
Abstract
Background:
Hamstring tendon grafts are usually fixed in anterior cruciate ligament (ACL) reconstruction using either an adjustable-loop device (ALD) or a fixed-loop device (FLD). The contact area between the graft and the tunnel wall is different between the 2 devices.
Purpose:
To determine using magnetic resonance angiography (MRA) whether ALD and FLD result in different blood flow of the graft in the femoral tunnel during the early postoperative period.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between 2008 and 2018, a total of 42 patients (17 men and 25 women) underwent MRA at 3 months after ACL reconstruction. All surgical procedures were performed using semitendinosus tendon autografts folded into 4 strands. Overall, 23 patients underwent the FLD procedure and 19 patients underwent the ALD procedure. The signal intensity of the superior portion of the graft in the femoral tunnel was evaluated using transverse MRA images perpendicular to the femoral tunnel axis.
Results:
MRA images showed high signal intensity in the superior portion of the graft in the femoral tunnel in 94.7% and 60.9% of the ALD patients and FLD patients, respectively, a statistically significant difference (P = .03).
Conclusion:
MRA images at 3 months after surgery revealed that blood flow reached the superior end of the tendon graft in the femoral tunnel in more patients who underwent ACL reconstruction with an ALD compared with an FLD.
A graft from the hamstring tendon is commonly used for reconstructing the anterior cruciate ligament (ACL), and good clinical outcomes can be achieved with this procedure. 2,9,13,14,18 However, blood loss from the harvested tissue while outside the body can lead to relative postoperative necrosis and require up to 1 year for the graft to mature. 7 For maturation to occur, blood flow must resume to the bone tunnel wall and tendon graft within the tunnel. Arai et al 3 measured blood flow using magnetic resonance angiography (MRA) after ACL reconstruction in patients. Those investigators were the first to visualize blood flow to the bone tunnel wall and graft in the tunnel in vivo. Arai et al found that blood flow resumed from the superior, medial, and inferior genicular arteries to the tunnel wall, and blood flow was supplied to the graft in the tunnel. Terauchi et al 23 and Kanamura et al 12 quantified blood flow to the tunnel wall and graft in the tunnel 2 to 6 months after ACL reconstruction. Both studies found that blood flow reached the wall at 2 months and the graft area at 3 months after surgery. The findings confirm that blood flow between the tunnel wall and the graft within the tunnel is important for graft maturation and suggest that contact between the tunnel wall and the graft is vital.
When the graft tendon is fixed to the femoral side, a method is used in which sutures forming an anchor and a loop are integrated. Two types of devices can be used, an adjustable-loop device (ALD) and a fixed-loop device (FLD), by which the loop length can and cannot be adjusted, respectively, after the anchor has been flipped. For FLD it is necessary to make the femoral tunnel longer than the graft portion that must be inserted (Figure 1). This means that when FLD is used, there is a gap between the tip of the graft and the upper end of the tunnel. Thus, the area of contact between the graft and the upper end of the tunnel wall is greater when using ALD than when using FLD, such that ALD results in greater blood flow to the graft from the tunnel wall, which can enhance graft maturation.

Gap between the tip of the graft and the upper end of the tunnel. Postoperative magnetic resonance angiography images of anterior cruciate ligament reconstruction using a (A) fixed-loop device (FLD) and (B) adjustable-loop device (ALD). Dashed lines indicate the tunnel wall, and solid lines indicate the graft within the tunnel. The tunnel is drilled about 10 mm longer for FLD than for ALD, which results in a gap between the tip of the graft and the superior end of the tunnel.
Because previous studies have shown that blood flow reached the graft area at 3 months after surgery,12,23 the current study aimed to compare the signal strength at the superior end of the graft on MRA images of the tunnel wall and graft area at 3 months after surgery between ALD and FLD. We hypothesized that graft revascularization of this area would be better with ALD than with FLD.
Methods
Participants
Ethics committee approval for this study was obtained from our institution. The study participants had all undergone unilateral ACL reconstruction between 2008 and 2018 at a single hospital and underwent MRA 3 months postoperatively. All surgical procedures were performed by the same surgeons (K.H., A.K., S.A.) using a similar technique and quadrupled semitendinosus tendon grafts; FLD was used until December 2013 and ALD thereafter. Study inclusion criteria were single-bundle reconstructions with quadrupled hamstring tendon, first such injury, follow-up for >1 year, and return to sports at preinjury level without further knee injury 1 year after surgery. Patients with a history of atopic dermatitis, allergies, impaired kidney function, or bronchial asthma were excluded. MRA was performed after written informed consent was obtained.
