
Abstract
Background:
There is a paucity of literature evaluating the effect of cigarette smoking on outcomes in patients undergoing hip arthroscopy and labral reconstruction.
Purpose:
(1) To report minimum 2-year patient-reported outcome (PRO) scores for patients who smoke cigarettes and underwent primary hip arthroscopic labral reconstruction and (2) to compare these results with those of a propensity-matched control group of patients who have never smoked.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were collected for all patients who underwent primary hip arthroscopy for labral reconstruction between January 2011 and January 2019. Patients were eligible for the study if they indicated that they smoked cigarettes within 1 month of surgery and had minimum 2-year postoperative outcome scores for the modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), and the visual analog scale (VAS) for pain. The percentage of patients achieving the minimal clinically important difference (MCID) and patient-acceptable symptom state (PASS) was recorded. Rates of revision surgery were also documented. These patients were then propensity matched in a 1:3 ratio to patients who had never smoked (controls) for comparison.
Results:
A total of 20 patients (20 hips) were included with a mean follow-up of 39.9 ± 13.0 months and mean age of 41.4 ± 10.4 years. These patients demonstrated significant improvement from preoperatively to the minimum 2-year follow-up for mHHS, NAHS, and VAS (P < .05). They also achieved MCID for mHHS and VAS at acceptable rates, 70% for both. When outcomes were compared with those of 60 control patients (60 hips), patients who smoke demonstrated lower preoperative PRO scores but similar minimum 2-year postoperative PRO scores for mHHS and NAHS. Patients who smoke demonstrated lower rates of achieving PASS for mHHS (55% vs 75%) and NAHS (40% vs 61.7%) compared with controls; however, these findings were not statistically significant. Rates of secondary surgery were statistically significantly higher in the smoking group compared with controls (25% vs 5%; P = .031). Survivorship for the smoking patients was 80% and 98.3% for the control group. At the two-year mark survivorship was 90% for the smoking group and 100% for the control group (P = .06)
Conclusion:
While smokers can still derive significant improvement from hip arthroscopy, their ultimate functional outcome and rate of secondary surgeries are inferior to those of nonsmokers. As smoking is a significant and modifiable risk factor, we should continue to counsel smokers on smoking cessation prior to and after surgery
Despite declining rates of smoking among the US population, the Centers for Disease Control and Prevention estimates that about 40 million Americans smoke on a regular basis. 11 Smoking status has been well studied in the orthopaedic surgery literature, with already established deleterious effects of fracture healing, bone density, and healing times because of nicotine. 9,19,28,50 Recently, a growing body of literature has been establishing the effect of smoking on outcomes after hip arthroscopy. 9,38,43,69
Several recent studies have evaluated the effects of smoking on patients undergoing hip arthroscopy with labral repair compared with patients who had never smoked. Cancienne et al 9 evaluated minimum 2-year outcomes of patients undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS) and labral tears and established that patients who smoke cigarettes had lower postoperative outcome scores and lower rates of achieving clinically significant improvement after hip arthroscopy compared with patients who had never smoked. A similar study by Lall et al 43 found similar outcomes with smokers, demonstrating lower preoperative and postoperative outcome scores in patients undergoing hip arthroscopy. To date, no study has focused on and evaluated the influence of cigarette smoking on outcomes solely after hip arthroscopic labral reconstruction.
The purpose of this study was (1) to report minimum 2-year patient-reported outcome (PRO) scores for patients who smoke cigarettes and underwent primary hip arthroscopic labral reconstruction and (2) to compare these results with those of a propensity-matched control group of patients who have never smoked. The hypothesis was that patients who smoke and undergo primary hip arthroscopic labral reconstruction would demonstrate favorable results at the minimum 2-year follow-up but these results would be inferior to those of a matched control group of patients who had never smoked.
