
Abstract
Background:
Tendon injuries are commonly seen in sports medicine practice. Many elite players involved in high-impact activities develop patellar tendinopathy (PT) symptoms. Of them, a small percentage will develop refractory PT and need to undergo surgery. In some of these patients, surgery does not resolve these symptoms.
Purpose:
To report the clinical results in a cohort of athletes who underwent further surgery after failure of primary surgery for PT.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 22 athletes who had undergone revision surgery for failed surgical management of PT were enrolled in the present study. Symptom severity was assessed through the Victorian Institute of Sport Assessment Scale for Patellar Tendinopathy (VISA-P) upon admission and at the final follow-up. Time to return to training, time to return to competition, and complications were also recorded.
Results:
The mean age of the athletes was 25.4 years, and the mean symptom duration from the index intervention was 15.3 months. At a mean follow-up of 30.0 ± 4.9 months, the VISA-P score improved 27.8 points (P < .0001). The patients returned to training within a mean of 9.2 months. Fifteen patients (68.2%) returned to competition within a mean of 11.6 months. Of these 15 patients, a further 2 had decreased their performance, and 2 more had abandoned sports participation by the final follow-up. The overall rate of complications was 18.2%. One patient (4.5%) had a further revision procedure.
Conclusion:
Revision surgery was feasible and effective in patients in whom PT symptoms persisted after previous surgery for PT, achieving a statistically significant and clinically relevant improvement of the VISA-P score as well as an acceptable rate of return to sport at a follow-up of 30 months.
Tendon injuries are commonly seen in sports medicine practice. 46 Up to 40% of elite players involved in high-impact sporting activities develop symptoms of patellar tendinopathy (PT). 1,31,32,41 PT, or jumper’s knee, is mostly considered an overuse injury and a multifactorial disorder. 37,45 Repetitive mechanical stresses during sporting activities are considered the most important inciting factor. 5,26 Several risk factors have been described: anthropometric, thigh muscle length, quadriceps strength, lower limb kinematics and muscle recruitment, and infrapatellar fat pad size. 18,24,43,44,59 PT considerably limits sports participation and performance and may be career-ending in professional athletes. 52 Blazina et al 13 classified PT into 4 stages according to pain and functional impairment. This classification starts with pain after (stage 1) or during (stage 2) sports activities through to persistent pain (stage 3) and ends with the patellar tendon rupture (stage 4). The management of PT is challenging. Return to sport timing depends strictly on the severity and treatment of PT. Local or systemic administration of anti-inflammatory agents, shock waves, physical therapy, electromagnetic field stimulation, hyaluronic acid, platelet-rich plasma, stem cells, or other growth factors have been proposed as management for chronic PT. 8,9,15,17,51 Conservative management is successful in approximately 90% of patients, especially for Blazina stages 1 and 2. 23,36,39,50 The remaining 10% of patients are candidates for surgery. Several surgical procedures have been proposed, including open, percutaneous, and arthroscopic procedures. 19,35,53 Regardless of the original surgical intervention, approximately 10% of patients have poor outcomes. The treatment of those patients with PT in whom symptoms do not respond to surgery is challenging, with limited options and unpredictable results.
To the best of our knowledge, there is only 1 case report detailing the management of a single patient who continued to report symptoms postsurgically. 47 Recently, the details of the surgical technique we employ after failure of surgery for PT 38 have been published. The present study reports the clinical results in a cohort of athletes after revision for failed previous surgery for PT.
Methods
The present study was performed according to the Strengthening the Reporting of Observational Studies in Epidemiology statement, 60 and all reported procedures received ethics committee approval. Athletes undergoing revision surgery after failed previous surgery for PT were prospectively recruited at the University of Salerno during the period between 2013 and 2017. The inclusion criteria were (1) symptomatic chronic PT, (2) focal or diffuse intratendinous high signals in T1 and T2 at magnetic resonance (Figure 1), (3) previous failed surgical treatments, (4) documented sports participation, and (5) patients able to understand the nature of the treatment and the study. The exclusion criteria were (1) infections, (2) uncontrolled chronic disease, (3) pregnancy or lactation, (4) any blood abnormalities, (5) malignancy, (6) immunodeficiency, and (7) bilateral PT. Ultimately, 22 athletes were enrolled in the study.

