
Abstract
Background:
A labral retear is an important contributing factor to surgical failure after arthroscopic soft tissue stabilization for recurrent anterior shoulder instability. However, surgeons frequently encounter poor tissue conditions in the anterior capsule, such as capsular tears, during revision surgery.
Purpose:
To analyze the clinical outcomes and failure rates of revision arthroscopic stabilization after failed Bankart repair based on the tissue conditions of the anterior capsule and the labrum. Outcomes were compared for revision after failed Bankart repair because of a labral retear versus a healed labrum but with capsular tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 55 patients who underwent revision arthroscopic stabilization after failed Bankart repair were included. Revision surgery was indicated if patients had a history of recurrent instability with positive apprehension test results, regardless of magnetic resonance imaging (MRI) findings of a labral retear. Patients were allocated into 2 groups based on arthroscopic findings at the time of revision surgery: group 1 consisted of patients who had a healed labrum with definite anterior capsular tears, and group 2 comprised patients who had labral retears without capsular tears. Clinical outcomes were assessed using the American Shoulder and Elbow Surgeons score, Rowe score, and surgical failure rate.
Results:
Overall, 10 patients were included in group 1, and 45 patients were included in group 2. No capsular tears were detected on preoperative MRI or magnetic resonance arthrography scans in either group, whereas all patients in group 2 had evidence of anterior labral retears on imaging scans. After revision surgery, 9 patients (16.4%) showed surgical failure by 25.6 months postoperatively. Patients in group 1 had a significantly higher surgical failure rate than did those in group 2 (4 patients [40.0%] vs 5 patients [11.1%], respectively; P = .04). The incidence of capsular tears was significantly higher in patients with surgical failure versus those without surgical failure (44.4% vs 13.0%, respectively; P = .04).
Conclusion:
A capsular tear of the anterior capsulolabral complex was an important indicator for surgical failure after revision arthroscopic stabilization. If patients demonstrate symptomatic instability after arthroscopic soft tissue stabilization without evidence of labral retears on imaging scans, an anterior capsular tear should be considered as a possible factor for recurrence.
Approximately 5% to 10% of patients who have undergone arthroscopic soft tissue stabilization procedures have had postoperative recurrent instability and have required revision surgery, despite various stabilization techniques, for recurrent anterior shoulder instability. 2,15,20 Younger age at the time of surgery and glenoid or humeral bone defects are well-known preoperative factors that increase the risk of recurrence after primary arthroscopic surgery. 14,19,27 In revision surgery, young age and the presence of off-track lesions are risk factors for poor outcomes. 25 However, during revision surgery after failed arthroscopic soft tissue stabilization for recurrent anterior shoulder instability, surgeons frequently encounter poor tissue conditions of the anterior capsule, such as anterior capsular tears and fibrotic changes. It is sometimes difficult to repair the anterior capsulolabral complex when a retear occurs in the capsular portion rather than the bone-to-labrum interface because of the fragility of the capsule.
Despite its importance, the poor tissue condition of the anterior capsule has not been included as a risk factor for postoperative recurrence in previous studies. Ligamentous laxity or anterior labroligamentous periosteal sleeve avulsion lesions have been reported as soft tissue factors for postoperative recurrence, which are different from anterior capsular tears or fibrotic changes in terms of the pathogenesis and tear location. 11,22 An anterior capsular tear can occur after a traumatic anterior shoulder dislocation, and the anterior capsule loses elasticity after repetitive capsular tears. 4,5 This damage and recurrent dislocation events eventually lead to plastic deformation with scarring and fibrotic changes of the anterior capsule. In contrast, ligamentous laxity affects shoulder instability by increasing the capsule’s elasticity, and an anterior labroligamentous periosteal sleeve avulsion lesion is an injury of the bone-to-labrum interface, although these 2 abnormalities are also related to poor tissue conditions.