Methods
Patient Selection Criteria
Data were retrospectively collected and analyzed on all consecutive patients who underwent primary arthroscopic hip surgery for labral reconstruction during the study period between January 2011 and January 2019. Patients were eligible for the study if they indicated that they smoked cigarettes at their 1-month preoperative appointment; underwent hip arthroscopy and labral reconstruction; had preoperative data for the modified Harris Hip Score (mHHS), 2 Nonarthritic Hip Score (NAHS), 17 and visual analog scale (VAS) for pain 15 ; and had minimum 2-year follow-up data for the same scores. Patients were excluded if they had a prior hip surgery, had workers’ compensation, were unwilling to consent and enroll in the study, had a Tönnis osteoarthritis grade >1, or had a previous hip condition (ie, avascular necrosis, ankylosing spondylitis, Ehlers-Danlos syndrome, Legg-Calvè-Perthes disease, pigmented villonodular synovitis, or slipped capital femoral epiphysis).
All patients who smoke were advised to quit smoking and received a smoking cessation protocol that reviewed the potential consequences of smoking and the risk it may carry with surgery. Analysis was performed against a propensity-matched control group of patients who had never smoked, met the same exclusion and inclusion criteria, and underwent primary hip arthroscopy and labral reconstruction (never-smoking group).
Participation in the American Hip Institute Hip Preservation Registry
All patients included in this study participated in the American Hip Institute Hip Preservation Registry. This study conducts novel research, but previous papers may have used data on patients in this study. All data collection and reporting received institutional review board approval. All patients consented to this study.
Preoperative Evaluation and Radiographic Imaging
A detailed patient history, physical examination, and radiographic analysis were collectively utilized preoperatively by the senior author (B.G.D.) to evaluate surgical candidates. Patient variables, including age at surgery, body mass index (BMI), sex, operative side, and follow-up time, were collected. Gait, range of motion, strength, points of tenderness, and signs of FAIS or mechanical symptoms (snapping, catching, locking) were noted during physical examination. Radiographs were obtained and evaluated for signs of cam-type and pincer-type morphologies, acetabular dysplasia, and osteoarthritis in all patients using the anteroposterior pelvis, Dunn 45°, and false-profile views. 18 Radiographic measurements included the lateral center-edge angle (LCEA), 56 anterior center-edge angle (ACEA), 46 alpha angle, 6 Tönnis angle of acetabular inclination, 35 ischial spine protrusion, crossover sign percentage, and femoral head-neck offset. 33 Osteoarthritis was graded according to the Tönnis classification. 22 Cam morphology was defined as an alpha angle >55° 21,51 or a femoral head-neck offset <0.8 cm. 33 Evaluations of these images were performed using a Picture Archiving and Communication System (General Electric Healthcare). Previously published studies have demonstrated the reliability of radiographic measurements. 23,48 Magnetic resonance imaging or magnetic resonance arthrography scans were obtained on all patients before surgical indication and was used to identify intra-articular pathology, such as labral tears or chondral damage.
Surgical Indications
All patients underwent at least 3 months of nonoperative treatments. The following recommendations were advised: activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), intra-articular injections, and physical therapy. Patients were recommended for surgery by the senior author (B.G.D.) if nonoperative treatments were unsuccessful. 8,32
Surgical Technique
All arthroscopies were conducted by the senior surgeon (B.G.D.). Patients were positioned on a traction table in the modified supine position and were administered general anesthesia. 20,44 Anterolateral, distal anterolateral, and modified midanterior accessory portals were used to enter the hip joint. Additionally, a diagnostic arthroscopy and interportal capsulotomy were conducted. 47 During the procedure, the following intraoperative findings were recorded: labral tears, chondrolabral junction damage, acetabular and femoral damage, and ligamentum teres damage. Labral tears were graded using the Seldes guidelines. 54,65 Chondrolabral junction damage was measured using acetabular labrum articular disruption (ALAD). 67 Acetabular and femoral cartilage defects were assessed using Outerbridge classifications. 57 The Domb 7 and Villar 5 classifications were used to analyze ligamentum teres damage. LCEAs were used to determine if hips had pincer-type morphologies (LCEA, >40°) and required an acetabuloplasty >2 mm or a minor acetabular rim trimming to create the necessary bony bed for labral reconstruction healing. Patients were evaluated for cam-type morphology intraoperatively using fluoroscopy with the hip in 6 different positions, as previously described. 42 As a result, it was possible to detect cam-type morphology in this manner, which may have not been identified on the preoperative Dunn view radiograph. In cases of cam-type morphology (alpha angle, >55°), patients underwent a femoroplasty. 49,51,60 Capsular repair was performed in all patients without excessive stiffness, adhesive capsulitis, or insufficient capsular tissue. 16,27,37,58 Preoperative characteristics such as age, sex, and BMI also went into this multifactorial algorithm.
