
Abstract
Purpose:
To present the clinical results of arthroscopic extended rotator interval release with a stretching program for treating refractory adhesive capsulitis.
Study design:
Case series; level of evidence, 4.
Methods:
Arthroscopy-assisted extended rotator interval tissue release including anterior capsular was performed in 26 patients with refractory adhesive capsulitis. All rotator interval tissues, except the medial sling of the biceps, were excised and the excursion of the subscapularis tendon was restored and freely mobilized. The preoperative mean passive forward flexion was 101°, whereas external rotation at the side was 10°. Patients were followed for a minimum of 2 years and their visual analog scale for pain, muscle power, range of motion, Constant score, modified American Shoulder and Elbow Surgeons Shoulder Evaluation Form score, and modified University of California at Los Angeles score were recorded.
Results:
Visual pain scale and the aforementioned clinical scores improved postoperatively. The patients exhibited a significant postoperative difference in forward flexion, external rotation, and internal rotation. Postoperative mean passive forward flexion was 172°, whereas external rotation at the side was 58°. There was no difference in the muscle power postoperatively including abduction, internal rotation, and external rotation.
Conclusions:
Our study revealed satisfactory subjective and objective clinical results after a 2-year follow-up. Arthroscopy-assisted extended rotator interval release with a stretching program could be an alternative treatment for refractory adhesive capsulitis.
Introduction
Adhesive capsulitis of the shoulder commonly affects approximately 2%–5% of the general population. The pathophysiology of adhesive capsulitis, which is poorly understood, is hypothesized to be a combination of inflammation and capsular fibrosis. Adhesive capsulitis usually resolves in most cases; however, refractory shoulder stiffness exists in cases where conservative treatment failed and in patients who had prolonged pain or residual functional limitation. 1,2
Patients nonresponsive to conservative treatment are considered for a manipulation under anesthesia (MUA) or arthroscopic capsular release. Given the recent advances in arthroscopy, arthroscopic release of the joint capsule is more favorable than other treatment options. 3 –5
However, the extent of release is still controversial. Several authors have recommended 360° release, whereas others have suggested a relatively conservative release. 4 –6 Because the pathology of the rotator interval tissue plays a primary role in adhesive capsulitis, treating rotator interval pathology is justified. Extended anterior capsule release involves resecting all pathological tissues of the rotator interval and restoring the full excursion of the subscapularis tendon. We hypothesize that an arthroscopic treatment with extended anterior capsule release contributes to refractory adhesive capsulitis.
Materials and methods
Patients
From July 2009 to August 2013, 42 consecutive patients with symptomatic adhesive capsulitis refractory to conservative treatment were treated with arthroscopic capsule release. Inclusion criteria were as follows: (1) a painful stiff shoulder for at least 3 months; (2) restriction of passive forward flexion of less than 110° and external rotation less than 45° in 90° of abduction pain; (3) patients had no response to physical therapy program and at least two shots corticosteroid injection. To eliminate bias from severe pain and muscle guarding, 29 patients with passive forward flexion <135° and external rotation <60° in 90° of abduction during general anesthesia were enrolled in this study. Magnetic resonance imaging was performed when intrinsic shoulder pathology was suspected (Figure 1). We excluded patients with full-thickness rotator cuff tears, subscapularis tendon tears, advanced glenohumeral arthritis, revision procedures, and acromioclavicular arthritis requiring distal clavicle resection. Before the operation, patients were apprised of the advantages, disadvantages, and technical difficulties of arthroscopic capsule release were explained to patients, following which all patients agreed to receive the treatment. All operative procedures were performed by the same orthopedic surgeon. After approval from the institutional review board, the obtained data were retrospectively analyzed.
