
Abstract
Background:
Adequate graft size and length are crucial factors that correlate with improved outcomes after anterior cruciate ligament reconstruction with a semitendinosus (ST) tendon autograft alone. Anthropometric parameters could be used as predictors of graft measurements but they have shown imprecise correlation in some patients.
Purpose:
To evaluate the accuracy of ultrasound (US) for the preoperative evaluation of ST graft size and length.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 40 patients were included in this study. Patient sex, age, anthropometric parameters, and preoperative US measurements were recorded. After the ST tendons were harvested, their lengths as well as the diameters of the 4-strand ST grafts were recorded. Correlations between patient US measurements were analyzed. Inadequate ST graft length was defined at <28 cm, and inadequate 4-strand ST graft diameter was defined at <8 mm.
Results:
The prevalence of patients with an ST graft length <28 cm was 47.5%, and the prevalence of patients with a 4-strand ST graft diameter <8 mm was 42.5%. US measurements had a strong, significant correlation with the ST graft length (P < .001) and a moderate correlation with the 4-strand ST graft diameter (P < .001). Absolute agreement between the preoperative US measurement of ST graft length and the intraoperative ST graft length showed good reliability (ICC2,1 = 0.825). The cross-sectional area (CSA) of the ST tendon at the knee joint level by US showed a weak correlation (r = 0.207) with the 4-strand ST graft diameter (P = .200). A CSA of 16 mm2 measured by US could be used to predict a 4-strand ST graft diameter ≥8 mm, with a sensitivity of 73.9% and specificity of 76.5%.
Conclusion:
Preoperative US measurements of ST tendons had a strong correlation with intraoperative ST graft length and provided good sensitivity to detect a 4-strand ST graft diameter ≥8 mm. All other anthropometric parameters showed a weak to moderate correlation with ST graft length and size.
Keywords
Hamstring (HS) autografts have become increasingly popular for anterior cruciate ligament (ACL) reconstruction because the long-term outcomes after reconstruction are comparable with those with bone–patellar tendon–bone (BPTB) autografts. HS grafts have shown lower donor site morbidity such as kneeling pain, anterior knee pain, and rate of osteoarthritis compared with BPTB grafts. 15,18,26 However, studies have found knee flexion weakness in patients after harvesting HS tendons for ACL reconstruction, which is a common complaint. 8,20 The weakness was considerably greater in cases when the gracilis (G) tendon was harvested in addition to the semitendinosus (ST) tendon. Therefore, some authors have suggested that the G tendon should be preserved if a single ST graft is adequate for ACL reconstruction. 13
When a single 4-strand ST graft is to be used, the surgeon should preoperatively evaluate the adequacy of the graft in length and diameter. Studies have shown a correlation between graft length and patient anthropometric characteristics. 11,19 Patient height appears to be an acceptable predictor to evaluate the adequacy of the graft, but the strength of the prediction depends on the sex and race of the patient. 11,19
As an imaging modality, 3-dimensional computed tomography (3D-CT) has demonstrated a strong correlation with graft length but a weak correlation with graft size. 27 Magnetic resonance imaging (MRI) could be used to estimate graft size, 6 however in general practice, 3D-CT and MRI are not performed in all of the cases. Therefore, we intended to evaluate ultrasound (US) as a screening tool that would help the surgeon choose an adequate ST graft. The primary aim of this study was to assess the accuracy of US measurements for the preoperative evaluation of ST graft length and size.
Methods
Patients
Forty patients scheduled for ACL reconstruction with an HS graft were prospectively enrolled in this study from June 2017 to May 2018. The exclusion criteria were scarring of the knee area and previous harvesting of an HS graft. In case the ligament of the patient was too small or short according to US, the patients were advised that reconstruction with both ST and G grafts might be necessary using a 4- or 5-strand HS graft. An ST tendon length <28 cm was defined as an inadequate graft length. It is our routine practice to use a minimum length of 7 cm for a single 4-strand ST autograft in ACL reconstruction, in which the graft is divided into 3 parts: 2 cm in the femoral tunnel, 2.5 cm in the intra-articular tunnel, and 2.5 cm in the tibial tunnel. Inadequate diameter for a 4-strand ST graft was defined as <8 mm. Patient characteristics are shown in Table 1.