The purpose of this study was to analyze the clinical outcomes and failure rates of revision arthroscopic soft tissue stabilization performed after failed Bankart repair based on the tissue conditions of the anterior capsule and the labrum. Clinical outcomes were compared between patients who had a failed Bankart repair because of a labral retear and those who had a healed labrum but capsular tears. We hypothesized that patients with a healed labrum combined with capsular tears would show poorer clinical outcomes and higher failure rates than would those with labral retears.
Methods
Patient Selection
Institutional review board approval was received for the study protocol, and informed consent was obtained from all participants. Between April 2010 and August 2017, a total of 65 patients who underwent a revision arthroscopic soft tissue stabilization procedure after failed Bankart repair at 2 institutions were evaluated retrospectively. The indications for revision surgery were a history of postoperative recurrent dislocations or subluxations, symptomatic instability with positive signs on apprehension tests, and glenoid bone defects <25%. These indications were applied regardless of magnetic resonance imaging (MRI) findings of a labral retear. Patients with glenoid bone defects >25% were treated using the Latarjet procedure as revision surgery. Patients were included in this study if they underwent revision arthroscopic soft tissue stabilization and had been followed for at least 2 years after revision surgery. The exclusion criteria were as follows: a glenoid bone defect >25% on the en face view of 3-dimensional computed tomography (3D-CT), a history of open Bankart repair, combined rotator cuff tears that required repair, combined biceps tendon–related abnormalities, combined shoulder fractures or brachial plexus injuries, a history of surgical site infections after primary surgery, or age >35 years (to eliminate the possible effects of degenerative labral and capsular changes on clinical outcomes). Patients were also excluded if they only had a single postoperative subluxation event after primary surgery. These patients were treated nonoperatively without revision surgery.
The patients were allocated into 2 groups based on the arthroscopic findings at the time of revision surgery. Patients with a healed labrum and definite anterior capsular tears were included in group 1, while those with labral retears were included in group 2. An anterior capsular tear was defined as a definite gap between the healed labrum and the capsule with exposure of the subscapularis muscle. When the gap was filled with scarring or fibrotic changes of the anterior capsule, the patient was also allocated into group 1.
Clinical Evaluation
All patients completed questionnaires about preoperative descriptive data including age at the time of the first dislocation, surgery type, sex, and number of dislocations. The clinical outcomes were assessed using the Rowe score and the American Shoulder and Elbow Surgeons (ASES) score preoperatively and postoperatively at 3, 6, and 12 months and at the last visit. Return to previous sports activity level was assessed using the following 4 grades at the last visit: grade 1, no limitation in previous sports activity; grade 2, mild limitation in previous sports activity; grade 3, moderate limitation in previous sports activity; and grade 4, severe limitation in previous sports activity. 7,12 Surgical failure was defined as a postoperative dislocation or recurrent subluxation event that required revision surgery because of symptomatic instability.
Radiologic Assessment
All patients underwent MRI or magnetic resonance arthrography before revision surgery to evaluate the status of the labrum and capsule. To determine the presence of off-track Hill-Sachs lesions, the widths of the glenoid track and the Hill-Sachs lesion were measured on preoperative MRI or magnetic resonance arthrography scans. 10,24 The width of the glenoid track was calculated as 83% of the normalized glenoid width minus the glenoid bone defect width. 18 The width of the Hill-Sachs lesion was calculated as the distance from the articular insertion of the rotator cuff tendon to the medial margin of the Hill-Sachs lesion on axial T2-weighted imaging scans. The patient was considered to have an off-track lesion when the width of the Hill-Sachs lesion was greater than was the width of the glenoid track. All patients also underwent plain radiography and 3D-CT to assess the degree of the glenoid bone defect. Glenoid defect size was calculated as a percentage of the normalized glenoid width on the en face 3D-CT view using a previously described method. 26 Ultimately, 2 shoulder fellowship-trained orthopaedic surgeons who were not involved in this study independently assessed clinical outcomes and radiologic measurements.