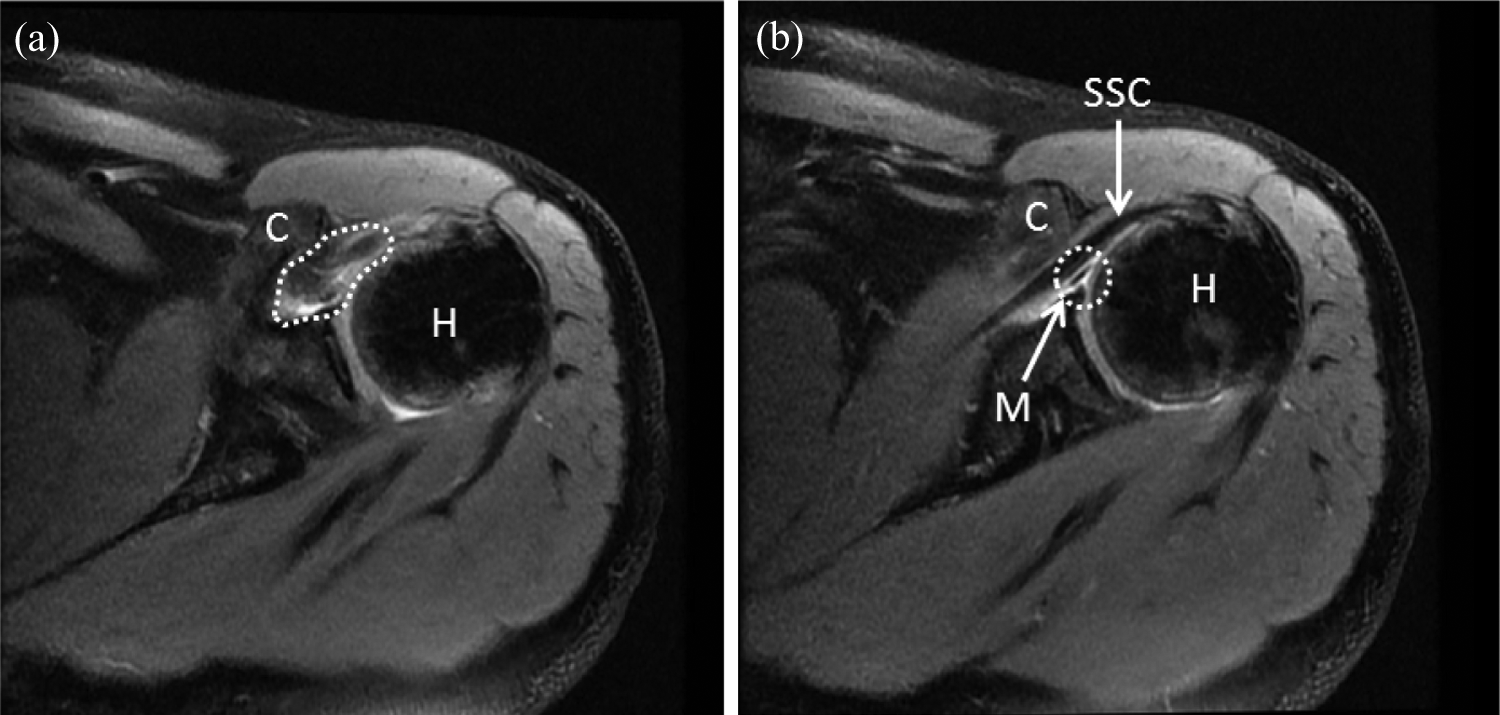
Proton density-weighted magnetic resonance image-based findings of refractory adhesive capsulitis: (a) thickening of anterior capsule (dotted area), (b) subscapularis tendon is bordered anteriorly by the coracoid process and posteriorly by middle glenohumeral ligament, respectively. C: coracoids process; H: humeral head; M: middle glenohumeral ligament (dotted circle); SSC: subscapularis tendon.
Preoperative and postoperative evaluations
Patients were examined at ward or clinic 1 day before operation, during anesthesia, and during follow-up. Outcomes were standardized and assessed by an independent examiner.
Preoperative and postoperative subjective pain was measured with the visual analog scale (VAS). The VAS was used to measure pain of the patients, with 0 indicating no pain and 10 indicating extremely severe pain. Passive shoulder motions including abduction, forward flexion, external rotation at the side and in 90° of abduction, and internal rotation in 90° of abduction were measured with the patient during anesthesia; at 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and 24 months postoperatively; and at the last follow-up. The goniometer was used in the assessment of range of motion (ROM). Quantitative strength measurements of the rotator cuff were obtained and active motion and strength were graded throughout their ROM on a scale from 0 to 5 according to the Medical Research Council. 7 Abduction strength was tested with the patient in the seated position with the arm flexed to 90° in the scapular plane. External rotation strength and internal rotation strength were tested with the shoulder in a neutral position and the elbow in 90° of flexion. The Constant score, 8 modified American Shoulder and Elbow Surgeons shoulder evaluation form, 9 and modified University of California at Los Angeles score were used for clinical assessment. 10
Operative techniques
Patients were placed in the lateral decubitus position and examined under anesthesia. A standard posterior portal was created, and a 30° arthroscope was introduced into the glenohumeral joint. Subsequently, thorough diagnostic arthroscopy was performed. An 18-gauge spinal needle was used for ascertaining the precise location for placing the anterior portal; the portal was created superior to the lateral half of the subscapularis tendon. After establishing the two portals, thorough arthroscopy was performed and the intra-articular pathology was assessed.