After we excluded 2 patients whose MRA images were blurred, the remaining patients were divided into 2 groups based on whether FLD or ALD was used. The ALD group consisted of 19 patients (mean age, 22.7 ± 6.5 years; mean BMI, 22.2 ± 1.4), and the FLD group consisted of 23 patients (mean age, 24.0 ± 8.2 years; mean BMI, 21.9 ± 4.0) (Table 1). Patient activity level assessed by the Tegner score showed no significant difference between the 2 groups, however the ratio of males to females was significantly different (P = .01) (Table 1).
Characteristics of the Study Groups a

a Values are expressed as mean ± SD unless otherwise noted. Bolded P value indicates statistically significant difference between groups (P ≤ .05). ALD, adjustable-loop device; FLD, fixed-loop device.
Surgical Technique and Postoperative Rehabilitation
All reconstructive procedures were performed using the inside-out approach under arthroscopic observation. 3 The semitendinosus tendon was harvested and folded into a 4-strand bundle about 6 to 9 mm in diameter. One end of the stump was sutured with No. 0 Surgilon thread (Medtronic), and 4 sutures were placed for fixation. The fixed-loop Endobutton CL (Smith & Nephew) or the adjustable-loop TightRope RT (Arthrex) was attached to the looped end of the graft for the femoral fixation. A Telos artificial ligament made of polyester was connected to the other sutured end of the graft for the tibial fixation. The graft diameter was measured, and tunnels were drilled into the tibia and femur, both wide enough to pull the graft through; the tibial tunnel was 7 to 10 mm, and the femoral tunnel was 6 to 9 mm in diameter. The length of the femoral tunnel was 25 and 15 mm for the Endobutton and the TightRope, respectively (Figure 2).
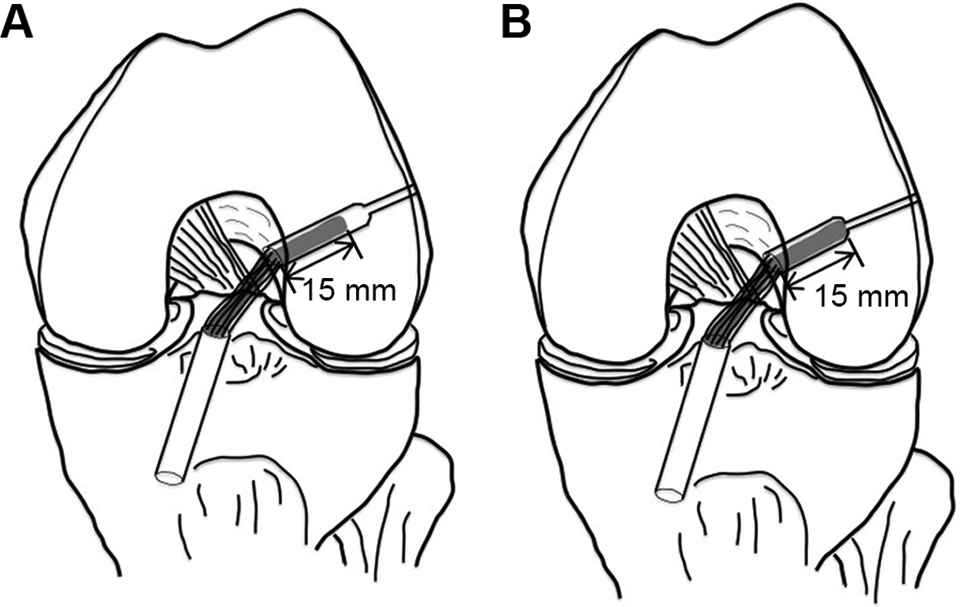
Relationship between grafts and walls in the 2 devices. (A) Use of a fixed-loop device (FLD) requires the femoral tunnel to be 10 mm longer than (B) use of an adjustable-loop device. The length of the inserted graft is kept constant, irrespective of the type of suspension device. Thus, there is a gap between the superior tip of the graft and the superior end of the FLD tunnel.