Magnetic resonance images suggestive of patellar tendinopathy demonstrating focal or diffuse intratendinous high signals in T1 (right) and T2 (left).
Surgical Technique and Postoperative Rehabilitation
The surgical interventions were performed by a single experienced surgeon (N.M.). An open approach was performed in all cases. All patients were placed in the supine position and underwent general or spinal anesthesia. After exsanguination, a thigh tourniquet was inflated to 300 mm Hg. A midline incision with the knee at 90° of flexion was performed from the proximal pole of the patella and extended distally to the tibial tuberosity. The patellar tendon was then exposed and separated from the Hoffa body by blunt dissection. The paratenon, or the scarred tissue overlying the patellar tendon, was excised by a combination of blunt and sharp dissection. Subsequently, 3 longitudinal tenotomies from the lower patellar pole to the tibial tuberosity were performed (Figure 2). Areas of visually identifiable tendon abnormalities were excised (Figure 2). The subcutaneous fat and skin were closed with absorbable sutures. A wool and crepe bandage was applied and kept in place for 2 weeks. Immediate postoperative mobilization was recommended, and weightbearing with crutches was permitted as tolerated. Five minutes per hour of isometric quadriceps exercises were recommended for each waking hour. The postoperative rehabilitation has been described in our previously published study. 38
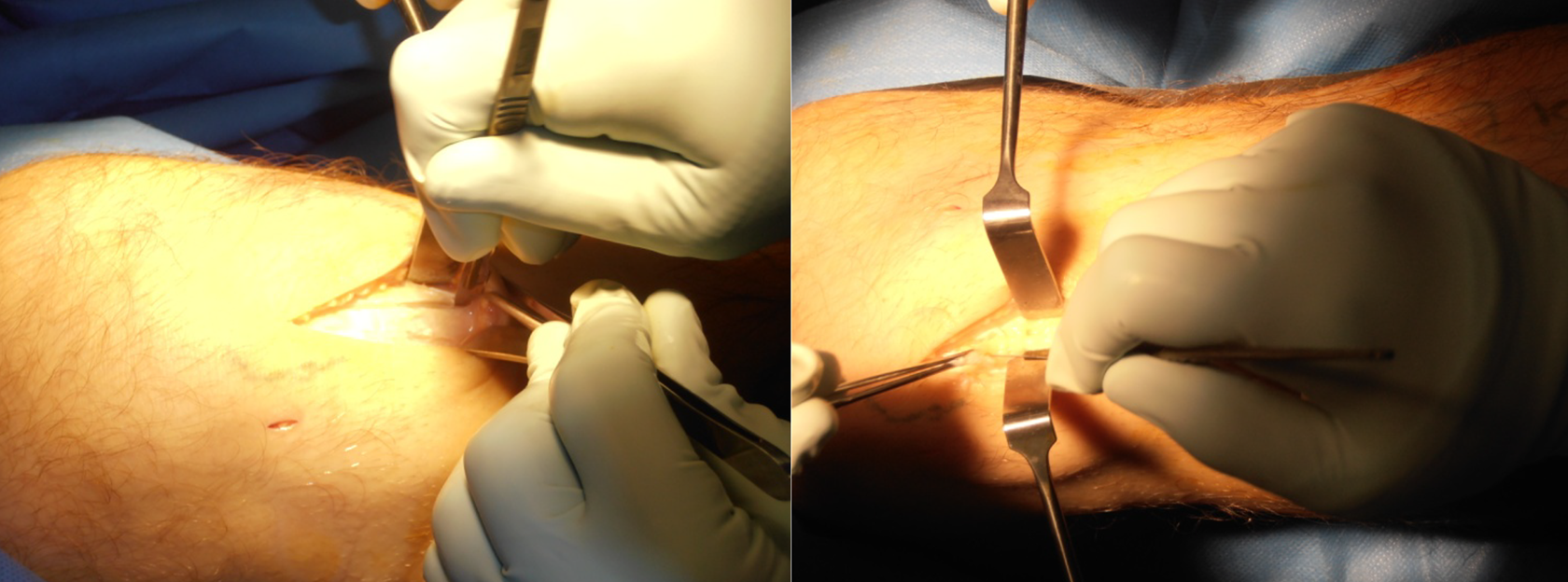
Left: longitudinal tenotomy. Right: excision of the area of tendinopathy.