Arthroscopic anterior capsule release
All rotator interval tissues between the upper subscapularis and the superior glenohumeral ligament were excised using a shaver and a 90° electrocautery probe (Orthopaedic Procedure Electrosurgical System; Arthrex, Naples, FL, USA). The upper border of the subscapularis tendon was exposed, and this tendon and the medial sling of the biceps (superior glenohumeral and coracohumeral ligaments) were cautiously preserved. The middle glenohumeral ligament (MGHL) was identified; severe erythematous, thickening, and hardening were usually observed (Figure 2). The MGHL was excised by the use of a punch. Then the 30° arthroscope was changed to 70° arthroscope. The coracoid process was identified and the coracohumeral distance was measured by a burr of which diameter was 8 mm. To achieving a goal of coracohumeral distance larger than 8 mm, coracoplasty was performed if narrow coracohumeral space was noted under 70° arthroscope.

(a) Arthroscopic findings of severe inflammation of the rotator interval tissues. (b) After removal of the anterior capsule, the hard, thickened, and erythematous middle glenohumeral ligament covering the subscapularis tendon was noted. The medial sling of the biceps was preserved. C: coracoid; H: humeral head; M: middle glenohumeral ligament; MS: medial sling of biceps; SSC: subscapularis tendon.
The subscapularis was usually covered in hard or inflamed fibrotic tissue, which affected the medial and lateral excursion of subscapularis. This fibrotic tissue was excised until the glistening subscapularis was freely appeared. The release was medially extended under the coracoid arch for ensuring optimal tendon excursion (Figure 3). Finally, an assistant performed the external and internal rotation to obtain a dynamic arthroscopic view to confirm a recovery of the medial and lateral excursion of subscapularis tendon.

Seventy-degree arthroscopic findings after middle glenohumeral ligament excision and coracoplasty: (a) subscapularis tendon covered in hard and thick fibrotic tissue above a probe; (b) after removal of fibrotic tissue covering the subscapularis tendon, the glistening subscapularis tendon was noted; (c) release extended medially under the coracoid arch (dotted black line). The subscapularis tendon was fully released. C: coracoid process after coracoplasty; SSC: subscapularis tendon.
Technique for manipulation of the shoulder
All instruments and cannulas were removed from the shoulder, and the suspension was removed from the arm. While positioning the arm at 90° abduction, the shoulder was manipulated to achieve a goal of 90° of external rotation while the assistant stabilized the scapula. The shoulder was then manipulated to a goal of 180° of forward elevation.
Postoperative rehabilitation
Each patient had a sling with a small pillow in a slight abduction position, which was applied in the operating room immediately after operation. During a predicted healing period for the capsule, the sling was worn full time for 6 weeks, except when showering or eating. All patients mainly performed home rehabilitation exercises. On the first postoperative day, they were instructed to perform passive stretch programs including forward elevation by table sliding and external rotation with a cane out to 45°. From the first postoperative day to the first 6 weeks, this gentle passive stretch program was performed 15 min every day. At 6 weeks from the date of surgery, the patient was instructed to discontinue the use of the sling. The patient then began aggressive stretches with forward elevation by door sliding and external rotation using a door. From 6 to 12 weeks, this aggressive stretch program was performed 10–15 min every day. At 8 weeks, the patient also started a strengthening program with push-up exercises against a wall. The progression to light weights was based on the patient’s progress. The return to full, unrestricted activities was usually 3–6 months postoperatively and was based on the patient and the patient’s rehabilitation progress.
Statistical analysis
The Wilcoxon signed rank test was used to compare preoperative and postoperative results. The level of statistical significance was set as p < 0.05.
Results
Twenty-six patients with complete follow-up documentation for a minimum of 2 years were included in the outcome analyses. Three patients could not complete regular follow-up evaluations due to two moved to another cities, and one could not be contacted. Patient demographics are listed in Table 1.
Patient demographics.

MGHL: middle glenohumeral ligament.
