
Abstract
Background:
The retear rate after revision rotator cuff repair (rRCR) ranges from 50% to 90%. Patients who undergo primary RCR (pRCR) for large to massive rotator cuff tear (mRCT) also have unpredictable outcomes.
Purpose:
To compare the clinical outcomes after rRCR for a posterosuperior rotator cuff tear of any size with those after pRCR for mRCT and to identify the risk factors for poor outcomes and retear after rRCR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Among patients with posterosuperior cuff tear treated between 2010 and 2017, the clinical outcomes of 46 patients who underwent rRCR were compared with 106 patients who underwent pRCR for mRCT. Between-group differences in patient-reported outcomes (visual analog scale [VAS] for pain, VAS for satisfaction and American Shoulder and Elbow Surgeons [ASES] and Constant scores) at final follow-up were evaluated and compared with previously published minimal clinically important difference (MCID) values. Radiological outcomes were evaluated using magnetic resonance imaging or ultrasonography at a minimum 1-year follow-up. Multivariate linear regression analysis was performed to identify the risk factors for poor ASES score, and multivariate logistic regression analysis was used to assess the risk factors for retear after rRCR.
Results:
The mean follow-up was 26.4 months (range, 24-81 months). Although final VAS for pain, VAS for satisfaction, and ASES scores in the rRCR group were significantly worse than those in the pRCR group, the Constant score was similar between the groups. These differences in outcomes did not exceed the MCID threshold. The retear rate in the rRCR group was 50% compared with 39% for the pRCR group (P = .194). In the rRCR group, risk factors for worse ASES score were retear (P = .043; r = –11.3), lower body mass index (P = .032; r = 1.9), and lower preoperative VAS for pain (P = .038; r = 2.3), and risk factors for retear were preoperative high-grade fatty degeneration (Goutallier grades 3 and 4) of the supraspinatus muscle (P = .026; odds ratio, 5.2) and serum hyperlipidemia (P = .035; odds ratio, 11.8).
Conclusion:
Both study groups had similar clinical and radiological outcomes. Patients with symptomatic failed rotator cuff repairs having high-grade fatty degeneration of the supraspinatus muscle and/or serum hyperlipidemia had a greater likelihood of retear after rRCR.
The number of arthroscopic rotator cuff repairs (RCRs) performed in the past 2 decades has exponentially increased across the globe, with an estimated rise of 200% to 600% in the United States alone. 6,17,32 Despite advancements in clinical knowledge, operative technique, and rehabilitation, the rate of retear after repair of a rotator cuff tear (RCT) is highly variable and reported to be in the range of 5% to 94%. 10 While further treatment is not indicated in all patients with retear after RCR, those with persistent symptoms and loss of function may benefit from a revision surgery. 16,22 The operative options to treat such patients with failed primary RCR (pRCR) are a revision RCR (rRCR), tendon transfer procedure, superior capsular reconstruction, partial repair with balloon spacer insertion, or a reverse shoulder arthroplasty. Among these operative options, an arthroscopic rRCR is considered suitable for young, healthy, and active patients with failed RCR. 22
The operative treatment via rRCR for a failed previous cuff repair is more challenging than is pRCR because of the possible poor quality of the remaining tendon, adhesions, foreign bodies from the previous surgery, and less bone available for anchor fixation. The knowledge of improvement in pain and function and healing rate after rRCR is essential to guide the proper treatment and set realistic patient expectations. Moreover, the knowledge of risk factors for retear after rRCR is also important to refine the patient selection criteria and optimize outcomes. According to systematic reviews on the topic, the available original studies focusing on outcomes after arthroscopic rRCR and the risk factors for poor clinical outcomes is mostly limited to several case series. 2,22 Only a few previous studies have compared the clinical and/or radiological outcomes of patients undergoing rRCR with those who had a pRCR. 13,15,36 However, the cohort in the pRCR group in these comparative studies was heterogeneous, consisting of patients who had RCTs of all sizes, and those who had a repair of the subscapularis tendon.
The aims of the current study, conducted in patients with a supraspinatus with or without infraspinatus (posterosuperior cuff) tendon tear, were 2-fold: (1) to compare the pain and function outcomes and healing rates after rRCR for any tear size with those after pRCR for large to massive RCT (mRCT) and (2) to identify the risk factors for poor functional outcomes and retear after rRCR.