When the Endobutton CL was used, after the passing sutures and the button were pulled through the femoral tunnel, the following suture was pulled up, and the button was expected to flip when the graft was seated. A mark already made on the implant helped to indicate that the button had exited the femur. When the TightRope RT was used, the femoral tunnel length was marked on the string attached to the implant, and another mark was made 15 mm from the femoral side of the graft. After the button was pulled though the femoral cortex, the tensioning sutures were pulled alternately to seat the graft in the tunnel.
In both methods, the ceramic button was put into the tibial tunnel. The Telos artificial ligament with the semitendinosus tendon was passed through the hole of the ceramic button and then ligated in 20° of flexion with maximum manual leverage. The length of the graft inserted into both the femoral and tibial tunnels was 15 mm. After inserting the graft, we confirmed the absence of roof impingement. Postoperatively, the knee was fixed with a splint in 20° of flexion. Knee range of motion exercises were begun on the second day after surgery. Partial weightbearing was initiated 7 days after surgery. Walking was permitted 4 weeks after and jogging 8 weeks after reconstruction. Return to sports was permitted 6 months after surgery, subject to muscle power evaluation.
Magnetic Resonance Angiography
MRA was performed using a 1.5-T magnetic resonance imaging system (Gyroscan Intera; Philips Medical Systems) with a knee coil, as previously described. 3,23 Several studies have reported that 8 to 12 weeks are required for soft tissue revascularization of the hamstring tendon graft in ACL reconstruction. 8,10,19 Previous studies have shown that it is possible to evaluate revascularization using MRA images of the area. 3,23 In those studies, blood reached the femoral tunnel wall from the superior and middle genicular arteries at 2 months after reconstruction and reached the inner region of the graft inside the tunnel at 3 months. Considering these previous findings, we decided to conduct MRA at 3 months after surgery.
An intravenous infusion line was inserted in the dorsal side of the patient’s hand, and the patient was placed in the supine position with the knee fully extended in the neutral position. For fat suppression images, the water selective excitation technique was used. Contrast-enhanced MRA was performed after intravenous injection of gadolinium
Imaging Analysis
