
Abstract
Background:
Active rehabilitation has an important role in the management of patellofemoral pain syndrome (PFPS). Although some studies have shown the benefit of hip-muscle strengthening, the effect of combining hip-muscle stretching with strengthening has not yet been defined.
Purpose:
To evaluate the effect of combined strengthening of the hip external rotators and abductors and stretching of the hip internal rotators on pain and function in patients with PFPS.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
A total of 109 patients with PFPS (75 female and 34 male; mean age, 31.6 ± 10.8 years) were first randomly assigned to protocol A (n = 67) of the A-B arm (AB group; standard rehabilitation) or protocol B (n = 42) of the B-A arm (BA group; standard rehabilitation with strengthening of the hip external rotators and abductors and stretching of the hip internal rotators). Each protocol consisted of 3 sessions a week for 4 weeks. After a washout period, corresponding to a symptom-free period, rehabilitation programs were crossed over. A visual analog scale (VAS) evaluating perceived pain, the Functional Index Questionnaire (FIQ), and the Kujala score were administered at baseline, the end of each rehabilitation protocol, and 12 weeks after the completion of the second protocol for each group.
Results:
Until the final follow-up, VAS, FIQ, and Kujala scores were significantly improved in both the A-B and B-A arms (P < .05 for all). Compared with protocol A, protocol B provided significant improvement in terms of pain and function in both the BA (VAS and Kujala; P < .001) and AB (VAS and Kujala; P < .001) groups.
Conclusion:
Combined strengthening of the hip abductors and external rotators with stretching of the hip internal rotators provided better outcomes, which were maintained for at least 12 weeks, in terms of pain and function in patients with PFPS.
Patellofemoral pain syndrome (PFPS) is defined as retropatellar or peripatellar pain resulting from physical and biochemical changes in the patellofemoral joint, typically occurring with activity and often worsening when descending steps or hills or after prolonged sitting. 11 It is one of the most common lower limb disorders. 2 In fact, approximately 1 of 4 people experience 1 episode of PFPS during their lifetime. 23
Advances in the pathophysiological understanding of PFPS have resulted in multiple approaches in the treatment of this condition. For example, excessive femoral internal rotation may increase patellofemoral joint stress and predispose people to PFPS through relative lateral displacement of the patella. 18,21 Excessive hip internal rotation during running, stepping, and landing from a jump has been noted in young, active female patients with PFPS. 22 Furthermore, an association between hip internal rotation during running and PFPS has been identified in a recent systematic review and meta-analysis. 17 These findings were highlighted by dynamic magnetic resonance imaging studies in female patients. 21 Additionally, excessive hip internal rotation has been advanced as a predictor of self-reported pain and function during a stepdown task 16 and the development of PFPS in Naval Academy cadets. 3 Thus, special attention should be given to hip rotators in the rehabilitation of this syndrome.
Global stretching of anterior hip structures was found to be beneficial when associated with aerobic exercises in the management of PFPS, 14 but the effect of including stretching of the hip internal rotators has not yet been studied. Furthermore, weakness of the hip abductors and external rotators has commonly been found in patients with PFPS, and strengthening of these muscle groups is beneficial when associated with knee-focused rehabilitation programs. 7,20
The aim of our study was to evaluate the effect of combining strengthening of the hip external rotators and abductors with stretching of the hip internal rotators on pain and function in patients with PFPS. We hypothesized that combining strengthening of the hip abductors and external rotators with stretching of the hip internal rotators would lead to better outcomes.
Methods
Study Design
A randomized, controlled, single-blinded crossover study was carried out. This type of design was chosen to reduce variability between participants and allow for a smaller sample size. All eligible patients were informed about the study and gave consent (consent for patients younger than 18 was given by a parent or guardian). We obtained approval from the hospital ethical committee before beginning patient recruitment.
Patients
Patients between 14 and 50 years of age referred to a single institution for PFPS were eligible for this trial. This large age range is justified by the significant incidence of PFPS in not only young patients but also middle-aged ones as well as the wide patient recruitment in our daily clinical practice. Patient enrollment began in January 2015 and ended in May 2016.
