee statically positioned in 30°, 45°, and 60° of flexion using a goniometer.

Cadaveric medial patellofemoral ligament reconstruction. (A) Before reconstruction. (B) After reconstruction. Note the parapatellar fenestrations (white arrows) that prevent violation of the medial or lateral capsule before testing.
We tested 4 states sequentially: native MPFL, transected MPFL, MPFL reconstruction performed with graft OT, and OT MPFL with LRR. The knee was taken off tension between testing states but not removed from the frame. Mean and peak contact pressure was recorded using I-scan (Tekscan). Peak contact pressures represented the area 2.6 mm × 2.6 mm of maximal pressure across the PFJ.
The MPFL was reconstructed using a semitendinosus graft. The graft was fixed to the patella using 2 JuggerKnot double-loaded 1.4-mm suture anchors (Zimmer Biomet) loaded with No. 1 braided suture. The medial capsule was then closed over the portion of graft anchored to the patella and reefed using No. 2 Ultrabraid suture. On the femoral side, the graft was placed at the isometric point of the posterior medial femur (Schottle’s point). The graft was secured to the femur with a 5.5-mm polyetheretherketone (PEEK) anchor loaded with No. 2 Ultrabraid suture. During fixation, each limb of the graft was sequentially tensioned with a 22.2-N (5-lb) hanging weight to simulate overtensioning of the MPFL in a consistent manner. A 5-lb weight was chosen because it consistently resulted in significantly increased contact pressure in pilot cadavers. Fixation was performed at 30° flexion. Overtensioning was confirmed with the presence of a reverse-J sign in each specimen. An LRR was performed by sharply incising the lateral parapatellar capsular structures from superior pole to inferior pole of the patella under direct visualization. 11 The release was considered complete when only synovial structures were visible.
After completion of all 4 testing states, the knee was then opened fully to confirm appropriate position of Tekscan sensor. Knees were excluded if it appeared that the sensor had lost fixation at any point during testing. A priori power analysis was based on a previous study 15 that identified a sample size of 8 for 80% power at 95% confidence based on a 0.2 ± 0.3 Mpa change in PFJ contact pressure and on another study 2 that identified a sample size of 12 required for an alpha of 0.05 and power >90% to detect differences in contact pressure across the PFJ.
Data were checked for normality and compared using a Wilcoxon signed rank test. W and C values were calculated and reported with P values, when possible, with alpha P < .05. Results were considered significant if the W value was below the calculated critical value.
Results
