
Abstract
Background:
Medial patellofemoral ligament reconstruction (MPFLR) is a standard treatment for patellofemoral instability. Concomitant lateral retinacular release (LR) or lateral retinacular lengthening (LL) is considered for patients with a tight lateral retinaculum (as determined by examination under anesthesia); however, the literature is limited on the frequency of these procedures and the factors associated with their incidence.
Purpose:
To investigate associations between demographic characteristics, physical examination findings, and radiologically measured patellofemoral parameters with LR/LL in patients undergoing primary MPFLR.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A prospective multicenter cohort study database was queried for patients who underwent primary MPFLR between January 2017 and July 2022. A total of 23 surgeons from academic centers across the United States performed the procedures. Radiologic parameters, concomitant procedures, and pre- and intraoperative physical examination findings were assessed between patients with and without LR/LL using the chi-square test, independent t test, or Mann-Whitney U test, as appropriate. Binary logistic regression was used to perform a multivariable analysis of factors associated with LR/LL.
Results:
Of 428 patients (mean age, 16.7 ± 4.2 years, 64.5% women), 22.9% underwent LR (13.6%) or LL (9.3%). Those who underwent LR/LL were more frequently men (44% vs 23%; P = .049), had lower Beighton scores (2.6 ± 2.7 vs 3.8 ± 2.9; P < .001), and their surgeons were more likely to have completed a sports fellowship (82.7% vs 64.8%; P < .001) compared with those who did not undergo LR/LL. On preoperative examination, patients with LR/LL more often exhibited patellar apprehension (92.6% vs 81.2%; P = .008) and pathologic lateral patellar translation (62.2% vs 49.1%; P = .012). Intraoperatively, patients with LR/LL more often dislocated in extension during examination under anesthesia (70.4% vs 57%; P = .017) and underwent a tibial tubercle osteotomy (TTO) (35.7% vs 9.4%; P < .001). A total of 168 patients had preoperative imaging measurements available, and patients with LR/LL showed greater patellar tilt (24.1°± 7.7° vs 18.5°± 16.7°; P < .001).
Conclusion:
Approximately 23% of patients who underwent MPLFR from a large multicenter cohort underwent LR/LL. The LR/LL appears to be associated with less ligamentous laxity, lateral patellar apprehension, surgeon completion of a sports fellowship, and concomitant TTO. These data may elucidate some of the relative factors associated with performing these procedures in patients undergoing primary MPFLR.
Keywords
Medial patellofemoral ligament reconstruction (MPFLR) has evolved over the past decade into a standard-of-care treatment for patients with recurrent patellofemoral instability (PFI). PFI may be associated with a constellation of underlying patient-based morphologic features—including patella alta, trochlea dysplasia, femoral anteversion, external tibial torsion, patellar tilt, and lateral patellar displacement. 15 For those patients with high degrees of patellar tilt or abnormal parameters of patellar lateralization, a concomitant lateral retinacular release (LR) or lateral retinacular lengthening (LL) may also be recommended to allow for more patellar medialization in conjunction with a realignment or stabilization procedure. 10 This can improve patellar tracking and/or decrease the risk of a recurrent instability event. Although the literature on the precise role and outcomes after LR/LL is quite variable, the popularity of the lateral release as a procedure diminished significantly after reports suggested elevated rates of postoperative recurrent PFI episodes following isolated LR.4,18 Some surgeons currently perform the procedure in the setting of MPFLR to improve patellar tracking and decrease potential lateral patellofemoral chondral wear.2,16,24
Limited research exists on the exact frequency and indications for performing an LR or LL in conjunction with MPFLR. The classic approach to considering an LR or LL in conjunction with an MPFLR is primarily based on the physical examination and magnetic resonance imaging (MRI) assessment of the patella's position in full extension. If the patella is not able to be centralized in the trochlea groove, due to tight lateral structures, then LR/LL may be indicated. In addition, if a centrally located patella cannot be tilted so that the lateral edge of the patella moves away from the lateral trochlea, then LR/LL can be considered.