Inclusion and Exclusion Criteria
Included patients were those diagnosed with PFPS, regardless of their activity level. The diagnosis was established by the referring physician and confirmed in all cases by a physiatrist with 14 years of experience in the management of musculoskeletal disorders (A.J.). The diagnosis was retained when symptoms were located in the peripatellar and/or retropatellar area and reproduced with at least 1 of the following activities: stair descent, squatting, kneeling, and prolonged sitting. Symptoms had to be present for at least 3 months, and other anterior knee pain such as referred pain caused by hip and spine disorders was ruled out through a thorough clinical examination and, if needed, radiological investigations such as computed tomography and magnetic resonance imaging. Patients with a history of knee osteoarthritis, injury or surgery, neurological disorders impairing the lower limbs, or systemic inflammatory disorders were excluded from the study.
Randomization
Patients were assigned to 1 of the 2 intervention arms using a computer-generated, random number table.
Interventions and Assessment Rate
Participants were evaluated at baseline and randomly assigned to receive protocol A of the A-B arm (AB group) or protocol B of the B-A arm (BA group). Protocol A is considered to be the standard protocol for treating PFPS. It consisted of transcutaneous electrical nerve stimulation (2 minutes); patellar mobilization (2 minutes); hamstring, quadriceps, and tensor fasciae latae muscle stretching; open kinetic chain strengthening of the quadriceps (concentric exercises); and proprioceptive exercises. Muscle strengthening was performed using weightbearing pulley systems with an intensity of 60% of the patient’s 1-repetition maximum. Protocol B supplemented protocol A with concentric strengthening of the hip external rotators and abductors using weightbearing pulley systems as well as stretching of the hip internal rotators. In each session, 4 repetitions of static stretching were performed manually by the physical therapist. Each repetition was maintained for 30 seconds at a point of mild discomfort but not pain. A resting interval of 20 seconds was observed between stretching repetitions.
Both protocols lasted for 4 weeks and included 12 rehabilitation sessions. Functional status, pain intensity, and knee and hip range of motion were assessed by the same physiatrist, who was unaware of patient allocation, at the end of the first protocol. Patients were instructed to return after a washout period so they could be assigned to the other protocol (crossover of programs). The washout period corresponded to a symptom-free period. It was measured for each patient and lasted from the end of the first protocol to the next consultation based on the patient’s request after symptom recurrence. Patients were evaluated at the end of the second protocol and a third time at 3 months after they had finished the second protocol (Figure 1).

Flowchart of the study. PFPS, patellofemoral pain syndrome.
Outcome Measures
The main outcome measures were pain and function. Pain was assessed using a visual analog scale with a range from 0 (no pain) to 100 (worst pain imaginable). Function was evaluated using 2 measures: the Kujala score and the Functional Index Questionnaire (FIQ). The Kujala score or “anterior knee pain scale,” which is a self-administered questionnaire for patients with PFPS, ranging from 0 to 100, with a lower score reflecting poorer functional capacity, is one of the commonly used assessment tools that has been developed for the evaluation of patients with patellofemoral disorders. It consists of 13 questions that relate to specified activities and pain severity and addresses clinical symptoms. 13 The Kujala score is a valid and reliable measure of anterior knee pain. 10 The FIQ is composed of 8 questions regarding aggravating activities for PFPS and was found to be a good discriminator for measuring clinical changes in these patients. 4 The score for this questionnaire ranges from 0 to 16, with a lower score reflecting poorer functional capacity. Although the FIQ exhibited poor day-to-day reliability, it has been shown to be a valid measure for the detection of clinical changes. 4
Statistical Analysis
Statistical analyses were performed using SPSS Version 21.0 software for Windows (IBM). We compared the means for quantitative variables before and after treatment using analysis of variance. The Student t test for paired samples was used to compare quantitative variables between treatment protocols. P < .05 was considered significant. The effect size for comparisons was determined using the Cohen d.
Results
A total of 149 patients with PFPS were recruited. Of these patients, 40 did not meet the inclusion criteria (Figure 1). We enrolled 109 patients, including 75 female patients, with a mean age of 31.6 ± 10.8 years. There were no significant differences in demographics or clinical scores between the groups at baseline (Table 1).
Baseline Characteristics a

a Data are reported as mean ± SD unless otherwise indicated. FIQ, Functional Index Questionnaire; VAS, visual analog scale.