Mean contact pressure decreased significantly after transection of the MPFL at 30° and 45° flexion (P = .006 and .005, respectively) (Table 1). No significant change in peak pressure was seen after transection at any degree of flexion (Table 2). An OT MPFL graft led to increased mean pressures in 11 (78.6%) knees at 30°, 10 (71.4%) at 45°, and 10 (71.4%) at 60° (Table 1). Peak pressure increased after overtensioning in 12 knees (85.7%) at 30°, 10 knees (71.4%) at 45°, and 9 knees (64.2%) at 60° (Table 2).
Changes in Mean Contact Pressure from Intact, Cut, Overtensioned, and Lateral Release State in the Knees that Demonstrated Increased Contact Pressures with Overtensioning of the MPFL Graft a
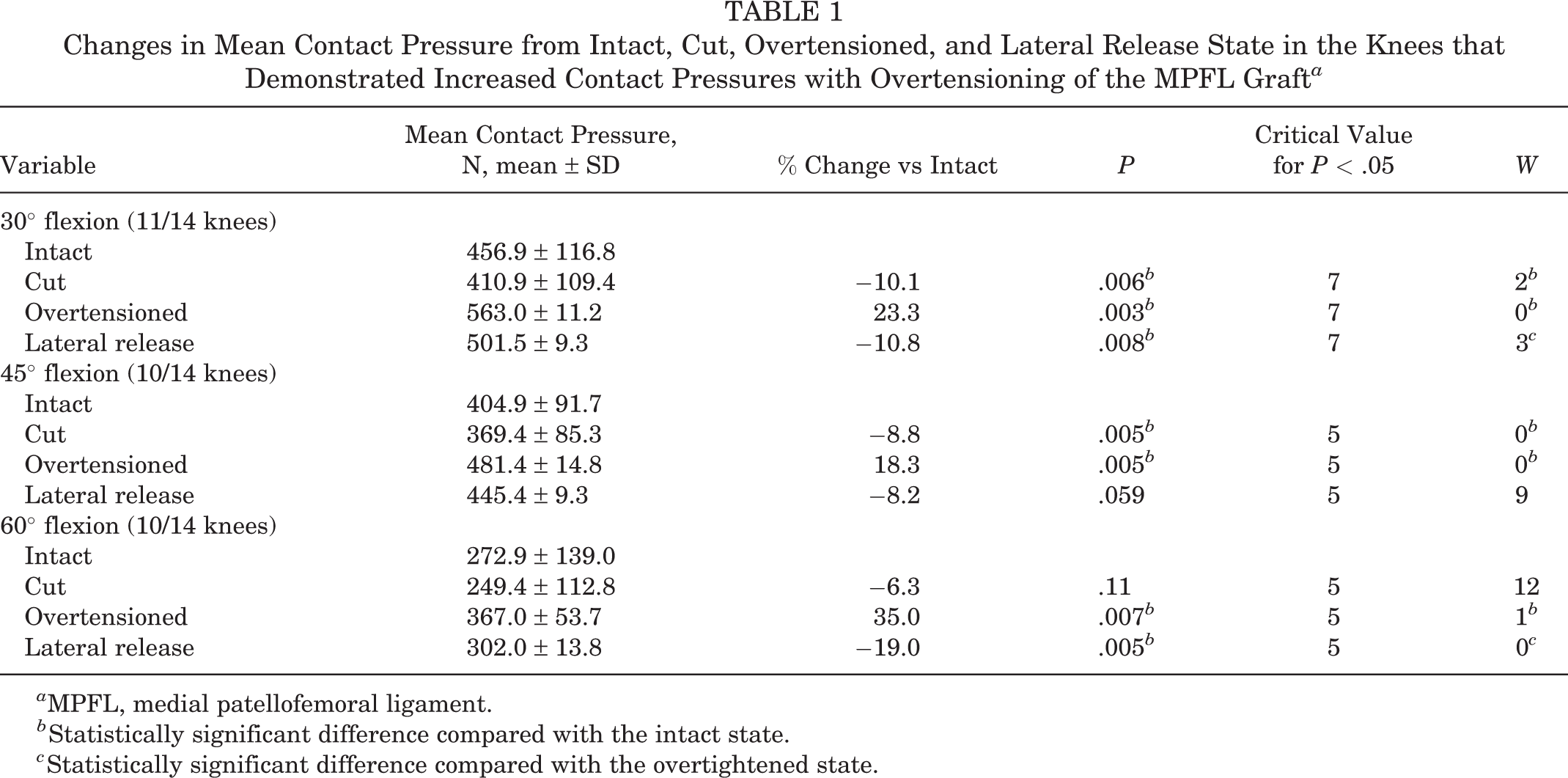
a MPFL, medial patellofemoral ligament.
b Statistically significant difference compared with the intact state.
c Statistically significant difference compared with the overtightened state.
Changes in Peak Contact Pressures from Intact, Cut, Overtensioned, and Lateral Release State in the Knees That Demonstrated Increased Pressures With Overconstrained MPFL Graft a

a MPFL, medial patellofemoral ligament; NA, not applicable due to insufficient number for the Wilcoxon signed rank test.
b Statistically significant difference compared with the intact state.
c Statistically significant difference compared with the overtightened state.
In knees with increased pressure after overtensioning, mean pressure increased significantly from intact to OT graft state at 30° (456.9 ± 116.8 vs 563.0 ± 11.2 N, P = .003, W < 7), 45° (404.9 ± 91.7 vs 481.4 ± 14.8 N, P = .005, W < 5), and 60° (272.9 ± 139.0 vs 367.0 ± 53.7 N, P = .007, W < 3). Peak pressure increased significantly between the intact and OT state at 30° (1364.0 ± 478.2 vs 2094.4 ± 619.8 N, P = .002, W < 9), 45° (1224.7 ± 491.5 vs 1676.7 ± 779.1 N, P = .005, W < 5), and 60° (1117.7 ± 566.8 vs 1604.2 ± 772.9 N, W < 3). In these knees, mean pressure increased by 23.3% (30°, 11/14 knees), 18.3% (45°, 10/14 knees), and 35.0% (60°, 10/14 knees), and peak pressure increased significantly by 35.3% (30°), 25.2% (45°), and 29.3% (60°). A significant decrease in mean pressure toward but not to baseline was observed between OT and LRR state at 30° (563.0 ± 11.2 vs 501.5 ± 9.3 N, W < 7) and 60° (367.0 ± 53.7 vs 302.0 ± 13.8 N, W < 5),and in peak pressure at 30° (2094.4 ± 619.8 vs 1886.5 ± 655.3 N, W < 9) (Figures 3 and 4).

Graphical representation of mean contact pressure changes between the intact, cut, overtensioned (OT), and laterally released (LR) knees with increased pressure after overconstrained MPFL graft. Error bars represent standard deviation. *Significantly different compared with the intact state (P < .05). **Significantly different compared with the OT state (P < .05). MPFL, medial patellofemoral ligament.

Graphical representation of peak contact pressure changes between the intact, cut, overtensioned (OT), and laterally released (LR) knees with increased pressure after overconstrained MPFL graft. Error bars represent standard deviation. *Significantly different compared with the intact state (P < .05). **Significantly different compared with the OT state (P < .05). MPFL, medial patellofemoral ligament.