The present study aimed to assess the frequency of LR/LL procedures performed in conjunction with MPFLR in a multicenter study of patients with PFI undergoing surgery by a large group of surgeons, demonstrating both geographic and training-based diversity, and to identify associations between demographic characteristics, physical examination findings, and patellofemoral morphology, as assessed by well-established radiologic parameters. The study hypothesis was that greater patellar tilt angles and lower ligamentous laxity scores would be associated with the addition of LR/LL in conjunction with MPFLR.
Methods
This study included a subcohort of patients, using predefined research questions and hypotheses for inclusion, from the comprehensive database of the prospective, multicenter Justifying Patellar Instability Treatment by Results (JUPITER) cohort study. This was an institutional review board-approved study. A total of 23 different surgeons from academic centers in all 5 major geographic regions in the United States performed the procedures. All but 1 surgeon (who was not fellowship trained) underwent fellowship training in sports medicine (39.1%), pediatric orthopaedic surgery (30.4%), or both (26.1%). The mean time in practice (calculated from 2024 unless retired) was 16.8 ± 8 years (range, 6-36 years). Patients who underwent primary MPFLR from January 2017 to July 2022 for PFI after a single patellar dislocation were included. The exclusion criteria were revision PFI procedures or those cases not including a MPFLR; or those with congenital instability (fixed dislocation present from birth), syndromic instability, habitual or fixed patellar dislocation, no recorded pre- or intraoperative examination (including Beighton score); no available baseline screening form or known number of PFI events; and those without established level of skeletal maturity (defined as either mature or immature by a musculoskeletal radiologist). Those patients undergoing trochleoplasty or distal femoral osteotomy were also excluded.
Demographic characteristics collected were age at the time of surgery, sex, and body mass index (BMI). Concomitant surgical procedures and pre- and intraoperative physical examination findings recorded in a standardized fashion per the multicenter study group—including Beighton score to assess patient ligamentous laxity—were evaluated. A Beighton score of ≥4 was used to denote hypermobility or pathologic ligamentous laxity; patellar translation of ≥3 quadrants was considered pathologic laxity, whereas ≤1 quadrant was regarded as pathologic tightness. 19 While LR and LL were tallied separately, for statistical comparison, these were combined into 1 group titled LR/LL. The specific indications for LL/LR were not recorded in this prospective study. All data were retrieved from the PatientIQ data collection platform.
Radiographic Parameters
Radiographic parameters were measured by a single musculoskeletal radiologist at each participating institution using standardized measurement techniques in this prospective registry as previously described by Fabricant et al. 7 These included skeletal maturity status (mature or immature), Caton-Deschamps index, trochlear bump (mm), sulcus angle, tibial tubercle-trochlear groove (TT-TG) distance (mm), sulcus angle, lateral patellar displacement (mm), and patellar tilt angle. The Caton-Deschamps index was measured on a lateral plain radiograph as the ratio of the distance from the lower edge of the patellar articular surface to the anterosuperior angle of the tibia and the length of the articular surface of the patella. The trochlear bump represented the distance between the highest point of the trochlea and a line along the anterior femoral cortex on a lateral radiograph. The sulcus angle is the angle between lines extending from the highest points of the medial and lateral femoral condyles to the deepest aspect of the trochlear groove on the most cranial axial MRI slice covered with articular cartilage. The TT-TG was measured on axial MRI on the most caudal slice with intact subchondral bone and full cartilage coverage. Lateral patellar displacement was taken as the horizontal distance of the medial patella on axial MRI from a line perpendicular to the posterior femoral condyles and passing through the anterior-most point of the medial femoral condyle. The patellar tilt was assessed on the same axial MRI sequence and was measured as the angle between a line across the posterior femoral condyles and a line through the midpoints of the medial and lateral patella.