All labral tears in this study were reconstructed. The decision of whether to repair or reconstruct the labrum was made intraoperatively by the senior surgeon. Patients were considered for labral reconstruction if nonviable labral tissues were found during diagnostic arthroscopy. 25,70 Labral reconstruction was performed according to a previously published technique. 14,24,61 At the beginning of the study period, the senior surgeon used hamstring autografts; however, to decrease the risk of donor site morbidity, the protocol changed to hamstring allografts. Reliable results have been established in the literature for labral reconstruction using both autograft and allograft. 10,29,30,45 Once the decision was made to reconstruct the labrum, the nonviable, calcified, and/or irreparable labral tissue was debrided. Acetabular bone trimming was performed and took into account the patient’s LCEAs and ACEAs to avoid iatrogenic instability. 53 The graft was prepared and inserted into the joint. Either segmental or circumferential reconstructions were performed as dictated by the amount of irreparable labrum present. Traction was released in all cases to assess for restoration of the suction seal between the labrum and the femoral head.
Rehabilitation Protocol
The rehabilitation protocol included physical therapy for 3 months and started as early as 1 day after surgery. Patients were instructed to limit weightbearing activity (20 lbs [9.07 kg] of flat-foot weightbearing) using crutches and a brace for stability (DJO Global), which limited their flexion and extension to 90° and 0°, respectively, for 6 weeks postoperatively. In addition, patients were recommended to use a stationary bicycle daily for 8 weeks after surgery. Also, NSAIDs were prescribed to all patients twice daily for 4 weeks to promote heterotopic ossification prophylaxis.
Surgical Outcome Tools
Questionnaires with PRO scores were completed by patients preoperatively and postoperatively at 3 months, 12 months, and annually thereafter. PRO scores contained the mHHS, NAHS, VAS for pain, and patient satisfaction. 2,17,40,52 Questionnaires were administered to patients during clinic visits. Patients unable to complete the questionnaires during their clinic visits completed them via encrypted email or telephone interviews. For this study, PRO scores were assessed at the preoperative and minimum 2-year checkpoints (mean ± SD, 39.9 ± 13.0 months [smokers] and 35.0 ± 10.8 months [never-smokers]).
The minimal clinically important difference (MCID) was calculated following the distribution-based method created by Norman et al. 55 This method has consistently approximated results comparable to the anchor-based methods and has been recommended for use because of its simplicity and consistency. 64,66,68 Unique MCIDs were calculated for the study for the following PRO scores: mHHS (≥6.4 [smokers], ≥7.42 [never-smokers]); NAHS (≥8.49 [smokers], ≥6.68 [never-smokers]); and VAS for pain (≥0.83 [smokers], ≥1.26 [never-smokers]). The patient-acceptable symptom states (PASSs) have been defined in the literature for the mHHS and NAHS as ≥74 and 85.6, respectively. 12,13,63 The proportion of hips achieving the maximum outcome improvement satisfaction threshold (MOIST) for the mHHS (≥54.8%), NAHS (≥52.5%), and VAS for pain (≥55.5%) was calculated for each hip using the method described by Maldonado et al. 49 The proportions of patients achieving the MCID and MOIST were reported for the mHHS, NAHS, and VAS for pain. Additionally, the proportion of patients achieving the PASS was calculated for the mHHS and NAHS.
Statistical Analysis
Statistical analysis was performed using Microsoft Excel with the Real Statistics Add-in package (Microsoft Corp). Equality and normality of variance were calculated using the F test and the Shapiro-Wilk test. Significance in continuous data was calculated using the 2-tailed t test or its nonparametric equivalent. For categorical data, the Fisher exact test or chi-square test was used. Statistical significance was established at a P value of .05. An a priori power analysis was conducted to determine the number of hips required in each group to detect 80% power with a 1:3 matching ratio. The power analysis was calculated based on the expected mean difference in the mHHS of 8 points and SD of 10 points. 36 The calculation required that 17 hips in the smoking group and 51 hips in the never-smoking group were necessary to minimize type 2 errors.