MRA images in the Digital Imaging and Communications in Medicine (DICOM) format were imported into the image software Aquarius NET and reconstructed using the multiplanar image reconstruction method (Figures 3 -5). To this end, oblique sagittal images were imported into Aquarius NET, and cross-sectional images along the femoral tunnel axis were constructed. Transverse images perpendicular to the tunnel axis were also constructed, and the slice closest to the upper end of the graft parenchyma was selected. The distance from the center was set according to the size of the reamer used to drill each tunnel and used to demarcate the tunnel wall and the inserted tendon parenchyma. That signal strength was observed, and the signal strengths of the tunnel wall and graft parenchyma in the tunnel were evaluated.
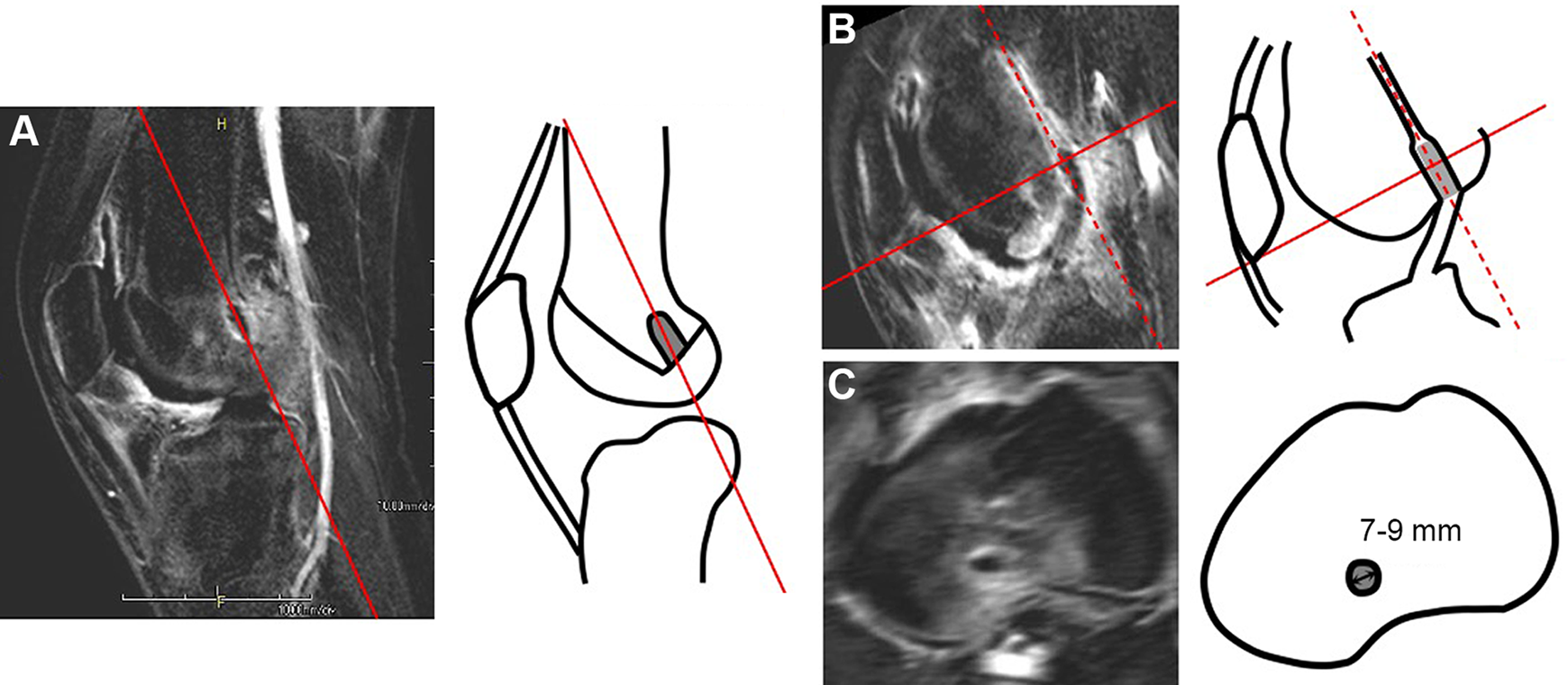
Reconstruction of magnetic resonance angiography scans. Original scans were imported into Aquarius NET and reconstructed via multiplanar reconstruction. (A) Sagittal section. (B) Cross section along the femoral tunnel axis (dashed line). (C) Transverse image perpendicular to the tunnel axis, constructed about the superior end of the implanted tendon. In each case, the tunnel wall was judged to be 7 to 9 mm from the center of the cross section.

Application screen of Aquarius NET: the multiplanar reconstruction method. Magnetic resonance angiography scans were imported into Aquarius NET, and cross-sectional images were constructed. (A, B) A transverse image perpendicular to the tunnel axis was constructed, while (C) coronal and (D) sagittal sections were constructed along the axis of the femoral tunnel at the section where the tunnel was longest.

Image of the selection of slice nearest the upper end of the graft. Signal strength was evaluated on a section perpendicular to the femoral tunnel axis.
The evaluations were performed twice by the same surgeon (A.K.) at intervals of >6 weeks and once by another examiner (K.H.), and intra- and interobserver agreement was measured using the kappa test to calculate the reproducibility. The kappa statistic showed good intraobserver agreement (κ = 0.72) and interobserver agreement (κ = 0.74).
Statistical Analysis
Results were analyzed using StatView 5.0 (Abacus Concepts). The Pearson chi-square test was used to compare the number of grafts in each group that had low or high signal intensity. P values ≤.05 were considered significant.
Post hoc power analysis was performed using G*Power 3. 6 For a total sample size of 42 and type I error (α) of .05, the study was expected to provide a power (1 − β) of 0.90 for detecting an effect size of 0.5.
Results
The tunnel wall, which is continuous with the bone marrow, had markedly higher signal strength at the periphery, and the signal strength of the graft in the tunnel was lower than that in the bone marrow around the wall in 1 patient in the ALD group and 9 patients in the FLD group. In contrast, the signal intensity of the graft in the tunnel was equal to or higher than that in the bone marrow in 18 patients in the ALD group and 14 patients in the FLD group. The data for all patients are provided in Tables 2 and 3.