Surgical Procedure
There were 2 experienced orthopaedic surgeons with 15 and 23 years of experience, respectively, (S.-J.S. and J.-Y.P.) who performed all revision arthroscopic soft tissue stabilization procedures at 2 institutions. All patients underwent the same surgical procedures and followed the same postoperative rehabilitation protocols. Under general anesthesia, patients were placed in the lateral decubitus position with the arm in 40° of abduction and slight forward flexion using a lateral traction device. A standard posterior portal was used for initial visualization. An anteroinferior portal was created in the rotator interval close to the upper margin of the subscapularis tendon for suture anchor insertion. An anterosuperior viewing portal was made through the musculotendinous junction of the rotator cuff posterior to the biceps tendon. Diagnostic arthroscopic surgery was performed through the posterior portal to assess all associated intra-articular lesions. After moving the arthroscope to the anterosuperior portal, the status of the anterior capsulolabral complex was carefully examined.
In patients with anterior capsular tears, the healed anterior labrum was dissected from the anterior edge of the glenoid and mobilized for proper tension on the anterior capsulolabral complex. Subsequently, the labrum and the torn capsule were reattached together to the glenoid using at least 4 all-suture anchors (1.3-mm Y-Knot; ConMed Linvatec). Simultaneously, a grasper was used to pull the capsulolabral complex upward to maintain tension in the anterior labrum and the capsule. In patients with definite anterior labral retears, the anterior capsulolabral complex was dissected thoroughly and mobilized from the anteroinferior glenoid neck using an arthroscopic radiofrequency probe. The anterior capsulolabral complex was repaired or reinforced using at least 4 all-suture anchors (1.3-mm Y-Knot). An additional remplissage procedure was performed in patients of both groups with engaging Hill-Sachs lesions. During the remplissage procedure, 1 or 2 suture anchors were placed in the middle of the Hill-Sachs lesion. The sutures were passed over the infraspinatus tendon and the capsule in a mattress configuration and tied over the infraspinatus tendon in the subacromial space.
Postoperatively, the shoulder remained immobilized with an abduction brace for 4 weeks. After this, the patients were allowed to progressively perform passive range of motion exercises, followed by active range of motion exercises. The patients began shoulder muscle strengthening exercises between 8 and 12 weeks postoperatively and were allowed to return to sports activities at 6 months postoperatively.
Statistical Analysis
The paired t test and Wilcoxon signed rank test were used to compare differences between the preoperative and final follow-up Rowe and ASES scores. The Mann-Whitney U test and Fisher exact test were used to identify significant differences in the clinical scores or failure rates between the 2 groups. P values <.05 were considered statistically significant. All statistical analyses and tests were conducted using SPSS software (Version 21.0; IBM Corp).
Results
Overall, 8 of the 65 patients were excluded for the following reasons: 3 patients were >35 years of age, 2 patients had undergone primary open Bankart repair, 1 patient had a concomitant rotator cuff tear requiring repair, 1 patient had a concomitant shoulder fracture, and 1 patient had a postoperative surgical site infection after primary surgery. A total of 57 patients met the inclusion criteria; however, 2 patients were lost to follow-up. Ultimately, 55 patients, 10 in group 1 and 45 in group 2, were enrolled in this study. No patient in this study had both a labral tear and a capsular tear. The mean follow-up period was 29.3 ± 13.1 months in group 1 and 26.6 ± 4.3 months in group 2. The descriptive data of the 2 groups are summarized in Table 1.