Propensity Score–Matched Analysis
Eligible patients who smoke cigarettes were propensity score matched in a 1:3 ratio to patients who have never smoked based on age at the time of surgery, sex, and BMI. Smoker was defined by social history indicating smoking during an office visit within 1 month before the procedure, and never-smoker was defined by social history indicating never smoking but otherwise meeting all inclusion criteria. R (version 4.1.0; R Foundation for Statistical Computing) was used to propensity score match smokers and never-smokers to minimize the effect of potential confounding variables. 26 The groups were greedy matched without replacement according to age at the time of surgery, sex, and BMI. For this process of matching, hips in the control group can only be matched to study patients once. Previous studies have shown that the optimal method for group comparison is greedy matching without replacement. 1,3,4
Results
Patient Characteristics
Overall, 21 hips were eligible for the smoking study group after all inclusion and exclusion criteria were applied, and 20 of these hips in 20 patients (95.2%) had a 2-year follow-up and were included. The never-smoking group consisted of 60 patients (60 hips). The mean ages at the time of surgery of the smoking group and the never-smoking group were 41.4 and 42.5 years, respectively (P = .668), and the mean BMIs of the smoking group and the never-smoking group were 30.2 and 28.7, respectively (P = .293). Follow-up times were similar between groups, as demonstrated in Table 1.
Patient Characteristics a

a Values are presented as No. (%) or mean ± SD. BMI, body mass index.
Radiographic Measurements
The mean LCEAs in the smoking and never-smoking groups were 34.0° and 32.4°, respectively (P = .391). All radiographic measurements were comparable between groups, as listed in Table 2.
Preoperative Radiographic Measurements a

a Values are presented as No. (%) or mean ± SD (range). ACEA, anterior center-edge angle; LCEA, lateral center-edge angle.
Intraoperative Findings and Surgical Procedures
Intraoperative findings are recorded in Table 3, and surgical procedures are outlined in Table 4. All patients, 20 in the smoking group and 60 in the never-smoking group, received a femoroplasty (P > .999). Both groups exhibited similar intraoperative findings and surgical procedures.
Intraoperative Findings a

a Values are presented as No. (%). ALAD, acetabular labrum articular disruption; LT, labral tear.
Surgical Procedures a

a Values are presented as No. (%).
Surgical Outcome Tools
Both groups accomplished significant improvement from preoperatively to the minimum 2-year checkpoint for the mHHS, NAHS, and VAS for pain (P < .001); however, preoperative scores were lower in the smoking group compared with the never-smoking group for the mHHS (P < .002) and NAHS (P < .001). All PRO data are recorded in Table 5.
Patient-Reported Outcomes a

a Values are presented as mean ± SD (range). Bolding indicates a statistically significant difference between comparisons (P < .05). mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
The rates of achieving MCID, PASS, and MOIST for all recorded PRO scores were lower in the smoking group compared with the never-smoking group, but these differences did not reach statistical significance. The most notable difference was found in rates of achieving PASS for mHHS (55% [smokers] vs 75% [never-smokers]) and NAHS (40% [smokers] vs 61.7% [never-smokers]), which did not reach statistical significance. Data for the MCID, PASS, and MOIST are recorded in Table 6.
MCID, PASS, and MOIST Achievement Rates a

a Values are presented as No. (%). MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; MOIST, maximum outcome improvement satisfaction threshold; NAHS, Nonarthritic Hip Score; PASS, patient-acceptable symptom state; VAS, visual analog scale.
Secondary Surgeries
One hip (5.0%) in the smoking group and 2 hips (3.3%) in the never-smoking group underwent secondary hip arthroscopies (P > .999). Four hips (20%) in the smoking and 1 hip (1.7%) in the never-smoking group had total hip arthroplasties. All secondary surgeries reported occurred before 5 years after the initial date of surgery. All patients receiving a secondary surgery had their PRO scores omitted in postoperative and improvement calculations for the mHHS, NAHS, and VAS for pain. The rate of total hip arthroplasty and the overall revision rate were statistically significantly higher in the smoking group compared with the never-smoking group (P = .013 and P = .031, respectively). Survivorship for the smoking patients was 80% and 98.3% for the control group. At the two-year mark survivorship was 90% for the smoking group and 100% for the control group (P = .06).