Clinical Data of Patients in the ALD Group a

a ALD, adjustable-loop device; F, female; M, male; MRA, magnetic resonance angiography.
Clinical Data of Patients in the FLD Group a
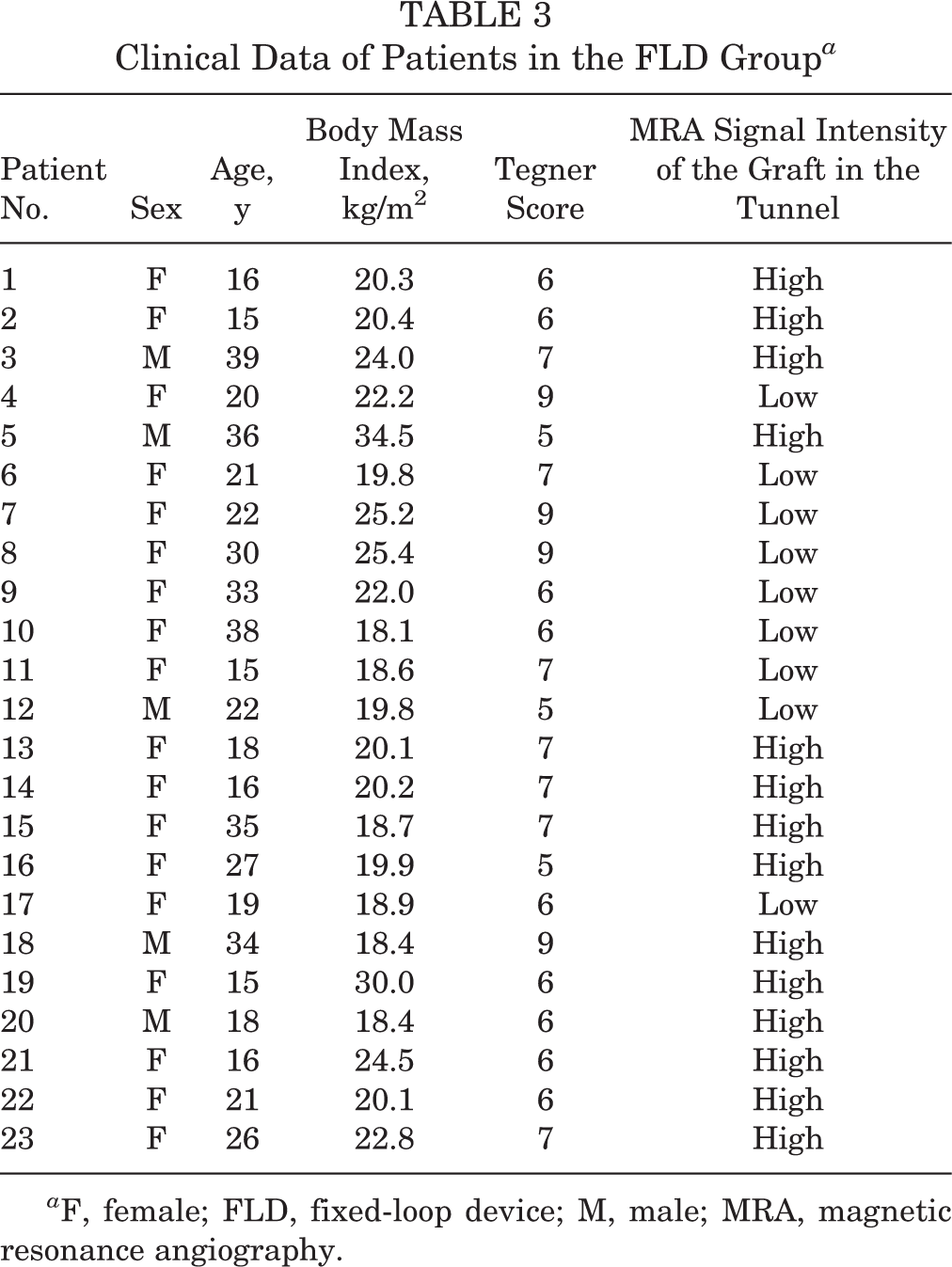
a F, female; FLD, fixed-loop device; M, male; MRA, magnetic resonance angiography.