Descriptive Data a
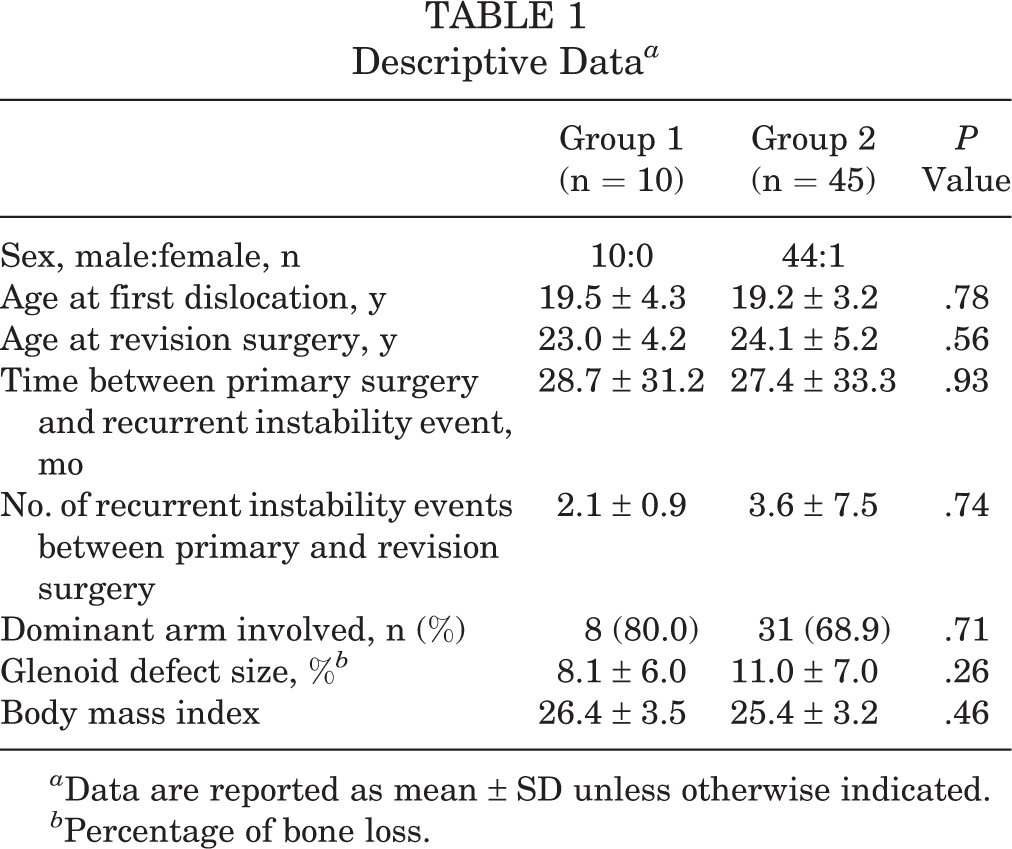
a Data are reported as mean ± SD unless otherwise indicated.
b Percentage of bone loss.
Before revision surgery, 43 patients underwent magnetic resonance arthrography (6 in group 1 and 37 in group 2), and 12 patients underwent MRI (4 in group 1 and 8 in group 2), to detect labral retears. In group 1, none of the patients had labral retears on imaging scans, suggesting a gap between the glenoid and labrum interface. In group 2, all patients had evidence of an anterior labral retear on imaging scans. An anterior capsular tear was not identified on preoperative MRI or magnetic resonance arthrography scans in either group.
Revision surgery was performed at a mean of 40.0 ± 35.1 months (28.3 ± 28.8 months in group 1 and 42.6 ± 36.1 months in group 2; P = .21) after primary surgery. During revision surgery in group 1, there were 7 patients who showed anterior capsular tears, and the other 3 patients showed anterior capsular tears with scar formation at the gap on arthroscopic surgery. All patients in group 1 showed a healed labrum at the bone-to-labrum interface (Figure 1A and B). In group 2, all patients had a labral retear at the bone-to-labrum interface without any capsular tears (Figure 1C and D). There were no differences between the groups in the incidence of other combined intra-articular abnormalities, such as superior labrum anterior to posterior lesions, off-track Hill-Sachs lesions, or posterior labral tears (Table 2). The mean number of suture anchors used was 4.6 ± 0.7 in group 1 and 4.3 ± 0.8 in group 2 (P = .14). An additional remplissage procedure was performed in 8 patients in group 2, who had an off-track Hill-Sachs lesion. There were no other complications, such as surgical-site infections, except for recurrent instability.