Surgical Technique
The surgical technique for LR and LL procedures varied across institutions; therefore, a specific method is not presented. The general approach for an LL is described by Hayden et al, 11 and a process for an LR is described by Wang et al. 28
Statistical Analysis
Normality of continuous variables was assessed using the Shapiro-Wilk test. Continuous variables were compared using independent t tests or Mann-Whitney U tests, as appropriate, and categorical variables were compared using the chi-square test or the Fisher exact test. In all tables, categorical variables are presented as numbers (percentages) and continuous variables as mean ± standard deviation (range). Binary logistic regression was used to perform a multivariable analysis of factors associated with LR/LL—including demographic characteristics (age and sex) and those achieving P < .1 significance in the univariable analysis. These are reported as odds ratios (OR) and 95% confidence intervals. All analyses were performed with SPSS Statistical Analysis Software, Version 24 (IBM), with a significance threshold set at P < .05.
Results
A total of 428 patients were eligible for inclusion in this study (Table 1). The mean age was 16.7 ± 4.2 years, and 276 patients (64.5%) were women. The mean BMI was 24.6 ± 5.9 kg/m2, and 302 (70.6%) patients were skeletally mature at the time of surgery. A total of 22.9% of patients underwent LR or LL, with 13.6% undergoing LR and 9.3% undergoing LL. There were no significant differences in age, BMI, number of preoperative instability events, or skeletal maturity status between LR/LL patients and non-LR/LL patients (Table 2). Women were less likely to receive an LR/LL (67% vs 56.1%; P = .049).
Patient Characteristics a (N = 428)

BMI, body mass index.
Patient Characteristics Based on Procedure a (N = 428)

Bold P values indicate statistical significance. Data are presented as mean ± SD or n (%). BMI, body mass index; LL, lateral retinacular lengthening; LR, lateral retinacular release; TTO, tibial tubercle osteotomy.