The mean washout period was longer for patients in the BA group than in the AB group (28.0 ± 14.3 vs 21.4 ± 11.2 weeks, respectively; P = .009). In both the AB and BA groups, pain and functional status were statistically significantly improved after protocol A and protocol B. These improvements were maintained to the end of the study protocol (Table 2). Overall, protocol B provided a more significant improvement compared with protocol A in terms of pain and function (P < .001 for all) (Table 3).
Changes in Pain and Functional Scores a

a Data are reported as mean ± SD. P 1: baseline vs end of first protocol; P 2: baseline vs end of second protocol; and P 3: baseline vs 3 months after end of second protocol. ES, effect size; FIQ, Functional Index Questionnaire; VAS, visual analog scale.
Improvement in Pain and Function a
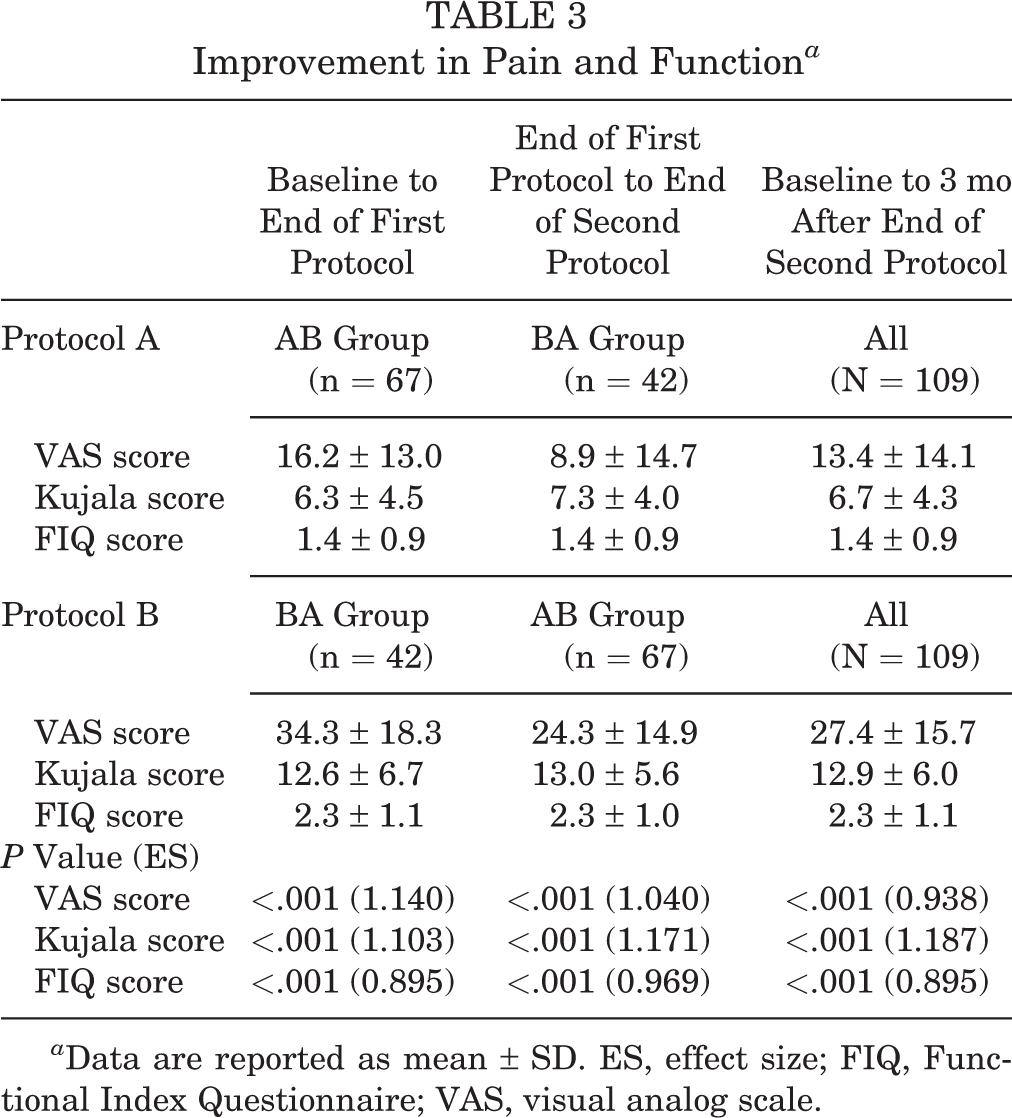
a Data are reported as mean ± SD. ES, effect size; FIQ, Functional Index Questionnaire; VAS, visual analog scale.