Outcomes of Interest
On admission, the following data were recorded: mean age, sex, duration of symptoms before revision, number of previous failed surgical treatments, and type of index surgery (open vs arthroscopy). Symptom severity was assessed using the Victorian Institute of Sport Assessment Scale for Patellar Tendinopathy (VISA-P) at admission and the final follow-up. 40 Furthermore, at the final follow-up, data regarding time to return to training, time to return to competition, and complications were recorded.
Statistical Analysis
All statistical analyses were performed by a single author (F.M.), who had not been involved with the clinical management of the patients using the software STATA/MP Version 14.1 (StataCorp). To assess normal distribution of continuous endpoints, the Shapiro-Wilk test (w) was performed. The paired t test was used to assess whether the difference between the VISA-P scores at baseline and the last follow-up was statistically significant (P < .05). A multivariate analysis was performed to investigate whether patients’ baseline characteristics influenced the surgical outcomes. A multiple linear model regression analysis through the Pearson product-moment correlation coefficient (r) was adopted to investigate associations between patients’ baseline at admission (mean age, sex, duration of symptoms before revision, number of previous failed surgical treatments, type of index surgery, and VISA-P score) and their surgical outcome at the final follow-up (VISA-P score, time to return to training, time to return to competition, and complications). The Cauchy-Schwarz formula 10 was used for inequality: +1 is considered as a positive linear correlation, while −1 is a negative one. Values of 0.1 < |r| < 0.3, 0.3 < |r| < 0.5, and |r| > 0.5 were considered to have small, medium, and strong correlations, respectively. The overall significance was performed through the χ2 test, with P < .05 considered statistically significant. A linear regression model was then performed for significant correlations. Added-variable plots were also performed for each comparison.
Results
Patient Characteristics
The 22 study patients participated in the following sports: 5-a-side football (n = 3), netball/squash (n = 2), hurdling (n = 1), volleyball (n = 3), soccer (n = 7), tennis (n = 1), basketball (n = 1), rugby (n = 1), high jump (n = 1), and triathlon (n = 2). Patients had already undergone previous treatment after the original surgical procedure before undergoing the revision procedure: 18.2% (4/22) of patients had 2, 18.2% (4/22) had 3, 36.4% (8/22) had 4, 22.7% (5/22) had 5, and 1 (4.5%) patient had 7 previous treatments. The original operation was performed arthroscopically in 7 patients (31.8%) and in an open fashion in 15 patients (68.2%). The mean age of the patients was 25.4 ± 4.1 years, and 17 patients (77.3%) were men. The mean duration of symptoms from the first surgical procedure was 15.3 ± 3.9 months. According to the Shapiro-Wilk test, the duration of symptoms from the first surgical procedure had a normal distribution (w = 0.9). The VISA-P score at baseline was 53.2 ± 6.6. The patients’ data are shown in Table 1.
Patient Data (N = 22) a

a VISA-P, Victorian Institute of Sport Assessment Scale for Patellar Tendinopathy.
Patient-Reported Outcomes and Return to Sport
At a mean follow-up of 30.0 ± 4.9 months, the mean VISA-P score was 81.0 ± 5.9 (+27.8 points compared with baseline; P < .0001). All patients returned to training within 9.2 ± 1.0 months. Fifteen patients (68.2%) returned to competition within 11.6 ± 1.7 months. Of these patients, at the final follow-up, 2 had decreased their performance, while another 2 had abandoned active sport. The results of the VISA-P at the final follow-up and return to training and competition are shown in Table 2.