All arthroscopic images are in the anterosuperior portal view. (A) A 28-year-old man with a postoperative recurrent dislocation of the left shoulder. The anterior capsule was torn, the subscapularis muscle was exposed (arrow), and the repaired labrum was maintained. (B) The labrum and the torn capsule were reattached together to the glenoid using suture anchors. (C) A 24-year-old man with a postoperative recurrent dislocation of the right shoulder. The repaired labrum was retorn without any anterior capsular tear. (D) The anterior capsulolabral complex regained appropriate tension after mobilization and repair using suture anchors.
Combined Intra-articular Abnormalities During Revision Surgery a

a Data are reported as n (%). SLAP, superior labrum anterior to posterior.
Clinical outcomes improved after revision surgery in both groups 1 and 2 (ASES score: P = .01 and P < .001, respectively; Rowe score: P = .01 and P < .001, respectively). No significant differences between the groups were found with regard to shoulder functional score at the final visit (Table 3). Furthermore, 9 patients (16.4%), in whom postoperative dislocations were noted to occur a mean of 1.9 ± 0.6 times after revision surgery, were classified as having surgical failure. These patients were treated via re-revision surgery at 25.6 months postoperatively. Among the 9 patients with surgical failure, 5 were treated with re-revision arthroscopic soft tissue stabilization (1 in group 1 and 4 in group 2), and the other 4 patients (3 in group 1 and 1 in group 2) underwent an open Latarjet procedure. In addition, 2 patients in group 2 encountered a single subluxation event, and they were treated using shoulder muscle strengthening exercises and did not require re-revision surgery. Group 1 had a significantly higher surgical failure rate (4 patients; 40.0%) than did group 2 (5 patients; 11.1%) (P = .04). In all patients, the incidence of anterior capsular tears was significantly different according to the occurrence of surgical failure (44.4% in patients with surgical failure and 13.0% in patients without surgical failure; P = .04). However, the glenoid defect size or incidence of off-track Hill-Sachs lesions was not associated with the occurrence of surgical failure (glenoid defect size: 8.3% ± 5.8% in patients with surgical failure and 10.9% ± 7.1% in patients without surgical failure [P = .40]; incidence of off-track Hill-Sachs lesions: 11.1% in patients with surgical failure and 15.2% in patients without surgical failure [P = .99]) (Table 4).
Clinical Outcomes and Surgical Failure Rates a

a Data are reported as mean ± SD unless otherwise indicated. Bolded P value indicates a statistically significant between-group difference (P < .05). ASES, American Shoulder and Elbow Surgeons.
Characteristics Between Patients With and Without Surgical Failure After Revision Surgery a
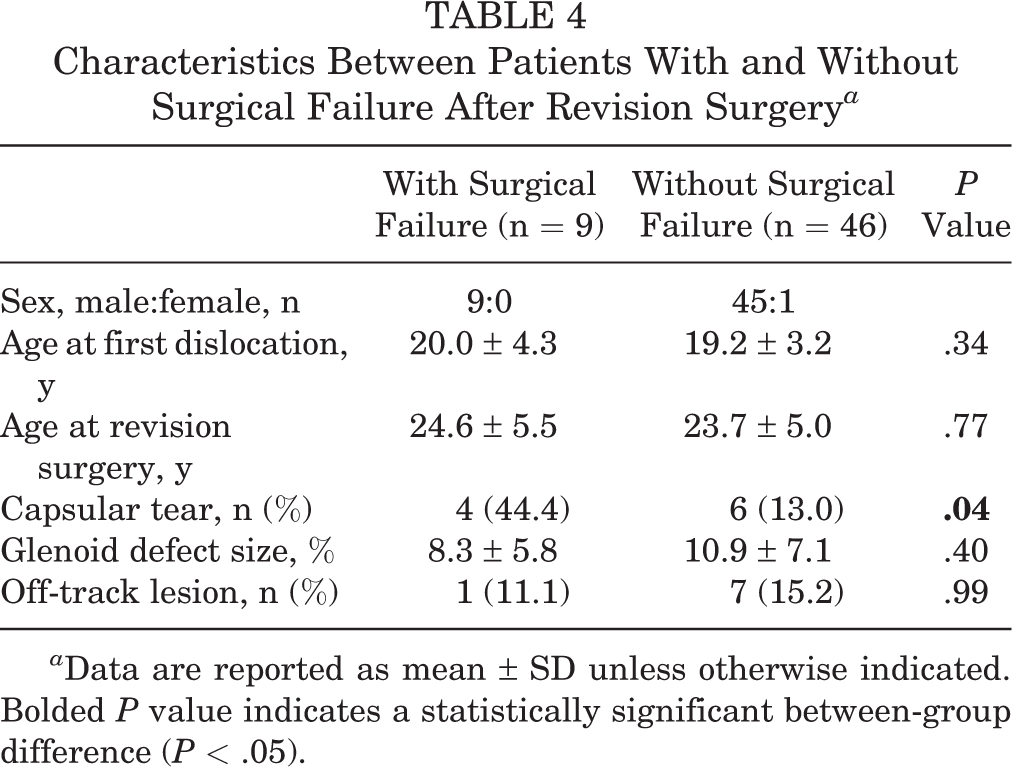
a Data are reported as mean ± SD unless otherwise indicated. Bolded P value indicates a statistically significant between-group difference (P < .05).