Methods
Patient Enrollment
Data collection and all protocols were approved by an institutional review board. We retrospectively reviewed the prospectively collected data of 3184 patients who underwent pRCRs at a tertiary care institution between January 2010 and December 2017 by a single surgeon (J.H.O.). The grading of RCTs as per tear retraction or anteroposterior dimension into small (≤1 cm), medium (>1 to <3 cm), large (≥3 to <5 cm), and massive (≥5 cm) was based on a previous study by DeOrio and Cofield. 9 We included patients with an RCT involving the posterosuperior cuff who had undergone either an rRCR or a pRCR and had an available clinical follow-up of a minimum of 2 years. We excluded patients with a cuff tear involving the subscapularis tendon, 26 calcific tendinitis, and glenohumeral arthritis. Patients who had a pRCR for small and medium RCTs (tear size <3 cm in both retraction and anteroposterior diameter) were also excluded. Those who had undergone >1 previous RCR and those who had conversion from arthroscopic to open/mini-open repair were excluded. Of 3184 patients, after the assessment of patient data according to the inclusion and exclusion criteria, 54 patients (1.7%) with rRCR and 162 (5.1%) with pRCR for mRCT were included in this study. Subsequently, 8 of 54 patients (15%) with rRCR and 56 of 162 (35%) with pRCR were lost to a minimum 2-year clinical follow-up. Ultimately, 46 patients in the rRCR group and 106 patients in the pRCR group were included for analysis (Figure 1).
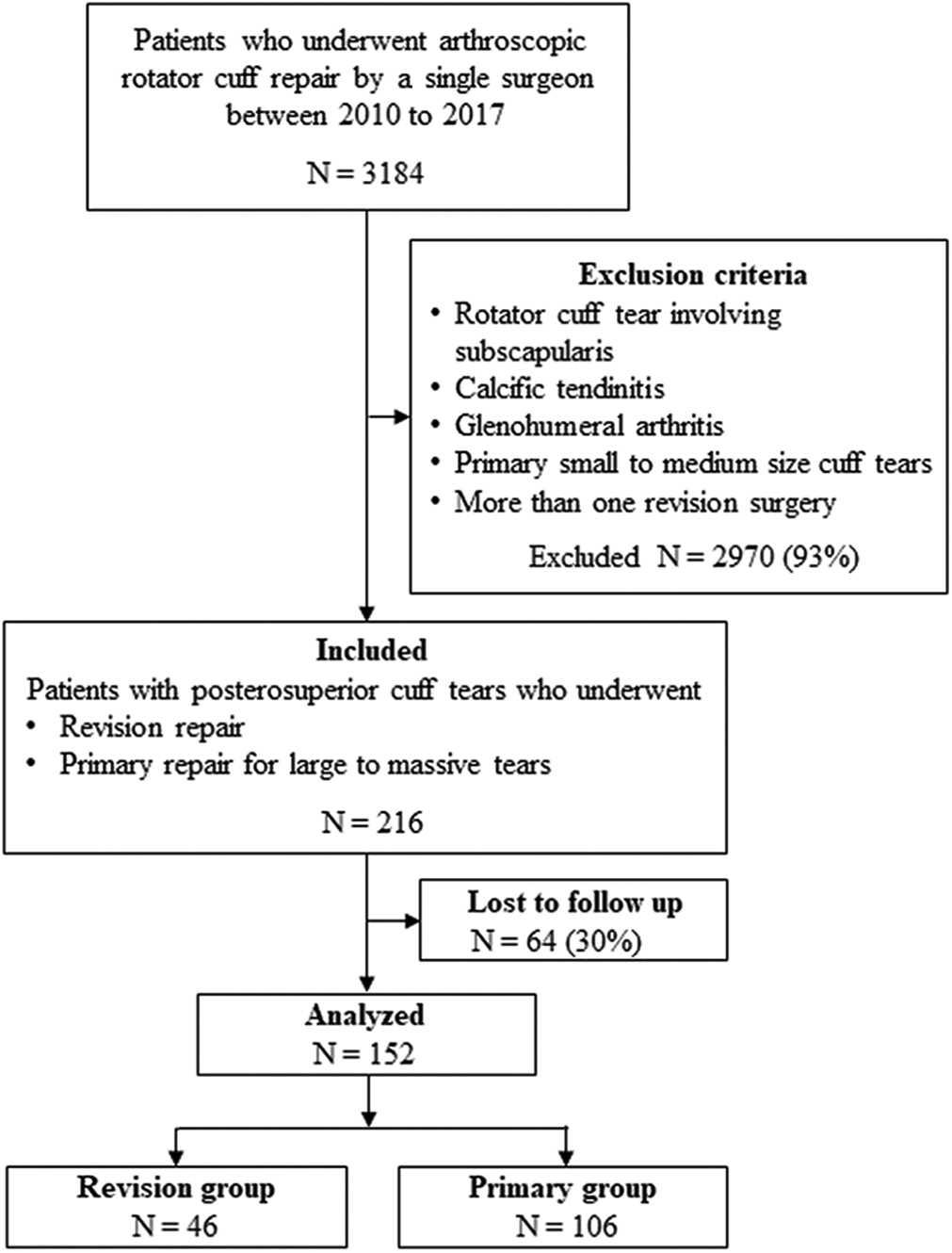
Flowchart showing patient enrollment in the study.