Patient Characteristics a
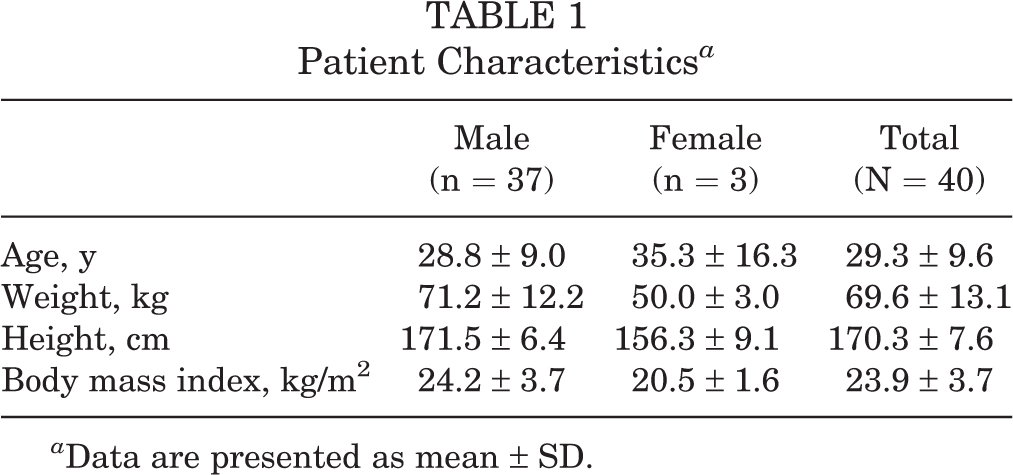
a Data are presented as mean ± SD.
Ultrasound
Preoperative US measurements, patient sex, age, and anthropometric parameters were recorded. A musculoskeletal radiologist with 10 years of experience (P.T.) performed all US imaging in this study. The midportion of the ST tendon was identified first at the posteromedial aspect of the knee in the cross-sectional view. We then traced along the ST tendon proximally and distally to identify the musculotendinous junction and the insertion point at the pes anserinus. Two points, the proximal and distal sites, were then marked on the patient’s skin, and the length of the ST tendon was measured. The diameter and cross-sectional area (CSA) of the ST tendons were measured on US at the knee joint level (Figure 1).

(A) The ultrasound probe was placed at the posteromedial aspect of the knee joint level, and (B) the size of the semitendinosus tendon was measured.
Surgical Procedure
Two orthopaedic surgeons (S.S., Artit Boonrod) performed all procedures by using the same ST tendon harvesting technique. A 3-cm skin incision was made over the pes anserinus parallel to the skin crease. The fascia was incised parallel to its fiber, and then the ST and G tendons were identified. ST tendons were harvested with a closed tendon stripper (Figure 2), and the length of the ST tendon was recorded. The ST tendons for the 4-strand graft were prepared. Then, the diameters of the 4-strand ST grafts were measured using Acufex sizing tubes (Smith & Nephew). If the ST graft length was <28 cm, or the 4-strand ST graft diameter was <8 mm, both the ST and the G tendons were harvested for ACL reconstruction.

The semitendinosus tendon was harvested with a closed tendon stripper.
Statistical Analysis
Patient data are reported as means and standard deviations. Absolute agreement between the preoperative US measurements of ST graft length and the intraoperative ST graft lengths was analyzed with the intraclass correlation coefficient (ICC). The correlation between the preoperative US measurements of CSA and the intraoperative 4-strand ST graft diameters was analyzed with the Pearson correlation coefficient. The correlation between the anthropometric parameters and the intraoperative findings was also analyzed with the Pearson correlation coefficient. The sensitivity and specificity of US to detect an ST graft length <28 cm and a 4-strand ST graft diameter <8 mm were investigated by using 2-by-2 contingency tables. Statistical significance was set at P < .05 in all analyses. SPSS Statistics for Windows (version 25.0; IBM) was used for statistical analysis.