There were 22 patients (40.0%) who had high levels of preoperative sports activity, including professional sports and military service (6 in group 1 and 16 in group 2; P = .18). Among them, 4 patients (18.2%) developed a postoperative recurrent dislocation during contact sports play (2 in group 1) or by a traffic accident (2 in group 2). Competent recovery (level 1 or 2) to previous sports activity was achieved in 78.2% of all patients.
Discussion
Revision arthroscopic soft tissue stabilization for patients after failed Bankart repair showed a 16.4% surgical failure rate at 2-year follow-up. Patients with anterior capsular tears seen at the time of revision surgery had significantly higher surgical failure rates than did those who had labral retears without definite capsular tears. The incidence of anterior capsular tears was significantly different between patients with and without surgical failure.
Based on the degree of bipolar bone defect or surgeon preference, various surgical strategies such as revision arthroscopic soft tissue stabilization or the Latarjet procedure could be considered to surgically revise failed Bankart repair. 1,6,17,21,23 According to previous studies, revision arthroscopic soft tissue stabilization seems to have a higher surgical failure rate than does the Latarjet procedure. 1,14,23 However, the surgical failure rate after revision arthroscopic soft tissue stabilization ranges from 12% to 42%. This wide range is because of the use of various surgical techniques and the addition of combined procedures such as the remplissage procedure. 6,14,25 Concomitant remplissage may be very important to lower the recurrence rate, especially in patients with off-track Hill-Sachs lesions. 9,16 Without the remplissage procedure, the surgical failure rate may be as high as 42% after revision arthroscopic soft tissue stabilization. 25 In our study, we performed an additional remplissage procedure in patients with off-track Hill-Sachs lesions. In this setting, the surgical failure rate was lower (11.1%) than that of the previous study, 25 which was performed without the remplissage procedure.
There are many factors that are related to postoperative surgical failure of revision arthroscopic soft tissue stabilization after failed Bankart repair, such as glenoid bone defects, off-track Hill-Sachs lesions, humeral avulsion of the glenohumeral ligament lesions, generalized ligamentous laxity, and contact sports. 1,13,25 However, in the present study, there were no differences in glenoid bone defect size or the incidence of off-track Hill-Sachs lesions between patients with and without surgical failure. These results may be explained by surgical indications such as a glenoid bone defect <25% or additional surgical procedures including the remplissage procedure for patients with off-track Hill-Sachs lesions. If revision arthroscopic soft tissue stabilization is only indicated in patients with a glenoid bone defect <25% and an additional remplissage procedure could be combined in patients with off-track Hill-Sachs lesions, the effects of a bipolar bone defect on surgical failure could be decreased. Under these situations, the soft tissue condition of the anterior capsulolabral complex would have a stronger contributing effect on postoperative surgical failure than would the bipolar bone defect.