Discussion
Our randomized crossover study demonstrated that combining strengthening of the hip external rotators and abductors with stretching of the hip internal rotators in association with a standard rehabilitation program provided significantly better improvement in terms of pain and function in patients with PFPS than a standard rehabilitation program alone.
Our results are concordant with those reported by Fukuda et al, 7 who conducted a randomized controlled trial to investigate the influence of strengthening the hip abductors and lateral rotators on pain and function in female patients with PFPS. They reported that rehabilitation programs focusing on knee-strengthening exercises and knee-strengthening exercises supplemented by hip-strengthening exercises were both effective in improving function and reducing pain in sedentary women with PFPS. Furthermore, improvements in pain and function were greater for the group that performed the hip-strengthening exercises.
The beneficial effects of hip-muscle strengthening have been reported by several authors. Dolak et al 5 found that compared with quadriceps strengthening, hip strengthening provided better outcomes in terms of pain and function in women with PFPS. They added that hip strengthening may initially be more efficient, facilitating muscle training while reducing the exacerbation of patellofemoral symptoms. The benefit of hip-strengthening exercises has been confirmed, regardless of whether the method of muscle strengthening was open kinetic chain exercises 5 or closed kinetic chain exercises. 9
Based on their trial comparing isolated hip abductor and external rotator strengthening to no exercise, Khayambashi et al 12 concluded that the incorporation of hip strengthening exercises should be considered when designing a rehabilitation program for female patients with PFPS. A 6-week supplementation of strengthening of the hip abductor and lateral rotator muscles in a quadriceps exercise program provided additional benefits in patients with PFPS. 15,19 However, these results contrast with the findings of Avraham et al, 1 who found no difference between hip external rotator and quadriceps strengthening compared with quadriceps strengthening alone. This could be explained by the relatively small sample size and the short follow-up period in their study.
The role of hip- and core-focused rehabilitation in PFPS has been reported. Ferber et al 6 conducted a single-blinded, multicenter randomized controlled trial in which they compared patients with PFPS assigned to either a hip- and core-focused or a knee-focused 6-week rehabilitation protocol. They found that the hip- and core-focused rehabilitation protocol provided an earlier resolution of PFPS and greater overall gains in muscle strength and core endurance than did a knee-focused protocol. 6
We could not find any studies evaluating the effect of a rehabilitation program combining hip rotator muscle strengthening and stretching in patients with PFPS; however, generalized stretching protocols including the quadriceps, iliotibial band, gastrocnemius, and hamstring were reported to have benefits when combined with a strengthening program, as demonstrated by Moyano et al. 14 Halabchi et al 8 demonstrated that significantly greater improvements in pain and function could be obtained with an individualized rehabilitation program incorporating specific stretching for hip muscles in patients with PFPS who demonstrated inflexibility on examination.
The washout period served as an indicator of the efficacy of the first administered protocol. The crossover design allowed us to evaluate both interventions in the same population, thus reducing recruitment bias and increasing the number of treated patients.
Limitations
The major limitation of our study was the fact that the washout period remained subjective and dependent on the patient’s perception of pain. In addition, participants were not blinded, possibly creating a bias in recording these subjective complaints. Another limitation was the fact that we recruited patients from third-line therapy. The lack of a power analysis to estimate the number of patients needed during the planning stage of the study is certainly another limitation, but our sample size remains among the largest in the PFPS literature.
Conclusion
Findings from this study confirm the interest in strengthening hip external rotators and abductors in patients with PFPS. A program of 3 sessions a week for 4 weeks improved pain and function with maintained benefits for at least 12 weeks beyond the intervention period. These results suggest the usefulness of adding hip internal rotator stretching exercises in a rehabilitation program, but their specific benefit remains unclear. As such, further high-quality clinical trials are needed.
Footnotes
Final revision submitted August 22, 2020; accepted September 30, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.