We found that 18 of 19 knees (94.7%) in the ALD group had high signal intensity, compared with 14 of 23 knees (60.9%) in the FLD group (P = .03) (Table 4). Representative examples of patients in the 2 groups are shown in Figure 6.
Results of Imaging Analysis a

a Data are reported as n (%). ALD, adjustable-loop device; FLD, fixed-loop device.

Representative examples. (A) A 25-year-old man in the adjustable-loop device group with high signal intensity of graft. (B) A 33-year-old woman in the fixed-loop device group with low signal intensity of graft.
Discussion
The most important finding of this study was that in the early phase after ACL reconstruction, the signal strength of the superior end of the graft in MRA was better with ALD than with FLD. To our knowledge, this is the first study to show that ALD is superior to FLD with regard to revascularization of the graft in the femoral tunnel.
In previous studies, investigators used original sagittal MRA images, with the tunnel as the axis, to evaluate blood flow in the region where the graft was in contact with the wall. 12,23 Only FLD was used in those studies, and it was shown that blood flow reached the side of tunnel wall at 2 months and the graft area in the femoral tunnel at 3 months after surgery. In the present study, because we compared the blood flow at the superior end of the graft, which is in contact with the superior end of the tunnel in the ALD group but not in the FLD group, we used the original sagittal MRA scan to reconstruct transverse images perpendicular to the femoral tunnel axis. The images were evaluated by 2 examiners. This appeared to be a reliable qualitative assessment, because the kappa values for intra- and interobserver agreements were 0.72 and 0.74, respectively.
Our finding suggests that revascularization occurs in that area more readily after the ALD procedure in the early postoperative period. This mechanism is due to the difference in contact area between the tendon and the tunnel wall of the 2 types of devices. During surgery, we varied the tunnel diameter to match the thickness of the tendon graft. Therefore, for both femoral cortical suspension devices, the graft touched the tunnel side walls. The same length of graft (15 mm) was pulled into all femoral tunnels. In the ALD procedures, because the tunnel was 15 mm long, the superior end of the graft contacted the superior end of the tunnel. However, in the FLD procedures, the tunnel was drilled 10 mm longer for the flip, resulting in a gap between the graft tip and the superior end of the tunnel. For this reason, the 2 femoral cortical suspension devices used in ACL reconstruction in this study resulted in different sizes of contact area between the femoral tunnel wall and graft inside the tunnel (Figure 2). In calculating all contact areas schematically, when the length of radius of the graft is r, the contact area between the graft and the tunnel in the ALD group is 30πr + πr 2 and that in the FLD group is 30πr. The difference in the contact area between the 2 groups is πr 2. This area is the superior end of the tunnel. Because the width of the graft and the tunnel in this study was 7 to 9 mm, the difference in the contact area ratio was 12% to 15% greater in the ALD group than in the FLD group (Figure 7).
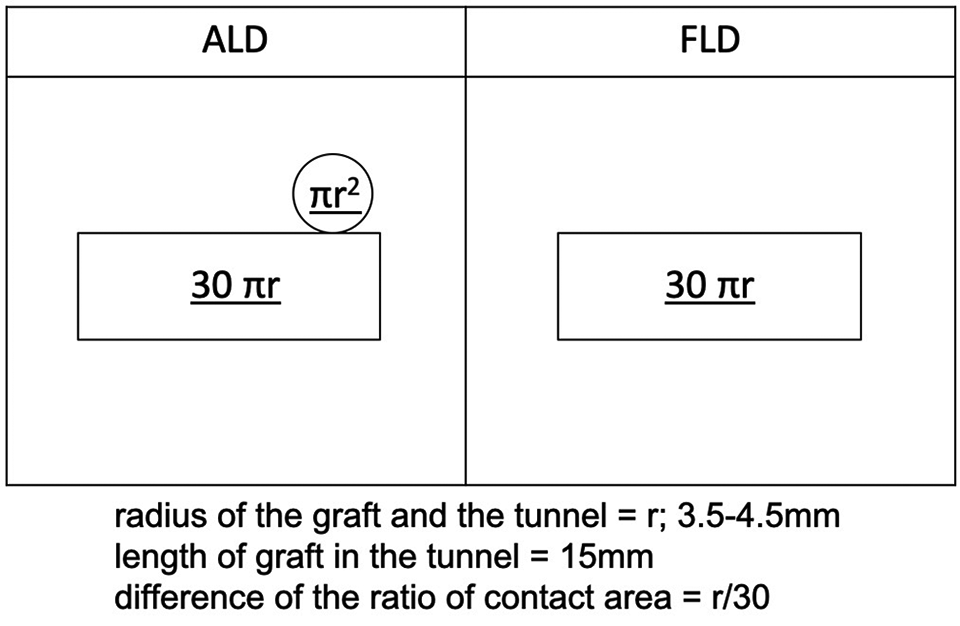
Difference in contact area between the adjustable-loop device (ALD) and fixed-loop device (FLD). When the length of the radius of the graft is r, the contact area between the graft and the tunnel in the ALD group is 30πr + πr 2 and in the FLD group it is 30πr. The difference in the contact area between the 2 groups is πr 2. Because the width of the graft and the tunnel in this study was 7 to 9 mm, the difference in the contact area ratio was 12% to 15% greater in the ALD group than in the FLD group.