The results of secondary surgeries are shown in Table 7. Survivorship analysis is depicted in Figure 1.
Revision Surgeries a
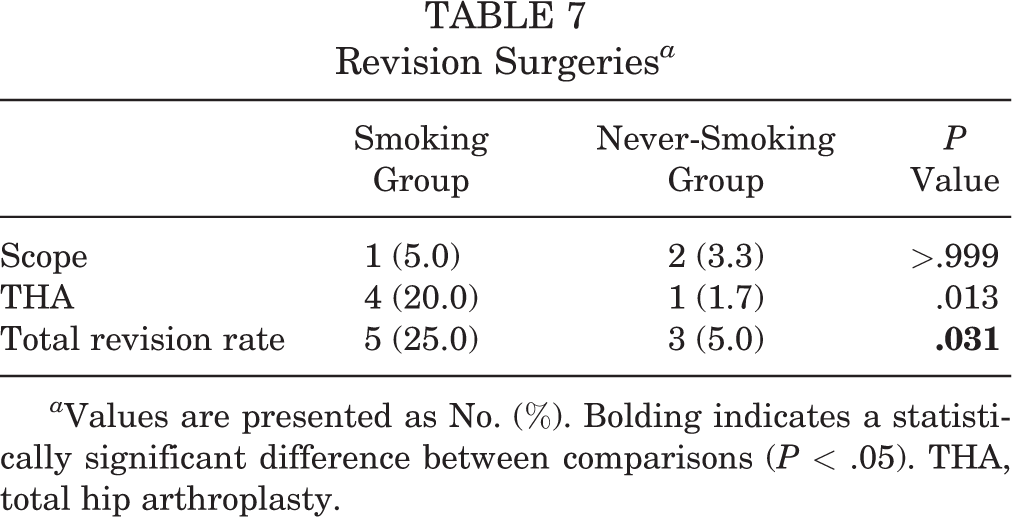
a Values are presented as No. (%). Bolding indicates a statistically significant difference between comparisons (P < .05). THA, total hip arthroplasty.
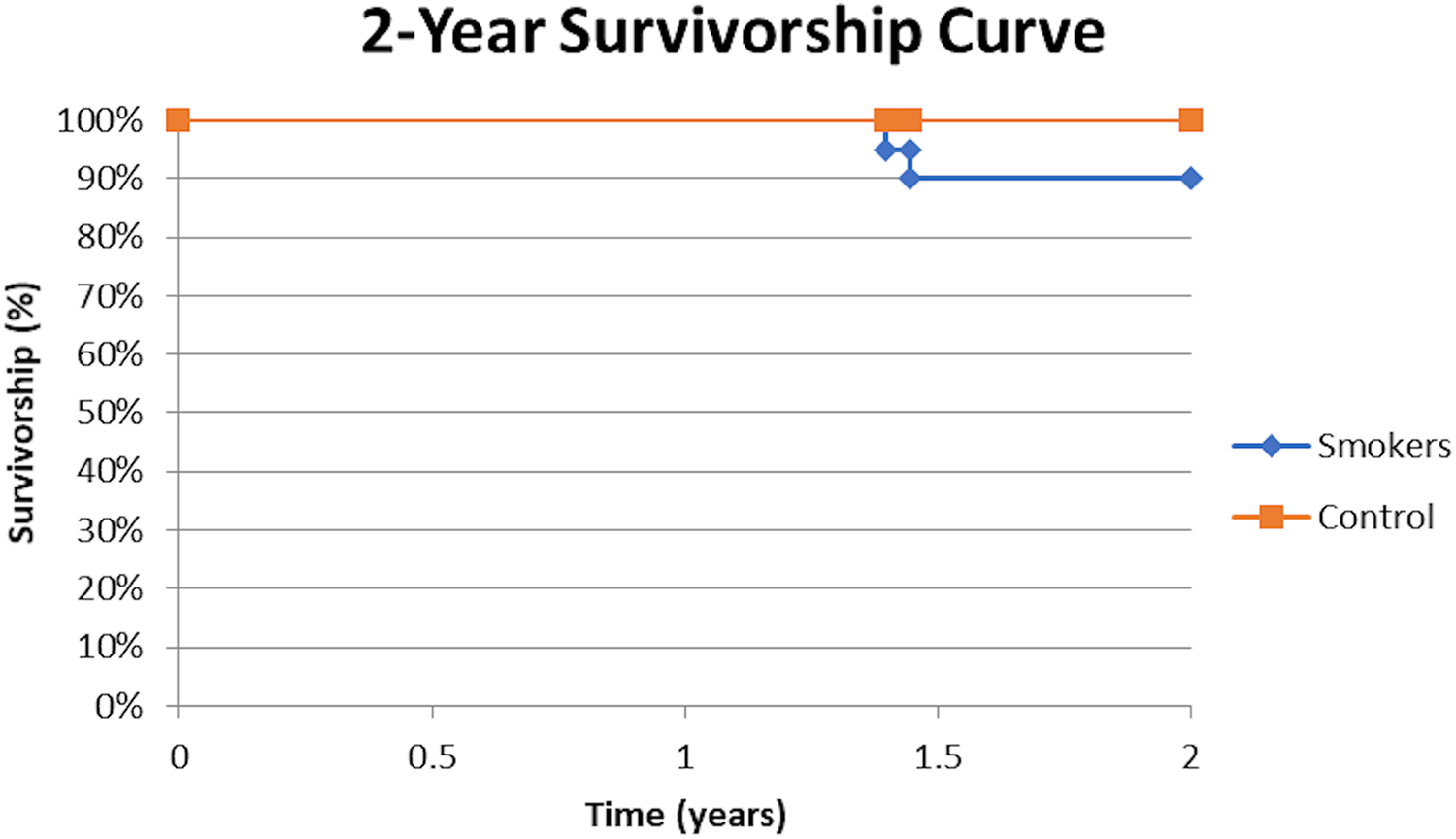
Survivorship curve depicting hip joint survival from conversion to total hip arthroplasty (THA) in smokers vs. never-smokers following primary hip arthroscopy with labral reconstruction.
Discussion
The main findings of this study were that current smokers who underwent primary hip arthroscopy demonstrated significant improvements in all recorded PRO scores at a minimum 2-year follow-up. When compared with a propensity-matched control group, patients who smoke had lower rates of achieving PASS for mHHS and NAHS, but this did not reach statistical significance. Further, patients who smoke underwent revision surgery at significantly higher rates compared with the control group of never-smokers.
The effect of smoking on perioperative complications and outcomes in other orthopaedic surgery procedures has been previously established. Cigarette smoking has been implicated in causing inferior outcomes after anterior cruciate ligament reconstruction as well as rotator cuff repair. 19,28,39,41,54 The effect of smoking status on outcomes of patients undergoing hip arthroscopy and labral repair has been established, but it has not been fully evaluated in patients undergoing labral reconstruction. 9,43 This study is the first to evaluate the effect of smoking in patients undergoing primary hip arthroscopy and labral reconstruction with a minimum 2-year follow-up.
The results presented in this paper are in line with previously reported literature in patients undergoing hip arthroscopy with labral repair. 9,43 Cancienne et al 9 evaluated minimum 2-year outcomes in 40 smokers undergoing primary hip arthroscopy and labral repair compared with a control group of never-smokers. They established inferior postoperative scores for Hip Outcome Score (HOS)–Activities of Daily Living, HOS–Sport Specific Subscale, increased pain levels, and lower odds of achieving MCID for HOS-Activities of Daily Living compared with patients who have never smoked. In a similar study, Lall et al 43 established that patients who smoke had lower PRO scores preoperatively compared with never-smokers at a minimum 2-year follow-up.