On preoperative examination, LR/LL patients more frequently exhibited patellar apprehension (92.6% vs 81.2%; P = .008) and lateral patellar translation of ≥3 quadrants (62.2% vs 49.1%; P = .012) when compared with non-LR/LL patients (Table 3). LR/LL patients also had lower Beighton scores (2.6 ± 2.7 vs 3.8 ± 2.9; P < .001) compared with non-LR/LL patients. A higher proportion of female patients also had hypermobility (59.4% vs 28.9%; P < .001). Intraoperatively, the LR group more frequently demonstrated the ability to manually dislocate in extension (during examination under anesthesia) (70.4% vs 57%; P = .017).
Physical Examination a
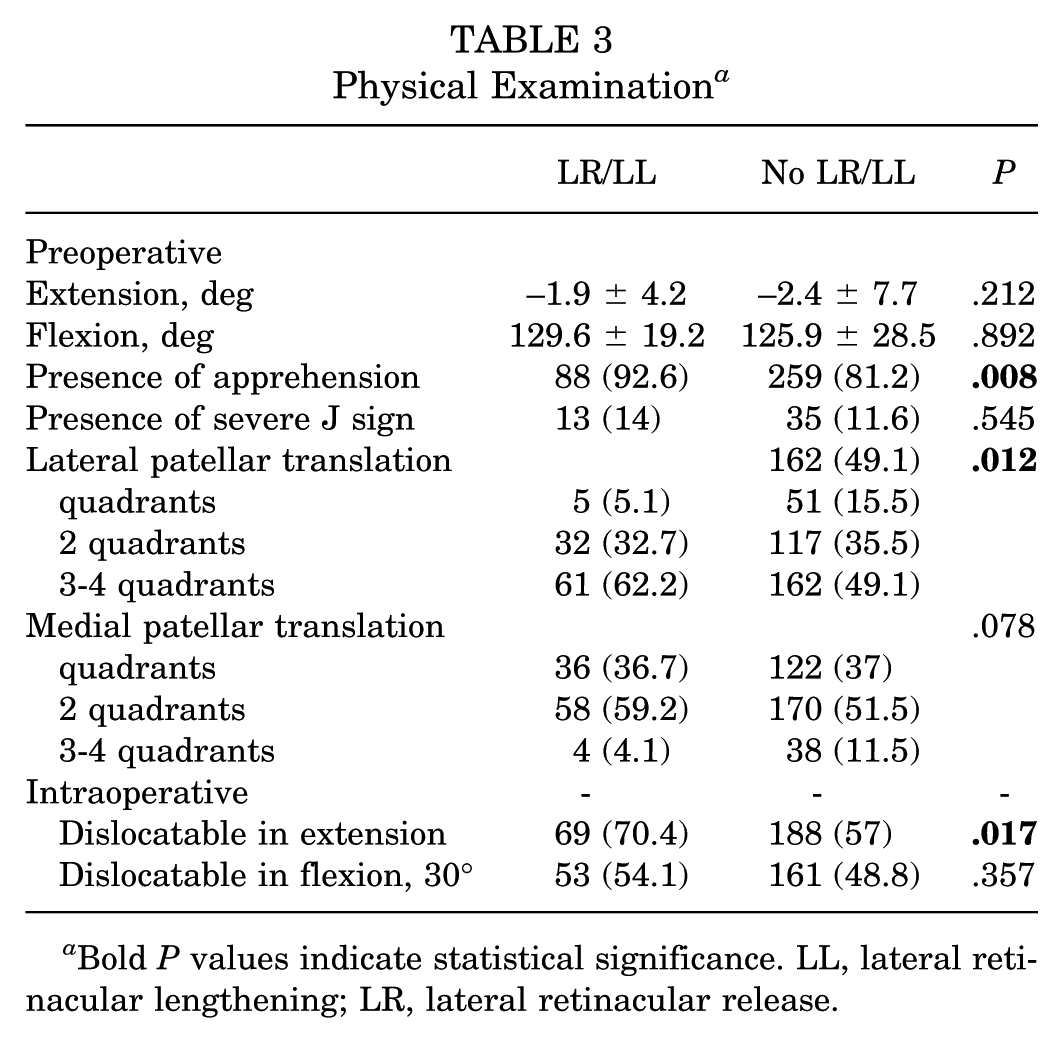
Bold P values indicate statistical significance. LL, lateral retinacular lengthening; LR, lateral retinacular release.
The most common concomitant procedures to MPFLR overall were patellofemoral chondroplasty (41.8%), loose body removal (17.3%), and tibial tubercle osteotomy (TTO) (15.4%) (Table 4). LR/LL patients were more likely to undergo concomitant TTO (35.7% vs 9.4%; P < .001). LR/LL was more likely to be performed if the surgeon had completed a sports fellowship (82.7% vs 64.8%; P < .001).
Other Surgical Procedures Performed a

Others: microfracture or osteochondral fracture treatment (N = 6; 1.4%). TTO, tibial tubercle osteotomy.
In multivariable analysis (P < .001) (Table 5), a pathologic Beighton score ≥4 (OR, 0.48 [95% CI, 0.28-0.83]; P = .009), preoperative apprehension (OR, 2.40 [95% CI, 1-5.75]; P = .049), sports fellowship training (OR, 2.99 [95% CI, 1.58-5.65]; P = .001), and performing a TTO (OR, 5.23 [95% CI, 2.77-9.88]; P < .001)] were associated with LR/LL. In subanalysis of patients with isolated MPFLR (without concomitant TTO), the LR/LL subgroup had less passive extension (–1.1 ± 4.4 vs −2.2 ± 7.9; P = .027), higher rates of patellar apprehension (91.7% vs 80.2%; P = .035), lower mean Beighton score (2.9 ± 2.7 vs 3.6 ± 2.9; P = .048), increased patellar tilt angle (24.2°± 8.3° vs 17.9°± 17.4°; P < .001), and sports fellowship training (81% vs 64.5%; P = .012) compared with the non-LR/LL subgroup.