Therefore, the blood flow in the graft probably improved more in the ALD group than in the FLD group because of the greater contact area (12%-15%) between the superior tip of the graft and the superior end of the tunnel wall in the ALD group.
A study in dogs reported that regeneration of blood vessels between the flexor digitorum profundus tendon inserted into a bone tunnel and the periphery of the tunnel promoted fusion of the graft to the bone. 5 Another study showed the presence of blood vessels between the bone tunnel tendon graft and the bone tunnel wall in humans, 16 suggesting that regeneration of blood vessels between the graft and tunnel wall is important for blood supply to the graft. Combining this information with the findings from previous studies regarding MRA, 3,12,23 it appears that the supply of blood to the graft by intermediary blood vessels is important in the regeneration of the graft’s blood flow, and the greater the contact area between the graft and the tunnel wall, the more the blood supply reaching the tunnel wall promotes the regeneration process. At 3 months after surgery in the current study, because the ALD group had a greater blood supply to the upper tip of the graft than did the FLD group, the larger contact area between the graft and tunnel wall afforded by the ALD probably better facilitated revascularization.
Other studies have shown differences between the 2 types of femoral suspension devices. Many of those studies were in vitro and biomechanical. 1,4,11,20,22 In several biomechanical studies, FLD was considered excellent with respect to its fixation. 1,4,11,22 However, some studies reported no difference between ALD and FLD with respect to outcomes in the early stages. 20 The current study is the first to compare graft revascularization in vivo between the 2 devices, focusing on the contact area between the graft and tunnel wall. The results of this study suggest that graft revascularization is better with ALD than with FLD. We also provided information for further histological and clinical study regarding the relationship between the contact area and revascularization of the graft in the tunnel wall.
The current study had a few limitations. There was a significant difference in the male-female ratio between the 2 groups, which introduced a confounding variable. Some reports have indicated no sex-related differences in graft failure rate 17 and clinical outcomes, 15,21 but we found no studies on sex-related differences in blood flow reconstruction from the bone to the graft. In a future study, it will be necessary to increase the number of participants and reexamine this topic with equal male-female ratios (1:1). We did not determine whether revascularization between the sides of the tunnel and the graft was the same in both groups. The reconstructed images were distorted compared with the original images, and the amount of slicing was limited. The current study did not include a clinical assessment. However, the favorable results of the ALD group in this study provide important information for future clinical studies to investigate whether an increase in blood flow can allow active rehabilitation in the early stage after ACL reconstruction and decrease the failure rate.
Conclusion
Using reconstructed MRA images taken early after ACL reconstruction surgery, we were able to focus on the area near the superior end of the tendon graft in the femoral tunnel. Evaluation and comparison of patients undergoing ALD and FLD procedures revealed that blood flow reached the tendon graft in the superior end of the graft in the femoral tunnel in more ALD patients than in FLD patients at 3 months after ACL reconstruction.
Footnotes
Acknowledgment
The authors thank the Department of Radiology at Kyoto Kuramaguchi Medical Center for help in setting the conditions of imaging and giving advice about image analysis.
Final revision submitted October 15, 2020; accepted November 23, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Japan Community Heath Care Organization Kyoto Kuramaguchi Medical Center (ERB-C-159-1).