The demographic variables noted were age; sex; body mass index (BMI); dominant side involvement comorbidities such as diabetes mellitus, hyperlipidemia, and osteoporosis; and history of trauma and smoking. All patients undergoing rotator cuff repair at our institution routinely undergo a DEXA scan to determine bone marrow density because a previous study found osteoporosis to be an independent risk factor for retear after cuff repair. 5 The incidence of osteoporosis was based on the T score value from the bone marrow density assessment measurement at the last outpatient visit before surgery using dual-energy X-ray absorptiometry (Lunar Prodigy, enCORE Version 8.8; GE Medical Systems). 5 The lowest T score of the proximal femur and lumbar spine, except for the value for the Ward area of the proximal femur, 1 was recorded, and scores were dichotomized as osteoporosis (T score < 2.5) and no osteoporosis (T score ≥ –2.5) for the purpose of statistical evaluation. Fatty degeneration of the rotator cuff muscles on preoperative magnetic resonance imaging (MRI) scans was assessed using the Fuchs et al 11 modification of the Goutallier et al 14 classification scheme. The Fuchs classification was dichotomized as favorable (Goutallier grades 0, 1, and 2) or unfavorable (grades 3 and 4) for the purpose of statistical evaluation in the current study, as in a previous study. 26 The radiological parameters were evaluated by a musculoskeletal radiologist with 18 years of experience who was blinded to the details of the present study.
Surgical Procedure and Rehabilitation
All procedures were performed arthroscopically by a single senior surgeon (J.H.O.) who has been performing arthroscopic rotator cuff surgeries for >18 years. In the rRCR group, the mean ± SD duration between the index primary RCR and detection of retear was 33 ± 39.4 months (range, 1-180 months). The mean ± SD duration between the index pRCR and rRCR in patients of the rRCR group was 36 ± 40.9 months (range, 4-185 months). In the pRCR group, the mean ± SD duration between onset of symptoms and primary surgery was 23.9 ± 26.1 months (range, 1-120 months).
Patients were placed in the lateral decubitus position under general anesthesia. An arm traction device (Spider limb positioner; Smith & Nephew) was applied to the operative arm of the patient. After the assessment of intra-articular lesions using the posterior portal as the viewing portal, the arthroscope was inserted into the subacromial space. The anterior and lateral portals were used as working portals. Subacromial decompression was performed if there was evidence of subacromial or outlet impingement that included an acromioplasty if the preoperative acromial thickness was >7 mm. 29 Acromial thickness was measured preoperatively at the widest portion of the acromion on the perpendicular plane to the long axis of the acromion on the oblique sagittal-plane MRI scan just lateral to the acromioclavicular joint, as described in a previous study. 29
Inflamed bursal tissues and adhesions were removed and debridement was performed at the edge of the torn cuff. The quality of the torn tendon was noted as poor if it was thin, fragile, or delaminated as per the intraoperative subjective assessment by the senior author (J.H.O.). Previous anchors were removed using an arthroscopic grasper device, if possible. The size of the tear was measured using a calibrated arthroscopic probe. The torn rotator cuff tendons were repaired in the subacromial space using a 70° arthroscope. The bleeding surface of the tuberosities was prepared to enhance the tendon-to-bone healing. The choice of suture configuration was dependent on the tear retraction; a modified Mason-Allen suture technique was used for small RCTs (≤1 cm), and a double-row suture bridge technique was used for medium to large RCTs (>1 to <3 cm). A single-row repair was performed in patients who had mRCTs (≥3 cm) in whom the torn tendon mobilization was limited to the medial part of the footprint. If the torn end of the rotator cuff tendon could not be attached to the footprint, intra- and extra-articular muscle releases were performed to allow for greater mobilization of the tendon. In cases where the torn tendon could not be attached to the footprint even with sufficient medial muscle release, footprint medialization up to 1 cm was performed by denuding the cartilage from the corresponding lateral articular surface of the humerus. Completion of the repair was achieved in all patients in this study. For patients with bicipital groove tenderness and concomitant biceps tear on MRI scans, biceps tenodesis was performed in those who wanted to preserve supination strength; otherwise, a biceps tenotomy was performed. 31
Postoperatively, the operated shoulder was immobilized via an abduction brace for 6 weeks. Shrugging of both shoulders, active elbow flexion-extension, active forearm supination-pronation, and active hand and wrist motion were encouraged immediately after the surgery. Early passive range of motion (ROM) exercise was restricted during the brace-wearing period. After weaning from the brace, active and active-assisted shoulder ROM exercises were conducted for the next 6 weeks. At 3 months postoperatively, we evaluated the active ROM of the shoulder and, if comparable with that of the opposite arm, we educated the patients on muscle-strengthening exercises using the TheraBand (Performance Health) including forward flexion, abduction, and external and internal rotation. Athletic activities were usually allowed 6 months postoperatively.