Multivariable Analysis a

Data are presented as OR (95% CI). Bold P values indicate statistical significance. OR, odds ratio; TTO, tibial tubercle osteotomy.
Defined as ≥3 quadrants of lateral patellar translation.
A total of 168 patients with available preoperative plain radiographs and MRI measurements were included in the radiologic evaluation (Table 6). There were no differences in baseline demographic characteristics (age, sex, and BMI) between patients with available imaging measurements and those without (P > .05 for all). Patients in the LR/LL group had greater patellar tilt angle (24.1°± 7.7° vs 18.5°± 16.7°; P < .001). There were no differences in Caton-Deschamps index, sulcus angle, lateral patellar displacement, TT-TG, or trochlear bump between the 2 groups (P > .05). No multivariable analysis was performed on the radiologic parameters, given the small number of patients in this subset who underwent LR/LL (N = 22) and the standard required 10 events per variable in logistic regression analyses. 26
Radiographic Evaluation a (N = 168)
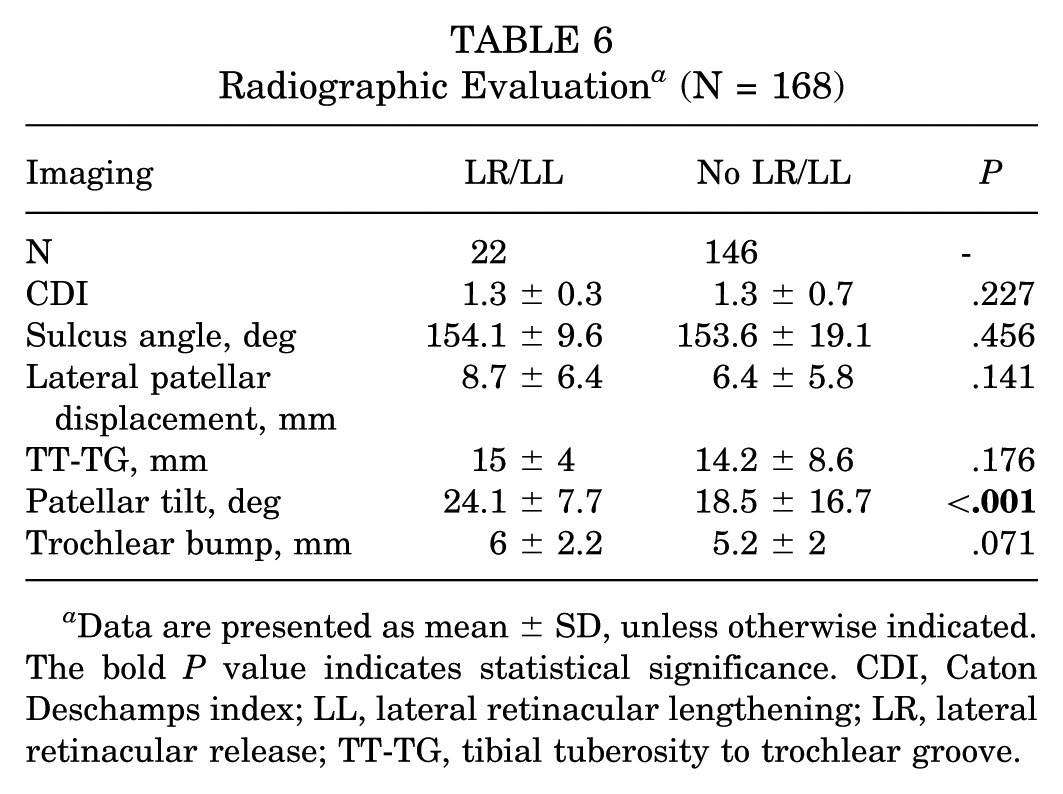
Data are presented as mean ± SD, unless otherwise indicated. The bold P value indicates statistical significance. CDI, Caton Deschamps index; LL, lateral retinacular lengthening; LR, lateral retinacular release; TT-TG, tibial tuberosity to trochlear groove.