Results
The prevalence of patients with an ST graft length <28 cm was 47.5%, and the prevalence of those with a 4-strand ST graft diameter <8 mm was 42.5%. The mean ST graft length was 27.63 ± 1.92 cm. All of the female patients had an ST graft length <28 cm, and 2 (66.7%) female patients had a 4-strand ST graft diameter <8 mm. Of the 37 male patients, 16 (43.2%) had an ST graft length <28 cm, and 15 (40.5%) had a 4-strand ST graft diameter <8 mm. Eighteen (45.0%) patients required 4-strand ST and G grafts for ACL reconstruction. Also, 1 patient (2.5%) required 5-strand ST and G grafts for ACL reconstruction.
Absolute agreement between the preoperative US measurement of ST graft length and the intraoperative ST graft length showed good reliability (ICC2,1 = 0.825). A 2-by-2 contingency table was created, as shown in Table 2. The sensitivity and specificity of the preoperative US evaluation to detect an ST graft length <28 cm were 94.7% and 76.2%, respectively. The CSA of ST tendons at the knee joint level by US (16 mm2) provided the highest accuracy, with a sensitivity of 73.9% and specificity of 76.5% to predict an adequate (≥8 mm) 4-strand ST graft diameter.
Contingency Table of Diagnosis of Inadequate ST Graft Length (<28 cm) a

a Data are presented as No. ST, semitendinosus.
b As measured on ultrasound.
The correlations between intraoperative findings and patient anthropometric characteristics were analyzed (Table 3). The preoperative US measurement of ST graft length showed a strong correlation (r = 0.772) with the intraoperative ST graft length (P < .001). The preoperative US measurement of ST graft length showed a moderate correlation (r = 0.646) with the 4-strand ST graft diameter (P < .001) (Figure 3). The CSA of ST tendons at the knee joint level by US showed a weak correlation (r = 0.207) with the 4-strand ST graft diameter (P = .200) (Figure 4). Patient height demonstrated a moderate correlation (r = 0.654) with the intraoperative ST graft length (P < .001) and a moderate correlation (r = 0.433) with the 4-strand ST graft diameter (P = .005). Patient thigh length demonstrated a moderate correlation (r = 0.594) with intraoperative ST graft length (P < .001). All of the other anthropometric parameters showed weak correlations with the 4-strand ST graft diameter. Scatter plot showing a strong positive correlation (r = 0.772) between the preoperative ultrasound measurement of semitendinosus (ST) graft length and the intraoperative ST graft length (P < .001). The dotted line is the cutoff point of the acceptable intraoperative ST graft length (28 cm). Scatter plot showing the weak positive correlation (r = 0.207) between the cross-sectional area of the semitendinosus (ST) tendon at the knee joint level by ultrasound (US) and the 4-strand ST graft diameter (P = .200). The dotted line is the cutoff point of the acceptable 4-strand ST graft diameter (8 mm).
15
Correlations of Intraoperative Findings
a
a
CSA, cross-sectional area; ST, semitendinosus; US, ultrasound.
b
The preoperative US measurement of ST graft length showed a strong positive correlation with the intraoperative ST graft length (P < .001).