Discussion
The results of our study demonstrate 2 important aspects of MPFL reconstruction surgery. First, our data support previous biomechanical evidence that an OT graft can lead to significantly increased mean and peak contact pressure across the PFJ in some knees. Second, when mean and peak contact pressure increased with an OT MPFL graft, the addition of an LRR was associated with a significant decrease in these pressures. These data suggest that LRR is biomechanically viable for decreasing contact pressure in MPFL reconstruction.
Our observation that some knees did not show increased pressure after overtensioning may represent a limitation of our biomechanical model or subtle anatomic variations. Previous studies have demonstrated the ability of an overtightened MPFL reconstruction, leading to increased contact pressure across the PFJ. 1,14,18 Our study sought to investigate the effect of LRR in the setting of increased contact pressures. Therefore, we chose to analyze the changes in pressures after a lateral release in those knees that demonstrated increased pressures.
We did not consistently demonstrate increased mean and peak contact pressures after overtensioning at higher flexion angles and had varying results after a lateral release at 45° and 60°. Additionally, transection of the MPFL significantly affected mean pressure only at 30° and 45°. This finding is consistent with the results from previous biomechanical studies demonstrating that MPFL integrity and increased graft tension had a greater effect at lower angles of flexion. Forces required to translate the patella laterally have been shown to rise with increasing flexion angles. 2,10,14 MPFL tension may play a lesser role in PFJ stability and, similarly, may play a smaller role proportionately in joint reaction forces at higher degrees of flexion. 7,14
We chose to investigate both mean and peak contact pressures in our model. One concern of overtensioning is that dramatic point loading could lead to patellofemoral chondral wear at an accelerated rate. Computational studies have shown that in an OT construct, medial pressures rise significantly more than lateral pressures. 15 Although we did not distinguish laterality in our model, we did observe changes in mean and peak pressures similar to those of the computational model. Increased medial pressure is of particular concern in that recurrent instability episodes may be associated with frayed or damaged medial cartilage. Further insult, especially medial point loading, could lead to or accelerate progressive degenerative changes.
The addition of an LRR to knees with an OT MPFL graft did not restore contact pressure to that of the intact state, and the clinical relevance of the observed mean and peak pressure changes is unknown. As shown in the current data and in a previous report, 7 an OT MPFL graft can lead to increased contact pressures across the PFJ. In the short term, this could lead to altered kinematics and pain. In the long term, increased pressure and point loading could predispose the PFJ to early degenerative changes. However, the magnitude of effect that an LRR would have in mitigating progression of degenerative change on an OT MPFL is unknown.
Our model suggests that contact pressure with an OT graft in MPFL reconstruction can be reduced with the addition of an LRR. Limited LRR has been shown to have some utility in the setting of lateral patella overload. 9,17 We were able to establish that mean and peak pressures were lowered at certain flexion points, but our model did not allow determination of whether LRR medializes the center of contact and, further, point loads an already at-risk medial compartment. Additionally, it is not known whether the alteration in pressures with an OT graft and LRR observed in this study was maintained after graft incorporation and remodeling.
This study was limited by several factors. These biomechanical results represent conditions at time zero and do not account for natural stretch and remodeling of a graft over time, in vivo. Our study was performed using cadaveric specimens without knowledge of pre-existing patellofemoral disease or risk factors for patellar instability. The patella tendon was loaded at 200 N, which approximates knee extension against gravity. Weightbearing loads, which may enhance patellar stability, were not tested. The weight chosen to simulate overtensioning of the graft has not been associated with clinical overtensioning, but it resulted in significantly increased contact pressure in pilot specimens and provided consistent tensioning across all test conditions. Furthermore, we did not look at the change in location of PFJ contact pressures, and we did not test any grafts that were not OT. Further research into these questions could help illuminate how the magnitude and location of pressures change through a range of motion in the PFJ compared with a more anatomic tension. Although we took great care in preserving the medial and lateral soft tissue structures for testing purposes, violation of the superior capsule to insert the sensor may have altered knee kinematics. Our construct did not produce increased pressure in all knees after overtensioning. Although this could be a limitation of the model, it may also represent subtle anatomic variances in PFJ morphology.
Conclusion
In knees that demonstrated increased contact pressures after an OT graft, LRR led to a statistically significant decrease in pressure across the PFJ. In this biomechanical model, LRR was effective in reducing PFJ pressure after overtensioning the PFJ in MPFL reconstruction.
Footnotes
Acknowledgment
The authors thank Lyn Camire Jones, MA, ELS, of our department, for editorial support.
Final revision submitted September 15, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Zimmer Biomet donated suture anchors for study. R.G.L. has received consulting fees from Miach and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.