Prior studies have proposed a physiologic mechanism for how cigarette smoking leads to worse outcomes after hip arthroscopy and labral repair. 9 Nicotine found in the cigarettes is known to cause vasoconstriction and likely reduces blood flow and oxygen delivery to the labral tissue after repair, thus compromising healing potential. 9,62 Additionally, carbon monoxide from cigarette smoke favorably binds to hemoglobin and can inhibit oxygen delivery to labral tissue. 62 These effects could synergistically work to limit blood supply and oxygen delivery to labral tissue and thus inhibit its healing capacity. It is likely that labral reconstruction, which requires healing and incorporation of graft tissue, is subject to similar demands. Histological studies have confirmed that labral reconstruction allograft has shown signs of revascularization as early as 8 weeks postoperatively. 31 As a result, smoking in this critical early postoperative period may have detrimental effects on the revascularization process.
The effect of smoking on postoperative outcomes has been well studied in shoulder and knee arthroscopic procedures. 34,41,59 Notably, smoking was found to have a detrimental effect on outcomes after anterior cruciate ligament reconstruction, with patients who smoke demonstrating greater knee instability compared with patients who do not smoke. Further, patients undergoing rotator cuff repair showed significantly higher rates of failure compared with a matched nonsmoking group. 59 In addition, smoking has been identified as an independent risk factor for complications after undergoing shoulder arthroscopy and knee arthroscopy. 34 These results were similar to the findings presented in the current study, and although postoperative complications were not evaluated in this paper, this represents an area of future investigation.
This study has identified smoking as a modifiable risk factor for higher revision rates in patients undergoing primary hip arthroscopic labral reconstruction. This represents a modifiable risk factor for inferior outcomes that can help preoperative optimization of patients undergoing arthroscopic hip surgery, and current smokers should be counseled on the risks of nicotine use in the perioperative period. Further research is warranted to determine if cessation of smoking can establish similar outcomes to those of patients who have never smoked.
This study had several strengths. It was the first to compare cigarette smoking and never smoking in patients undergoing hip arthroscopic labral reconstruction. The study also used a propensity-matched control group to account for confounding variables and underwent an a priori power analysis to ensure adequate power. Further, several established PRO scores were used to assess patient outcomes, and clinical correlation was provided by evaluating rates of achieving MCID, PASS, and MOIST.
This study also had several limitations. This was a retrospective study design that carries inherent limitations. Next, impaired healing of the labral allograft by smoking status may not be evident until after the 2-year follow-up, and longer-term studies are needed to evaluate the durability of results. Further, smoking status was considered a binary yes/no variable, and data were not available to stratify patients based on amount of cigarette smoking. Additionally, the sample size was relatively small, and further studies with larger samples that are better powered to detect differences are warranted. Psychosocial factors correlated with smoking may have added a confounding factor to the study as well. Last, the study was performed at a single institution, and surgeries were performed by 1 high-volume hip preservation–trained surgeon. As a result, the findings of this paper may have limited generalizability, and the external validity of these results should be evaluated.
Conclusion
While smokers can still derive significant improvement from hip arthroscopy, their ultimate functional outcome and rate of secondary surgeries are inferior to those of nonsmokers. As smoking is a significant and modifiable risk factor, we should continue to counsel smokers on smoking cessation prior to and after surgery.
Footnotes
Final revision submitted October 5, 2021; accepted November 12, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. has received research support from Arthrex, the Kauffman Foundation, and Stryker; consulting fees from Adventist Hinsdale Hospital, Arthrex, Medacta, and Stryker; education payments from Arthrex, Breg, and Medacta; speaking fees from Arthrex; honoraria from Medacta; royalties from Amplitude, Arthrex, DJO Global, Medacta, Stryker, and Orthomerica; and hospitality payments from Zimmer Biomet and has had ownership interests in the American Hip Institute, Hinsdale Orthopaedics, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center. A.E.J. has received education payments from Medwest. D.R.M. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. B.R.S. has received grants from Arthrex and speaker fees from DJO Global. A.C.L. has received research support from Arthrex, Stryker, and Medacta; education support from Arthrex, Medwest, and Smith & Nephew; consulting fees from Arthrex and Graymont Medical; and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Advocate Health Care Institutional Review Board (reference No. 5276).