Discussion
This stratified analysis, derived from a large, multicenter prospective cohort study of PFI, demonstrated a relatively high frequency of LR/LL procedures performed (~25%) for patients undergoing primary MPFLR. The addition of LR/LL procedures was associated with the addition of concomitant TTO, lower ligamentous laxity, preoperative apprehension, and sports medicine fellowship training by the surgeon. The dominant preoperative radiologic feature in the LR/LL cohort was a higher patellar tilt angle, which confirmed our hypothesis.
Concerns about iatrogenic medial instability, even with MPFLR, have prompted many surgeons to favor LL over LR. The main advantages of LL over LR are that it maintains the integrity of lateral soft tissue structures and joint containment, which may prevent a notable lateral joint defect, the extravasation of intra-articular joint fluid and hemarthrosis from tracking extra-articularly, and global postoperative periarticular swelling. 27 Other biomechanical studies illustrated that the lateral retinaculum, in addition to serving as a lateral soft tissue restraint to medial translation of the patella, also paradoxically served as a lateral restraint to lateral translation. Even as early as 2004, a survey of the International Patellofemoral Study Group reported that <2% of surgeons would perform an isolated lateral release, with the most common indications being lateral tightness and patellar tilt on examination/imaging, as observed in our study. 8
Lateral retinacular tightness is classically described as (1) a patellar tilt angle of >20° and/or (2) an inability to evert the patella to neutral in full knee extension.6,11 These criteria have therefore become common indications for concomitant LR/LL when performing PFI surgery, which now, most commonly, revolves around MPFLR. Parikh et al 25 and Hinckel et al 12 have advocated for its use when performing additional bony realignment procedures or in patients with fixed or obligatory patellar dislocations. However, caution must be exercised when considering the cause of lateral patellar tilt, as a dysplastic trochlea and medial insufficiency may also contribute to this observation. A recent large national database study by Kamalapathy et al 13 of >2000 patients observed that the rate of concomitant LR/LL decreased from 32% in 2010 to 18% in 2018. This study mirrors these findings, as an LR/LL was performed in ~25% of patients undergoing primary MPFLR, with approximately 60% of these being traditional LR.
The precise clinical benefit, from an outcome's perspective, of LR/LL in conjunction with an MPFLR has not been well established in the recent literature. However, a small patient-reported outcome (PRO) study and systematic review have attempted to assess its effect.20,21 A cadaveric study by Gallagher et al 9 reported that LR reduced patellofemoral contact pressures after an overtensioned MPFLR. Conversely, a long-term in vivo follow-up study has further found that concomitant lateral release does not decrease the rate of patellofemoral arthritis at 10 years postoperatively. 23 A recent prospective cohort study by Wang et al 28 recommended a concomitant LR in patients undergoing MPFLR, observing higher 1-year postoperative Lysholm and International Knee Documentation Committee scores for those who also underwent LR, but did not assess minimum clinically important differences. 28 Additionally, there is concern that despite potential patellar tracking improvements, LR may lead to decreased force required to displace the patella laterally. 1 A finite element analysis by Kheir et al 14 demonstrated that despite decreases in patellofemoral contact pressures with lateral release, there was ironically a higher risk of lateral patellar displacement and potential lateral patellar instability. Exactly how this interplay of decreased contact forces versus lateral translational vulnerability affects patients postoperatively remains incompletely explored.
Patients in the present study who underwent LR/LL demonstrated greater preoperative lateral patellar translation on physical examination, in univariable analysis, compared with those who did not undergo LR/LL. This may be, in part, due to tighter lateral structures (necessitating a release) and deficient medial soft tissues, leading to an earlier sensation of apprehension with less force required by the examiner. 5 This corresponds with the observation of higher rates of ability to dislocate the patella in extension during examination under anesthesia in the patients with LR/LL.