Arthroscopic and preoperative evaluations
The mean follow-up period was 28.2 months (range, 24–52 months). The mean duration of symptoms before surgery was 7.5 months (range, 3–18 months). Table 2 lists the preoperative evaluations.
Preoperative and postoperative (at last follow-up) measurements.

ROM: range of motion; FF: forward elevation; ERs: external rotation; ERab: external rotation at 90° abduction; IRab: internal rotation at 90° abduction; Abd: abduction; IR: internal rotation; VAS: visual analog scale; ASES: American Shoulder and Elbow Surgeons; UCLA: University of California at Los Angeles.
Pain
At the last follow-up, the mean VAS score was 1.7. Patients showed significant improvement from preoperative levels (Table 2).
Range of motion
As shown in Table 2, at the last follow-up, passive forward flexion was 172° (155–180). External rotation at the side was 58° (44–73), and external rotation in 90° of abduction was 91° (82–105). Internal rotation in 90° of abduction was 29° (15–38), whereas abduction was 168° (160–180).
Muscle strength
The mean muscle strength of patients during abduction, external rotation, and internal rotation was measured at 4.6, 4.6, and 4.8 (grades 0–5), respectively, at the last follow-up. Patients reported no statistically significant decrease in muscle strength (Table 2).
Clinical assessment
The Constant score at the last follow-up was 91 (80–97) points. The modified American Shoulder and Elbow Surgeons score was 90 (79–98) points. The Shoulder Rating Scale of the University of California at Los Angeles score was 34 (28–39) points. Patients reported statistically significant improvement in clinical assessment postoperatively (Table 2).
Recovery patterns of ROM in shoulders
Forward flexion
Patients presented gradual recovery that of 155.1° at 2 weeks postoperatively, 158.2° at 6 weeks, 160.5° at 3 months, 164.8° at 6 months, and 170.2° at 2 years (Figure 4).

Recovery pattern in forward elevation and external rotation during follow-up.
External rotation at 90° of abduction
Patients presented gradual recovery that of 86.5° at 2 weeks postoperatively, 87.2° at 6 weeks, 90.1° at 3 months, 90.0° at 6 months, and 92.1° at 2 years (Figure 4).
Internal rotation at 90° of abduction
Patients presented gradual recovery that of 25.3° at 2 weeks postoperatively, 27.8° at 6 weeks, 26.5° at 3 months, 30.2° at 6 months, and 30.1° at 2 years.
Preoperatively, patients had severely limited passive ROM in forward flexion, external rotation, and internal rotation. This passive ROM recovered postoperatively (Figure 5).
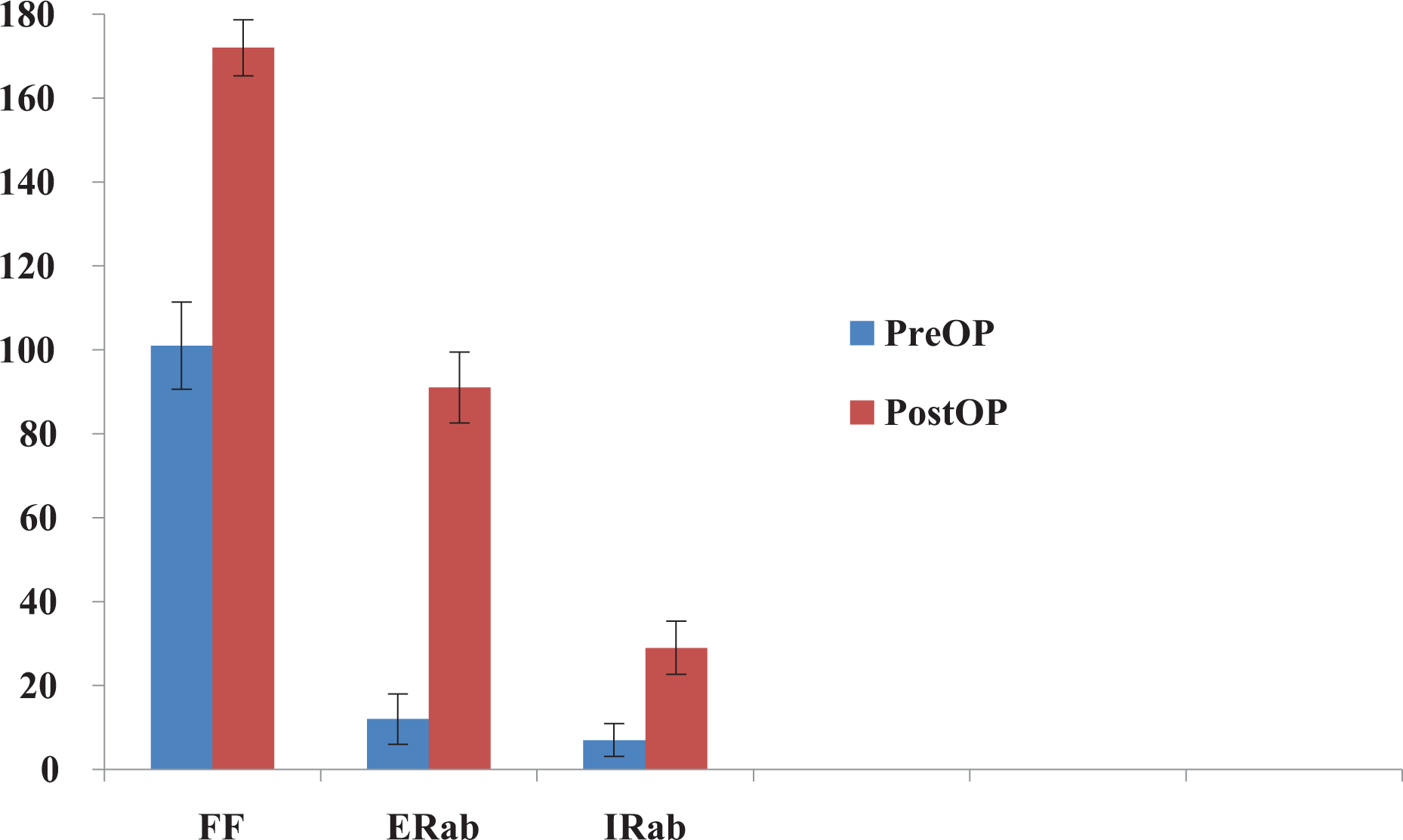
Gain in the range of motion at the last follow-up. FF: forward elevation; ERab: external rotation at 90° of abduction; IRab: internal rotation at 90° of abduction.
ROM for the affected, contralateral, and unaffected shoulders
At last follow-up, the contralateral shoulders had passive ROM (175.3° of forward flexion, 94.2° of external rotation at 90° of abduction, 30.3° of internal rotation at 90° of abduction, and abduction 171.3°) that was almost identical to that in the shoulders after surgery (172.1° of forward flexion, 91.2° of external rotation at 90° of abduction, 29.3° of internal rotation at 90° of abduction, and abduction 168.4°); the difference was not significant.
Complications
No patient requires reoperation or remanipulation. During the first 4-week follow-up, the passive ROM did not improve in three patients, in whom steroid injection at the glenohumeral joint was given. Improvement of shoulder motion was observed after injection. No patient reported symptoms of instability. One patient exhibited superficial wound infection at the site of the surgical incision, which resolved after oral antibiotic administration for 1 week.