Outcome Assessment
The clinical outcomes noted preoperatively and at final follow-up were patient-reported outcomes (PROs) and active ROM. The PROs included a 10-point visual analog scale (VAS) for pain, the American Shoulder and Elbow Surgeons (ASES) score, 27 and Constant score 7 administered by a trained clinical researcher. Postoperative satisfaction was noted using a 10-point VAS. The active ROM for forward flexion, external rotation with arms at the side, and external rotation with arms at 90° were measured by a trained clinical researcher (S.W.K.) using a goniometer. Internal rotation was noted as the maximum height of the spinous process that could be reached at the back with the tip of the patient’s thumb.
The radiological outcome was assessed using MRI done at 1 year follow up after the surgery. However, for patients who had implanted MRI-incompatible devices including pacemakers or who refused MRI because of its high cost, ultrasonography was utilized instead. An intact cuff was defined as the maintenance of tendon insertion to the footprint, while an unhealed cuff was defined as discontinuity at the footprint. 30 Among patients who had MRI scans available at the 1-year follow-up, retear of the cuff was graded according to the Sugaya classification. 37
Statistical Analysis
Descriptive statistics were performed to summarize the data. Paired-samples t test was used to compare the pre- and postoperative variables within a study group. The difference between the rRCR and pRCR groups was calculated for continuous variables using an independent-samples t test and for categorical variables using a chi-square test. To identify the risk factors for poor ASES scores in the rRCR and pRCR groups, variables that were found significant (P < .05) in univariate linear regression analysis were tested using a multivariate linear regression model to calculate the adjusted regression coefficient (r). Similarly, to identify the risk factors for retear in the rRCR and pRCR groups, variables that were found significant (P < .05) in univariate logistic regression analysis were then tested using a multivariate logistic regression model to calculate an adjusted odds ratio (OR). All statistical analyses were performed with SPSS Version 25 (IBM Corp). A P value < .050 was considered significant.
The difference in outcome scores of comparison groups was considered clinically significant if it was more than previously published minimal clinically important difference (MCID) values. 21,38 Accordingly, the thresholds for MCID were considered as 2.4 for VAS for pain, 27.1 for ASES, and 10.4 for Constant scores.
Results
Patient Demographics in Comparison Groups
There was no difference between the baseline characteristics of the population eligible for the study and the final sample analyzed (excluding patients lost to follow-up) in both groups (Appendix Table A1). The patients in the rRCR group were younger (58.6 ± 7.9 vs 65.4 ± 7.6 years; P < .001) with a higher proportion of male patients (65.2% vs 34.9%; P = .001) than were those in the pRCR group (Table 1). The other baseline characteristics were similar in both groups. Preoperative PROs and ROM were similar in both groups except for less internal rotation at the back in patients in the rRCR group (11.0 ± 3.2 vs 9.2 ± 3.0, wherein vertebral levels were numbered serially [Table 1] indicating the highest level at the back to which the tip of the thumb could reach; P = .001).
Comparison of Preoperative Baseline Variables Between the Revision and Primary RCR Groups a

a Values are reported as n (%) or mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; F, female; M, male; NA, not analyzed; RCR, rotator cuff repair; VAS, visual analog scale.
b Values are reported as n (% male).
c Vertebral levels were numbered serially: 1-12 for the 1st to 12th thoracic vertebra, 13-17 for the 1st to 5th lumbar vertebra, and 18 for any level below the sacral region.
The preoperative tear size in the rRCR group was similar to that in the pRCR group for retraction and anteroposterior dimension. The incidence of unfavorable fatty degeneration in the rRCR group was significantly lower than that in the pRCR group for the supraspinatus (37.0% vs 56.6%; P = .026) and infraspinatus (8.7% vs 22.6%; P = .042) muscles. The incidence of poor tendon tissue quality and osteoporosis was similar in both the groups.
The final follow-up was at a mean of 26.4 months (range, 24-81 months) in the study patients. Both groups had a statistically and clinically significant improvement in PROs and ROM from preoperatively to the final follow-up (Table 2). Patients in the rRCR group had significantly worse VAS for pain (2.1 vs 1.0; P = .004), VAS for satisfaction (6.9 vs 8.6; P <.001), and ASES (79.7 vs 89.8; P = .001) scores than did those in the pRCR group, whereas the Constant score (68.0 vs 67.8; P = .919) was not statistically different between the groups (Table 2). None of the above differences in PROs were clinically significant, as they did not exceed the MCID threshold.
Changes in Outcome Scores and ROM at Final Follow-up Within and Between Groups a

a Data are reported as mean ± SD. Dashes indicate that the MCID was not available in the literature. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; NA, not analyzed; preop, preoperative; RCR, rotator cuff repair; ROM, range of motion; VAS, visual analog scale.
b The difference between preoperative and final follow-up values exceeded the MCID.
c Vertebral levels were numbered serially. See Table 1 footnote.