Results of VISA-P at the Final Follow-up and Return to Training and Competition a
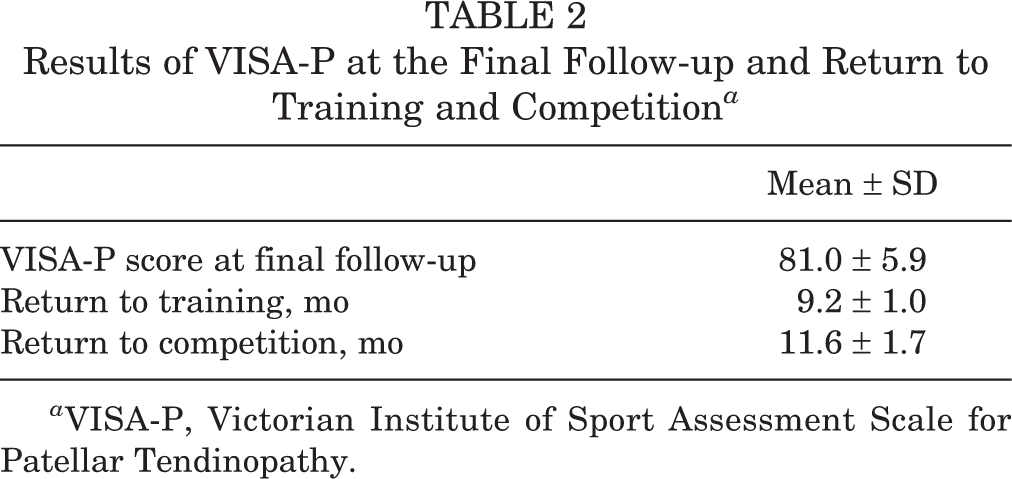
a VISA-P, Victorian Institute of Sport Assessment Scale for Patellar Tendinopathy.
Complications
The overall rate of complications was 18.1% (4/22): 1 patient (4.5%) developed a hematoma, 1 (4.5%) an area of hypoesthesia medial to the surgical scar, and 2 (9.1%) a hypertrophic scar. One patient (4.5%) underwent a further revision.
Multivariate Analysis
The primary procedure could have been performed arthroscopically or in an open fashion; this did not have a statistically significant influence on the final result of the revision surgery on any of the endpoints of the analysis. Male athletes returned to training slightly faster than female athletes (9.0 vs 10.0 months; P = .04), with no further difference between sexes regarding the other surgical outcome. The multivariate analysis evidenced a strong positive correlation between return to training and return to competition (r = 0.65; P = .008). No further correlations were found between patients’ baseline at admission and their surgical outcome at the final follow-up. The added-variable plot of the association between return to training and return to competition is shown in Figure 3.

Added-variable plot of the association between return to training and return to competition.
Discussion
Open surgery with excision of scarred tissue overlying the patellar tendon, separation of the patellar tendon from Hoffa body, multiple longitudinal tenotomies, and excision of macroscopically evident abnormal areas of the tendon from failed surgery for PT result in clinically relevant improvement in symptoms, VISA-P scores, and levels of activities at the 30-month follow-up. The patients in the present cohort returned to training within 9 months of the procedure, while 68.2% returned to competition within a year. Men returned to training approximately 1 month more quickly than women. There was evidence of a statistically significant positive association between quicker return to training and return to competition. There was no evidence of a statistically significant association between the characteristics of patients on admission (age, duration of symptoms before revision, number of previous failed treatments, VISA-P score) and their surgical outcome at the final follow-up (VISA-P score, complications, time to return to training and to sport). Patients had received the primary procedure arthroscopically or in an open fashion, but this did not have a statistically significant difference on the surgical outcome. The overall rates of complication and revision were 18.1% and 4.5%, respectively.
For those patients who do not respond to conservative treatments (approximately 10%), surgery may be required. 6,35,36,39,50 About 10% of patients do not benefit from surgery and are challenging to treat. To the best of our knowledge, only 1 case report reporting data on revision surgery for failed previous surgery for PT was previously published. 47 The patient was a 21-year-old male basketball player with PT refractory to conservative treatments and surgical debridement. Revision was performed through percutaneous, ultrasound-guided tenotomy with a single platelet-rich plasma injection. At 5 months follow-up, the patient had returned to sport with sporadic and slight discomfort after competitions. He was asymptomatic at the 2-year follow-up. However, a single case report does not allow us to draw reliable recommendations.