Increased radiologic patellar tilt angle and lateral patellar displacement measurements have also been previously discussed as indications for performing an LR/LL, due to the association between a tight lateral retinaculum and PFI. 15 Levy et al 17 recommended the addition of an LR procedure when the patellar tilt angle is >20°, mainly based on older data by Dejour. 6 This recommendation is consistent with the observations in the present study, as patients who underwent LR/LL had a mean patellar tilt of 24°, compared with 18° in those who did not undergo LR/LL. 17 Surgeons in this cohort study may therefore utilize the LR/LL in an attempt to improve patellar tracking and reduce the rate of recurrent PFI, specifically in patients with elevated patellar tilt over those with more evidence of trochlear dysplasia. In our population, nearly 40% of patients who underwent LR also had a TTO performed, despite similar TT-TG measurements between those who did and did not undergo LR or LL. Patellar tracking should be assessed after TTO to determine whether an LR/LL is required.
Ligamentous laxity, as with other forms of pathologic joint instability, is another well-established underlying risk factor for PFI. 22 The present study demonstrates that patients with higher Beighton scores, or scores that placed them into a category of hypermobility, were significantly less likely to undergo an LR procedure. Limited past literature exists on the association between ligamentous laxity and the use of LR/LL, although hyperlaxity is generally associated with poorer PFI outcomes after isolated LR. 3 This observation may result from tighter lateral structures in patients with lower or normal scores for ligamentous laxity, with this subpopulation potentially benefiting from LR/LL to reduce patellar tilt and obtain more normal patellar tracking. Conversely, patients with Beighton scores ≥4 are more likely to have loose lateral soft tissues that do not provide a strong lateralizing force on the patella. Lastly, surgeon training may have influenced the decision to perform an LR/LL procedure, as a greater proportion of surgeons with formal sports fellowship training added an LR/LL to the MPFLR than those who received pediatric orthopaedic fellowship training. The precise reasons for this difference are unclear and may have been driven by a small number of individual surgeons in either group who are dogmatic about the use, or lack of use, of LR/LL procedures, based on their training mentors’ perspectives or anecdotal experience. However, because children tend to have greater ligamentous laxity than adults, pediatric orthopaedic surgeons may be less accustomed to adding LR/LL to PFI surgeries. As the multivariable regression analysis controlled for age-based factors, this concept clearly warrants further investigation in larger cohorts.
Limitations
Various study limitations should be noted. First, this study does not clearly establish the absolute or relative indications for LR/LR, nor does it elucidate, based on patient outcomes, the optimal LR/LL indications. Instead, the study explores the associations between a variety of salient pre- and intraoperative demographic, physical examination, and imaging variables and the decision to perform an LR/LL. As there is little literature regarding the frequency of LR/LL or associations with the variables identified above in a largely adolescent patient population, these results may inform surgeons of factors that are commonly applied to indicate a LR/LL, with the study findings reflecting the experience, both anecdotal and evidence-based, of a group of high-volume PFI surgeon-investigators, who contributed patients to this study. Future studies may identify specific parameters associated with successful outcomes (eg, lower rates of postoperative recurrent PFI) after an LR/LL procedure. Another limitation is that this study included only individuals undergoing primary MPFLR; therefore, extrapolation to revision surgical settings should not be attempted. The large number of patients excluded from the final analysis in this study reflects the authors' concerted effort to ensure that comprehensive data were collected and that the most accurate reporting of variables associated with LR/LL was achieved. Specifically, patients undergoing trochleoplasty or distal femoral osteotomy, who underwent LR/LL at disproportionately high rates and/or had underlying malalignment atypical of most patients with PFI, were excluded. We chose to include patients undergoing TTO because it is frequent in patients with PFI. Third, LR and LL procedures were combined for statistical analysis, both to enhance the statistical power of the substratified analyses and because selection between these variants is almost entirely due to surgeon preference and/or training. Importantly, future studies will focus on a more thoughtfully designed prospective comparison of these 2 procedures. Fourth, due to the multicenter design of the study, without a standardized preoperative work-up and the requirement for large amounts of data entry, not all patients had imaging data available. Therefore, a subcohort analysis was performed to identify radiographic parameters associated with LR in a relatively smaller group of patients, which could have been subject to selection bias. Finally, because this study was conducted at a time when medium-term PRO measures were not yet available, these measures would not allow more informative associations between the LR/LL procedures and clinical results. Future publications with a central focus on PROs are critical to the overall JUPITER initiative and will build on the current foundation, which reveals key practices and thought-provoking insights into variables that are important to consider for patients with PFI.