Discussion
For treatment of refractory adhesive capsulitis, MUA has been a long-standing treatment, since Neviaser suggested that patients in whom flexion was still limited to less than 90° and those who had not improvement in motion were candidates for closed manipulation. 11 However, the potential complications associated with the manipulation include proximal humerus fractures, glenohumeral dislocation, osteochondral defects, rotator cuff tears, anterior labral detachment, superior labral anterior and posterior tears, and radial nerve injury. 12,13 Moreover, stretching and manipulating mainly improved scapulothoracic motion and not glenohumeral joint motion. 11,14
Numerous recent studies have supported arthroscopic release for effectively treating refractory adhesive capsulitis through the controlled release of the capsular restraints. 4 –6,15 Glenohumeral motion loss assessed in cadaveric cutting studies has clarified that the regional capsule must be released. 16,17 Loss of external rotation mandated the release of the MGHL, rotator interval, coracohumeral ligament extra-articularly, or intra-articular portion of the subscapularis. Loss of elevation merits the release of the anteroinferior capsule, including the anterior band of the inferior glenohumeral ligament. Loss of internal rotation warrants posterosuperior capsular release. However, clinically consensus is lacking on the extent of capsule release; certain authors recommend 360°, whereas others suggest a relatively conservative release. 4 –6
Arthroscopic capsule release entails some complications. Zanotti and Kuhn found an average distance of 7.04, 8.2, and 15.9 mm from the capsular release to the axillary nerve, posterior circumflex artery, and brachial artery, respectively. 18 Harryman et al. reported a case of transient axillary neuropraxia after inferior capsule release. 3 Furthermore, Wong and Williams reported that 1.4% of his series had postoperative axillary neuropathy, of which 95% exhibited sensory deficits lasting an average of 2.3 months. 19 Gobezie et al. reported a case of shoulder dislocation after arthroscopic anterior, posterior, and inferior capsule release, in which the patient was treated with reduction under general anesthesia. 20 Jerosch and Aldawoudy reported a rare but catastrophic complication of glenohumeral joint chondrolysis, which was treated with surface replacement surgery. 21 Moreover, arthroscopic capsule release causes other possible complication, such as hemarthrosis or fluid extravasation. 22
Neer describes the anterosuperior space between the subscapularis and supraspinatus tendon as the rotator interval. Although the definitive role of the rotator interval structures has not been established, they can manifest as adhesive capsulitis. A normal rotator interval contains elastic and membranous tissue, including the biceps long head tendon, superior glenohumeral ligament, MGHL, coracohumeral ligament, and anterior capsule. 23 In adhesive capsulitis, the tissue of rotator interval may become thicken, inflamed, and contracted. The rotator interval tissue has been critically associated with the development of a frozen shoulder. 15,24
Because the pathological condition of the rotator interval tissue plays a primary role in adhesive capsulitis, release of the rotator interval may be justified. Harryman et al. demonstrated an increase in the range of flexion, extension, and external rotation by sectioning the rotator interval capsule. 25 Ozaki et al. demonstrated that open surgical release of only the rotator interval in 17 patients with refractory adhesive capsulitis significantly improved pain; 16 of 17 patients postoperatively regained complete ROM in 3 months. 24 Although open surgery was performed in these studies, no study regarding arthroscopic surgery for only anterior capsule release has been reported.