Retears were evaluated using MRI in 110 patients (72.4%) and ultrasonography in 42 (27.6%). The retear rate in the rRCR group (50.0% vs 38.7%; P = .194) was not statistically different from that in pRCR group. Out of 23 patients with retear in the rRCR group, 15 had MRI scans available at the final follow-up, which showed a retear of Sugaya type IV in 4 patients and type V in 9 patients. While comparing PROs in the rRCR group, patients who had a retear at the 1-year follow-up showed statistically significantly worse VAS for pain and ASES scores than did patients with an intact cuff; but these differences did not exceed the MCID threshold (Table 3). Additionally, the Constant score, VAS for satisfaction score, and ROM were similar in patients in the rRCR group irrespective of the cuff integrity at final follow-up.
Comparison of Final Outcomes in the rRCR Group Between Patients With an Intact Cuff and Retear a
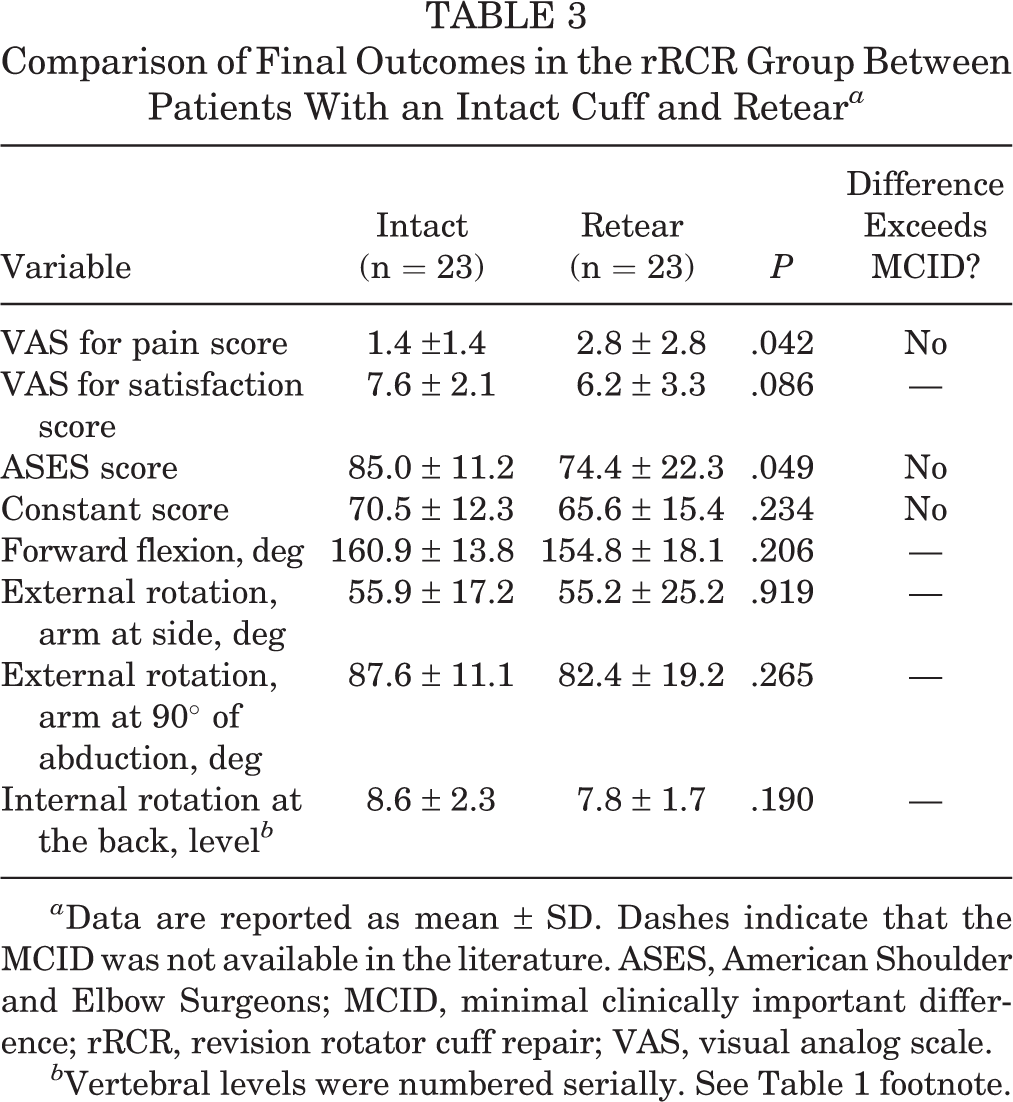
a Data are reported as mean ± SD. Dashes indicate that the MCID was not available in the literature. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; rRCR, revision rotator cuff repair; VAS, visual analog scale.
b Vertebral levels were numbered serially. See Table 1 footnote.
Out of 41 patients with retear in the pRCR group, 29 had MRI scans available at the final follow-up, which showed a retear grade of Sugaya type IV in 9 patients and type V in 20 patients. Patients in the pRCR group who had a retear did not show statistically or clinically significant differences in any PROs and ROM compared with those who had an intact cuff (Table 4).