Discussion
ACL reconstruction with an HS graft is a common procedure in orthopaedics. One of the frequent complications after performing this technique is knee flexor strength deficit, which is more significant if both the ST and the G tendons are harvested. 8,20 To reduce this complication, previous studies have suggested using an ST autograft alone if an acceptable size and length could be obtained. 13 The adequate preparation of a single ST autograft has been a 4-strand graft; however, some patients were found to have inadequate 4-strand ST graft lengths or diameters intraoperatively. Therefore, an accurate preoperative prediction of ST graft size and length could help the surgeon to inform patients and to prepare the proper procedures. Many researchers have studied ways to predict HS graft characteristics, and they have proposed various techniques using anthropometric parameters § or preoperative 3D-CT and MRI measurements. 2,6,27
US can be used to evaluate structures around the knee such as tendons, ligaments, and menisci. 1,3,7,12 The ST tendon can be identified easily by US if one is familiar with the anatomy of the tendon. In this study, we proposed the use of US for the preoperative evaluation of ST graft length and size. The preoperative US evaluation showed excellent sensitivity and greater specificity than any anthropometric parameter to detect an inadequate autograft.
Reboonlap et al 19 evaluated the relationship between the graft length and diameter and anthropometric parameters in 74 male patients. Patient height and leg length showed the strongest correlation (r = 0.603 and 0.610, respectively) with HS graft length; graft diameter did not correlate with any physical parameters. Celiktas 4 found that height had a moderately positive correlation with ST graft length. Height and weight, however, had a weakly positive correlation with graft thickness. Age, thigh circumference, and body mass index did not correlate with graft thickness. Pereira et al 16 studied 64 patients, in which 60 (94%) patients were male and 4 (6%) were female. They found that patient height had the highest positive correlation (r = 0.450; P < .01) with ST graft length. Age, weight, and body mass index did not correlate with graft diameter and length. Similarly, in the current study, we found that height was the best anthropometric predictor, with moderate correlations between it and intraoperative ST graft length and 4-strand ST graft diameter. All other anthropometric parameters had weak correlations with intraoperative ST graft sizes in this study.
Previous imaging studies have reported an excellent significant correlation with the intraoperative HS graft length, but there is still controversy over trying to predict graft diameter. 2,6,27 Measurements using 3D-CT have shown a significant correlation with intraoperative ST graft lengths but no significant correlation with CSAs. 27 The CSAs of HS grafts on MRI and US have demonstrated a moderate correlation with intraoperative HS graft sizes. One study proposed the use of CSA by US (14 mm2) to predict an adequate graft diameter (≥8 mm) and showed a sensitivity and specificity of 80.8% and 100.0%, respectively. 7 Similarly, in the current study, the cross sections of the tendons were elliptically shaped and varied from a quite flat shape to a more circular shape, adding to the challenge of measuring the actual radius and diameter by US. Therefore, we found that the CSA is more suitable than the diameter of the ST tendon on US. In this study, a CSA cutoff of 16 mm2 on US was found to predict an adequate (≥8 mm) 4-strand ST graft diameter with a sensitivity of 73.9% and specificity of 76.5%. The preoperative US measurement of ST graft length showed a strong correlation with the intraoperative ST graft length and a moderate correlation with the 4-strand ST graft diameter. The CSA of ST tendons at the knee joint level by US showed a nonsignificant, weak correlation with 4-strand ST graft diameters.
A limitation of this study was the measurement of CSA. The entire length of the ST tendon at a single site was measured because the ST tendon is most obvious at the level of the knee joint. The ST tendon has different shapes at different sites, which would have different CSAs, and this might be the cause of the weak correlations found in this study. Calculations from several points of measurement along the ST tendon may provide better correlations with the 4-strand graft diameter. Another limitation is that only 3 female patients were included in the study, which were too few to analyze as a subgroup. This might also have affected the results of this study, which was intended to reflect the general population.
Conclusion
Preoperative US measurements of ST tendons have a strong correlation with intraoperative ST graft lengths and a high sensitivity to detect inadequate ST graft lengths. Also, a 16-mm2 CSA of the ST tendon at the knee joint level by US can be used as the cutoff point to predict a 4-strand ST graft diameter ≥8 mm. All other anthropometric parameters showed a weak to moderate correlation with ST graft lengths and sizes.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Khon Kaen University.