We hypothesized that only anterior capsule release has additional advantages. First, it prevents axillary nerve injury. To avoid possible axillary nerve injury, certain studies have been extremely cautious regarding inferior capsule release. 3,19 In addition, Warner analyzed the requirement of inferior capsule release, which may affect the axillary nerve, especially when electrocautery or motorized instruments were used. 2 Second, only anterior capsule release reduces the risk of shoulder instability and dislocation compared with extended capsule release. Third, because the bone is the weakest in rotation, the humeral fracture risk is highest during external rotation manipulation. Extended anterior capsule release can restore external rotation without excessively forced manipulation.
Excursion of the subscapularis tendon is crucial in treating adhesive capsulitis. Simeon et al. noted a thick synovium, particularly at the superior border of the subscapularis, which is significantly more common in adhesive capsulitis. 26 Several other previous studies recommended releasing, cutting, or lengthening the intra-articular subscapularis tendon to restore passive external rotation. 24,27 –30 Although controversial, jeopardized subscapularis tendon may introduce postoperative weakness of internal rotation and unbalanced force couple. In this study, enough space for excursion of subscapularis tendon was created instead of lengthening, releasing, or cutting subscapularis itself. The subscapularis tendon was boundary by coracoid anteriorly and MGHL posteriorly. Commonly, coracoplasty was performed if a narrow coracohumeral space was noted; and the MGHL was excised when severe inflammation, thickening, or hardening of the MGHL was noted. The bandlike fibrotic tissue or peritendon, which covers intra-articular component of subscapularis tendon, was also excised until the glistening tendon fibers were visible. To ensure optimal tendon excursion, the release was medially extended under the coracoid arch, and a dynamic arthroscopic view was obtained for confirmation of restoring medial and lateral excursion of the subscapularis. Without reducing internal rotation strength, a satisfactory recovery of external rotation stretch was achieved in this study.
The study has certain limitations; the first being the relatively small sample. However, during the follow-up, there was continued significant relief in the severity and frequency of shoulder pain with activity, at rest, and when trying to sleep without complication. Second, since this was a retrospective study, future prospective randomized comparative studies should be conducted to fully evaluate the clinical results. Third, the role of rotator interval, MGHL, coracoid, and subscapularis tendon were not definite in adhesive capsulitis pathology. Future basic and clinical study should elucidate this point.
In conclusion, arthroscopy-assisted extended anterior capsule release in patients with refractory adhesive capsulitis revealed satisfactory clinical subjective and objective results after a follow-up of 2 years; this release decreases the risk of axillary nerve injury, shoulder instability, fluid extravasations, and hemarthrosis and provides favorable clinical outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.