Conclusion
In the present large multicenter study of >400 patients, approximately 23% of patients undergoing primary MPFLR underwent LR or LL. The addition of such a concomitant procedure was associated with less ligamentous laxity, a positive preoperative lateral patellar apprehension sign, elevated radiographic patellar tilt, surgeon sports medicine fellowship training, and the addition of concomitant TTO. These data may provide surgeons with a sense of current relative indications for performing lateral retinacular procedures in patients undergoing primary MPFLR.
Footnotes
Joshua T. Bram, MD (Hospital for Special Surgery, New York, New York, USA); Emilie Lijesen, BS (Hospital for Special Surgery, New York, New York, USA); Daniel W. Green, MD (Hospital for Special Surgery, New York, New York, USA); Benton E. Heyworth, MD, PhD (Boston Children's Hospital, Boston, Massachusetts, USA); Philip L. Wilson, MD (Texas Scottish Rite Hospital for Children, Dallas, Texas, USA); Beth E. Shubin Stein, MD (Hospital for Special Surgery, New York, New York, USA); Shital N. Parikh, MD (Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA).
Collaborating members of the JUPITER GROUP: Eric J. Wall, MD (Cincinnati Children's Hospital Medical Center, Cincinnati, OH, USA); Adam B. Yanke, MD, PhD (Rush University Medical Center, Chicago, IL USA); Jacqueline M. Brady, MD (Oregon Health and Science University, Portland, OR, USA); Lauren H. Redler, MD (Columbia University, New York, NY, USA); Jack Farr, MD (OrthoIndy, Indianapolis, IN, USA); Sabrina M. Strickland, MD (Hospital for Special Surgery, New York, New York, USA); Peter D. Fabricant, MD, MPH (Hospital for Special Surgery, New York, NY, USA); Jason L. Koh, MD (Northshore University, Chicago, IL, USA); Yi-Meng Yen, MD, PhD (Boston Children's Hospital, Boston, Massachusetts, USA), Dennis Kramer, MD (Boston Children's Hospital, Boston, Massachusetts, USA), Matthew Milewski, MD (Boston Children's Hospital, Boston, MA USA); Marc Tompkins, MD (TRIA orthopedics, Minneapolis, MN, USA), Caitlin Chambers, MD (TRIA orthopedics, Minneapolis, MN, USA); Henry Ellis, MD (Texas Scottish Rite Hospital for Children, Dallas, TX, USA), Philip Wilson, MD (Texas Scottish Rite Hospital for Children, Dallas, TX, USA); Robert Magnussen, MD (The Ohio State University, Columbus, OH, USA); Seth Sherman, MD (Stanford University, Stanford, CA, USA).
Final revision submitted July 26, 2024; accepted September 6, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.W.G. has received royalties from Arthrex Inc and Orthopediatrics; and consulting fees from Arthrex Inc. B.E.S.S. has received consulting fees from Arthrex and research support from ConMed. Her spouse has received consulting fees and royalties from Arthrex. S.N.P. has received consulting fees from Pfizer; support for education from CDC Medical; and speaking fees from Synthes GmbH. B.E.H. has received support for education from Arthrex, Kairos Surgical, and Pylant; and holds stock options in Imagen Technologies Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (2022-0649).