Comparison of Final Outcomes in the pRCR Group Between Patients With an Intact Cuff and Retear a

a Data are reported as mean ± SD. Dashes indicate that the MCID was not available in the literature. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; pRCR, primary rotator cuff repair; VAS, visual analog scale.
b Vertebral levels were numbered serially. See Table 1 footnote.
Among the various baseline variables studied (see Table 1), the risk factors for worse ASES score in the rRCR group were lower BMI (P = .032; r = 1.9) and lower preoperative VAS for pain score (P = .038; r = 2.3). Similarly, retear (P = .043; r = –11.3) was a risk factor for poor ASES score in the rRCR group. Additionally, the risk factors for retear in the rRCR group were preoperative high-grade fatty degeneration of supraspinatus muscle (Goutallier grades 3 and 4) (P = .026; OR, 5.2) and serum hyperlipidemia (P = .035; OR, 11.8). In the pRCR group, the risk factor for poor ASES score was serum hyperlipidemia (P = .0212; r = 11.5). The risk factor for retear in the pRCR group was a preoperative high-grade fatty degeneration of infraspinatus muscle (Goutallier grades 3 and 4) (P = .174; OR, 2.0). Additionally, with a 1-cm increase in the anteroposterior tear diameter, there was a 20% higher risk of retear in the pRCR group (P = .533; OR, 1.022).
Discussion
The knowledge of clinical outcomes after rRCR could improve the decision making for treatment strategy and setting of reasonable patient expectations. The aim of the current study was to compare the clinical outcomes in patients with posterosuperior cuff tear who underwent rRCR with those in patients who underwent pRCR for mRCTs. The pain relief, function, and ROM at the final follow-up showed no clinically meaningful difference between the rRCR and pRCR groups. The retear rate was also similar after primary and revision surgery. Among patients who had rRCR, the risk factors for poor postoperative function were retear, lower BMI, and lower preoperative pain. On the other hand, the risk factors for retear after rRCR were high-grade fatty degeneration of the supraspinatus muscle and serum hyperlipidemia.
The statistically significant improvements in pre- to postoperative clinical outcomes, pain, and satisfaction in the rRCR group are consistent with those reported in previous studies 15,23,33,39 and systematic reviews. 2,22 To the best of our knowledge, this is the first study to evaluate the improvements in pain and function after rRCR in terms of clinically significant change using MCID thresholds. If one were to apply the MCID values used in the current study to previous reports, few studies have shown clinically significant improvement in pain and function after rRCR. 19,23,39 It is difficult to compare the results of this study with those of previous studies that compared the clinical outcomes of rRCR and pRCR. 13,15,36 This is because the cohort undergoing primary surgery in those studies included RCTs of all sizes and included patients with subscapularis tendon tears. Of note, the clinical outcomes differed according to tear size and involvement of the subscapularis tendon. 26,30,35 Accordingly, we excluded patients with small to medium RCTs from the pRCR group and those with tears involving the subscapularis tendon from both groups to mitigate confounding factors and have a more homogeneous cohort for comparison.
Similar to the results from the current study, previous studies have reported statistically worse pain relief, function, and satisfaction for surgery after rRCR than after pRCR. 13,15,36 However, as recent literature has emphasized, it is critical to use the MCID to judge the effectiveness of the treatment as perceived by the patients instead of just the P value to interpret the results. 8,18,21,25,38 Only 1 study has compared the improvement in postoperative function based on the MCID of the Flexilevel Scale of Shoulder Function (FLEX-SF) score and found it to be clinically significantly worse in the rRCR group than in the pRCR group. 15 In contrast, the patients in our study who had revision and primary surgery experienced similar pain relief and function in terms of clinically meaningful difference at the final follow-up. The reason for this could be that the tear characteristics of the patients were comparable and homogeneous in our study due to the inclusion of only posterosuperior tears in both groups and only large to massive tears in the primary group.
The high retear rate after rRCR in the current study (50%) is similar to that reported in previous original studies, ranging from 40% to 55.5%. 19,36,41 Brochin et al, 2 in a systematic review, analyzed 9 studies for outcomes after arthroscopic rRCR and reported a retear rate of 13.7% (range, 0%-48%). 2 Another important finding of this study was that the retear rate after revision surgery was not different from that after the primary repair done for mRCTs. This is contrary to the previous studies that found a worse success rate after rRCR than after pRCR. 15,36 The reason for this could be that the mean tear size in those studies was smaller in the pRCR group than in the rRCR group, as they did not exclude patients with small and medium RCTs for the pRCR group. Of these 2 studies, 1 had younger patients in the pRCR group than in the rRCR group. 36 In our study, patients included in the pRCR group were confined to those who had mRCTs with a similar tear size to that of the rRCR group. Additionally, patients in the pRCR group were older and had a higher incidence of high-grade fatty degeneration of the supraspinatus and infraspinatus muscles. 5,24 Thus, an older cohort of patients with a higher incidence of high-grade fatty degeneration undergoing pRCR for mRCT in this study had a success rate similar to that of patients who had an rRCR for mRCT.