The rationale of multiple tenotomies is to stimulate the healing process. A deeper knowledge concerning the tendon-healing process is also crucial. Tendon has limited regenerative capability. 42 The tendon healing process is strongly in favor of fibrotic scars. 20,62 This compromises the biomechanical proprieties of the tendon, resulting in reduced elasticity, strength, and efficiency compared with a noninjured tendon. 27,33 Furthermore, after tendon surgery, tissue adherences are common and lead to poorer outcomes. 21,30 These factors enhance the risk of development of chronic degenerative tendinopathies. 4,21,34 Hypovascularity, hypocellularity, and the minimal metabolic activity could be related to the low healing capability of tendons. 12,29 The process of tendon healing has not yet been fully clarified. 16 Animal models of chronic PT are difficult to produce. 54 Furthermore, the processes of tendon healing differ considerably among species. 14,61 Nonhuman primates, such the macaques, are considered the gold standard for research on tendons; however, high costs and ethical restrictions limit their use. 61 Consequently, rats are widely used, even if their tendon healing pathways are different from those of humans. 61
Orthopaedic surgeons must be aware of the prognostic factors for poor postsurgical outcomes for tendinopathy. Greater body mass index and comorbidities are risk factors for poor surgical outcome after tendon surgery. 25,49,63 Postsurgically, women report greater residual symptoms as well as reduced satisfaction and performance. 55 Older patients also exhibit poorer outcomes. 7,22,28,48 Hyperglycemia promotes collagen glycation, reducing healing capabilities. 56 Hypercholesterolemia has also been associated with poorer outcome after rotator cuff and Achilles tendon repair. 2,58 Smokers show thinner and harder tendons, with increased risk of rupture and reduced surgical outcomes compared with nonsmokers. 3,11
The patients in the present study were all secondary and tertiary referrals, with long clinical histories and failures of a variety of conservative treatments before the primary procedure and after symptoms had recurred after the primary surgery. Surgery can be more demanding in patients in whom primary surgery for PT has failed. Recovery time is prolonged, thus considerably reducing recreational activities and quality of life, and may lead to the inability to accomplish rehabilitation. The tendon-healing process can also last a year. 46 Patients must be made aware of this, and even if combined with the best physical therapy care, success cannot be guaranteed. Early attempts to return to sport are a common cause of surgical failure. The rehabilitation protocol will encourage patients to gradually increase their sports and activity level. 57 High-impact sports are not permitted for at least the first 6 months following surgery. Rather, rowing, cycling, swimming, and training on an elliptical or a stepping machine are strongly recommended to maintain or increase the athletes’ level of fitness.
Although no data were systematically collected in this respect, it appears that patients may have had unreasonable expectations after the first surgical procedure. We caution that rehabilitation after surgery for PT is a relatively long process, and the loss of a full sporting season should be expected. Therefore, it is not realistic to plan return to sport after only a few months; even after technically well-performed surgery, 9 months of rehabilitation should be expected, and some patients may take longer.
This study certainly has its limitations. First, the small number of patients included in the present investigation may have affected our ability to identify potentially important variables leading to poor outcomes. Thus, even if methodologically well-conducted, results from multivariate analysis must be carefully interpreted, and further investigations with greater sample size are required. However, it should be considered that these patients are not common; moreover, to our knowledge, no previous studies in this field are available. The patients were all secondary and tertiary referrals to the main author, who has a specialized practice and is fellowship trained in knee and sports surgery. In this respect, therefore, the results are not fully generalizable. The unblinded nature of the study design is a further limitation. As such, we cannot be sure whether all the patients reported all the treatments they underwent before deciding to undergo further surgery. Finally, our case series did not include a control group. A randomized controlled trial comparing 2 or more techniques could be planned to demonstrate which one offers superior outcomes. We have to emphasize, however, the difficulties such a study design would face, given the fact that these patients are not common and that randomization in revision surgery may not be easily accepted by the patients and the surgeons alike. All these limitations affect considerably the reliability of our results; therefore, data must be interpreted with caution. Future studies should consider these limitations and perform high-quality analyses on larger populations.
Conclusion
Multiple longitudinal tenotomies as management for failed surgery for PT are feasible and effective, achieving a considerable improvement of the VISA-P score at the 30-month follow-up. Patients returned to training within 9 months, and 68.2% returned to competition within a year. Men returned to training faster than women. No further differences between sexes were found. Both patients and physicians must be aware that the realistic time to return to sport is long, in the region of a full sporting season.
Footnotes
Final revision submitted October 16, 2020; accepted November 19, 2020
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Salerno.