During recurrent instability events, the anterior capsulolabral complex could tear at its weakest point, which is either the bone-to-labrum repaired site or the anterior capsule. In patients who have had weak labral healing, a labral retear is very possible with recurrent instability events. However, in patients with firm healing between the bone-to-labrum interface and strong suture strings, a recurrent tear might occur farther from the suture site at the anterior capsule. With multiple instability events, the anterior capsule loses its elasticity. This leads to repetitive capsular tears and fibrotic changes, which complicate a revision stabilization procedure. In this study, 10 patients were found to have poor tissue conditions, represented by anterior capsular tears. Such patients had poor clinical outcomes compared with patients with labral retears without capsular tears. Therefore, to improve postoperative clinical outcomes, it would be better to consider other revision surgical procedures or additional combined procedures such as the Latarjet procedure or open anterior capsular reconstruction in patients who have recurrent instability without MRI evidence of a labral retear. 3,8,23
Despite its important contributing effects on instability, the tissue condition of the anterior capsule has been considered in few studies. In the literature regarding revision arthroscopic soft tissue stabilization by Su et al, 25 the incidence of anterior capsular tears was reported as up to 23% according to the arthroscopic findings, which was similar to the rate in the present study. However, a capsular tear of the anterior capsulolabral complex is difficult to detect preoperatively, despite its frequency. In this study, poor capsular conditions were not detected on preoperative MRI or magnetic resonance arthrography scans in all patients with associated injuries observed via arthroscopic surgery. The decision to perform revision surgery in these patients was made based on clinical symptoms rather than imaging findings. When patients demonstrate symptomatic instability after arthroscopic soft tissue stabilization without evidence of labral retears on imaging scans, an anterior capsular tear should be considered as a possible factor for recurrence. This paradoxical radiologic finding provides clinical clues to predict anterior capsular tears on preoperative imaging scans, which are important factors to decide on an appropriate surgical modality.
This study has several limitations. First, this was a multicenter study in which 2 different surgeons performed all surgical procedures. This arrangement made the study vulnerable to bias. To overcome this multicenter study limitation, we tried to control the surgical indications and to standardize the operative environment and techniques. The second limitation was that magnetic resonance arthrography was not performed in all patients. It was difficult to perform magnetic resonance arthrography in all patients because of its more invasive nature compared with that of MRI. Magnetic resonance arthrography also induces pain with contrast medium injections into the glenohumeral joint. Third, not all patients with failed Bankart repair with glenoid bone defects <25% underwent revision arthroscopic stabilization. Instead, some patients underwent the Latarjet procedure as their revision surgery. Even some patients with a glenoid bone defect <25% underwent the Latarjet procedure because of their own preference. These choices may have influenced our results. Fourth, the sample size of patients with capsular tears was relatively small. Therefore, we may not have had statistical power to detect a significant difference in the clinical outcomes or the incidence of intra-articular abnormalities between patients with capsular tears and labral retears. However, it was difficult to enroll sufficient patients with a capsular tear because of its overall low incidence, especially in situations of shoulder recurrence.
Conclusion
A capsular tear of the anterior capsulolabral complex was an important indicator for surgical failure after revision arthroscopic stabilization. However, it was difficult to detect anterior capsular tears on preoperative MRI or magnetic resonance arthrography scans, whereas a labral retear was easily detected on preoperative imaging scans. If patients demonstrate symptomatic instability after arthroscopic soft tissue stabilization without evidence of labral retears on imaging, an anterior capsular tear should be considered as a possible factor for recurrence.
Footnotes
Final revision submitted November 16, 2020; accepted December 7, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ewha Womans University (No. EUMC 2019-12-027).