The results of this study strengthen the evidence that retear is an independent risk factor for poor functional outcomes after arthroscopic rRCR. 19,36 Additionally, the preoperative variables of lower BMI and lower pain scores were found to be associated with poor function after rRCR. While the influence of obesity on functional outcomes after RCR is controversial, 28,40 studies evaluating the influence of lower BMI on the outcomes of pRCR or rRCR are lacking. Among previous studies, the demographic factors that were found to be associated with poor function after rRCR were female sex, 4,23,33 surgery involving the dominant arm, 4 poor preoperative ROM, 4,19,33 and recurrent retear after revision surgery. 19 In the current study, the risk factors for retear after rRCR for posterosuperior tears were preoperative high-grade fatty degeneration of the supraspinatus muscle and serum hyperlipidemia. Such patients could be considered for alternative suitable treatments such as reverse shoulder arthroplasty, superior capsular reconstruction, tendon transfer, or balloon spacer, as retear after rRCR was associated with poor postoperative functional outcomes. The results of the current study concur with those of a previous study that found that tear size, patients’ age, number of anchors used, and tissue quality of the cuff were not factors contributing to a higher retear rate at 6 months and 2 years after arthroscopic rRCR. 36 Another previous study, however, found that older age and multiple tendon tear were associated with retear after rRCR for supraspinatus and/or infraspinatus RCT. 19
The study findings that serum hyperlipidemia is associated with poor function after primary repair of mRCTs is in line with those of previous studies that found its association with cuff retear 12,20 and increased revision rate. 3 Further studies are needed to make recommendations about prescribing statins to optimize serum lipid levels in patients undergoing RCR. The study results further strengthen the evidence that high-grade fatty degeneration of the infraspinatus muscle and larger tear dimensions are risk factors for retear after pRCR. 5,20
The present study has certain limitations that must be considered. First, the study design was retrospective in nature. Second, 30% of the patients eligible for this study were lost to follow-up, which could have led to a sampling bias. However, there was no statistical difference between the baseline characteristics of the eligible population and the patient sample that was analyzed (excluding patients lost to follow-up) in both the rRCR and the pRCR groups (Appendix Table A1). This indicates that, despite the 30% loss to follow-up, the comparison groups analyzed in this study are representative of the patient populations undergoing rRCR and pRCR. Third, the findings of pre- and postoperative quantitative muscle strength were not reported in the current study, which would have allowed for better comparison and correlation of the outcome variables. Fourth, postoperative radiological outcomes in some patients were evaluated using ultrasonography instead of an advanced imaging technique such as MRI. However, ultrasonography has been found to have a similar accuracy for the assessment of shoulder abnormality after surgery. 34
Nonetheless, this study has certain strengths. Unlike previous comparative studies, 15,36 the selection criterion for the pRCR group was stricter with the inclusion of patients who had mRCT and exclusion of those with small to medium tears. The selection bias was mitigated by excluding RCTs involving the subscapularis tendon for both groups, which have different demographic characteristics and outcomes from RCTs involving the posterosuperior cuff. 26 Unlike a previous similar study, 15 all surgeries were performed arthroscopically by a single surgeon (J.H.O.) at 1 institution, minimizing the assessment and treatment bias including operative technique and rehabilitation. Previous similar studies have used single and not so commonly have used tools such as the L’Insalata shoulder questionnaire 36 and Flexilevel Scale of Shoulder Function 15 for the comparison of functional outcomes after pRCR and rRCR. In contrast, we utilized 2 different and commonly used PROs (ASES score and Constant score) to compare the function among the study groups, which probably gives more credibility to our study results and enables direct comparison with other studies in a meta-analysis. Finally, we used MCID along with the statistical significance to compare the results between study groups, which is aligned with the recent emphasis on reporting the clinical significance of the observed difference in clinical outcomes. 8,18,21,25,38
Conclusion
Patients who underwent rRCR had similar clinical and radiological outcomes to those who underwent pRCR for large to massive posterosuperior cuff tears. According to the current data, patients with symptomatic failed RCRs having high-grade fatty degeneration of the supraspinatus muscle and/or serum hyperlipidemia had a greater likelihood of retear after revision repair, which was associated with poor functional outcomes. These patients should be considered for an alternative treatment such as reverse shoulder arthroplasty, superior capsular reconstruction, tendon transfer, or balloon spacer.
Footnotes
Final revision submitted November 3, 2020; accepted December 14, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Bundang Hospital (study No. B-1905/543-106).
Appendix
Baseline Characteristics in the Revision and Primary Groups Between Eligible and Enrolled Patients a

| Revision RCR Group | Primary RCR Group | |||||
|---|---|---|---|---|---|---|
| Eligible Patients (n = 54) | Enrolled Patients (n = 46) b | P | Eligible Patients (n = 162) | Enrolled Patients (n = 106) b | P | |
| Age, y | 59.2 ± 8.2 | 58.6 ± 7.9 | .719 | 63.7 ± 9.3 | 65.4 ± 7.6 | .110 |
| Sex, M:Fc | 33:21 (61.1) | 30:16 (65.2) | .672 | 69:107 (34.0) | 37:69 (34.9) | .872 |
| BMI | 25.1 ± 3.3 | 25.1 ± 3.2 | .970 | 24.9 ± 2.8 | 24.8 ± 2.9 | .798 |
| Dominant side involved | 40 (74.1) | 36 (78.3) | .900 | 142 (87.7) | 92 (86.8) | .836 |
| History of diabetes mellitus | 13 (24.1) | 11 (23.9) | .985 | 31 (19.1) | 18 (17.0) | .655 |
| History of hyperlipidemia | 12 (22.2) | 10 (21.7) | .954 | 35 (21.6) | 21 (19.8) | .724 |
| History of smoking | 8 (14.8) | 8 (17.4) | .726 | 11 (6.8) | 8 (7.5) | .813 |
| History of trauma | 27 (50.0) | 22 (47.8) | .828 | 70 (43.8) | 45 (42.5) | .886 |
| Steroid injections given before surgery | 2.0 ± 3.6 | 2.1 ± 3.7 | .925 | 1.0 ± 1.6 | 1.0 ± 1.7 | .805 |
| Osteoporosis | 12 (22.2) | 11 (23.9) | .841 | 45 (27.8) | 25 (23.6) | .445 |
| VAS pain score | 6.4 ± 2.6 | 6.2 ± 2.5 | .678 | 6.6 ± 1.9 | 6.5 ± 1.9 | .687 |
| ASES score | 44.3 ± 16.9 | 45.4 ± 16.1 | .740 | 48.9 ± 15.8 | 48.7 ± 15.8 | .922 |
| Constant score | 51.9 ± 15.0 | 52.9 ± 15.3 | .754 | 47.6 ± 17.5 | 47.5 ± 16.8 | .974 |
| Forward flexion, deg | 144.3 ± 31.8 | 142.8 ± 32.2 | .824 | 145.1 ± 31.2 | 143.8 ± 32.4 | .739 |
| External rotation, arm at side, deg | 45.3 ± 19.3 | 44.7 ± 18.8 | .875 | 44.8 ± 22.1 | 44.9 ± 22.3 | .979 |
| External rotation, arm at 90° of abduction, deg | 71.6 ± 19.8 | 71.9 ± 19.3 | .945 | 75.0 ± 19.3 | 72.6 ± 20.4 | .335 |
| Internal rotation at back, level d | 10.9 ± 3.4 | 11.0 ± 3.2 | .860 | 8.9 ± 2.9 | 9.2 ± 3.0 | .522 |
| Tear retraction, mm | 29.6 ± 9.9 | 30.5 ± 10.2 | .632 | 32.6 ± 6.6 | 32.4 ± 6.2 | .803 |
| Tear anteroposterior dimension, mm | 26.7 ± 11.1 | 27.4 ± 11.5 | .735 | 27.2 ± 8.3 | 27.3 ± 7.9 | .996 |
| Poor tendon quality | 39 (72.2) | 34 (73.9) | .849 | 112 (69.1) | 84 (79.2) | .188 |
| Acromial thickness >7 mm and acromioplasty performed | 33 (61.1) | 30 (65.2) | .672 | 144 (88.9) | 101 (95.3) | .068 |
| Unfavorable fatty degeneration (Goutallier grades 3 and 4) | ||||||
| Supraspinatus | 19 (35.2) | 17 (37) | .854 | 99 (61.1) | 60 (56.6) | .463 |
| Infraspinatus | 4 (7.4) | 4 (8.7) | .813 | 37 (22.8) | 24 (22.6) | .970 |
| Subscapularis | 3 (5.6) | 3 (6.5) | .839 | 5 (3.1) | 3 (2.8) | .904 |
| Teres minor | 0 | 0 | NA | 0 | 0 | NA |
| No. of anchors used | 3.9 ± 1.4 | 4.0 ± 1.5 | .959 | 4.0 ± 1.2 | 3.9 ± 1.2 | .529 |
a Values are reported as n (%) or mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; F, female; M, male; NA, not analyzed; RCR, rotator cuff repair; VAS, visual analog scale.
b Excluding patients who were lost to follow-up.
c Values are reported as n (% male).
d Vertebral levels were numbered serially as follows: 1-12 for the 1st to 12th thoracic vertebra, 13-17 for the 1st to 5th lumbar vertebra, and 18 for any level below the sacral region.