
Abstract
Background:
The prevalence of findings on shoulder magnetic resonance imaging (MRI) is high in asymptomatic athletes of overhead sports.
Purpose/Hypothesis:
The purpose of this study was to determine the prevalence of atypical findings on MRI in shoulders of asymptomatic, elite-level climbers and to evaluate the association of these findings with clinical examination results. It was hypothesized that glenoid labrum, long head of the biceps tendon, and articular cartilage pathology would be present in >50% of asymptomatic athletes.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 50 elite climbers (age range, 20-60 years) without any symptoms of shoulder pain underwent bilateral shoulder examinations in addition to dedicated bilateral shoulder 3-T† MRI. Physical examinations were performed by orthopaedic sports medicine surgeons, while MRI scans were interpreted by 2 blinded board-certified radiologists to determine the prevalence of abnormalities of the articular cartilage, glenoid labrum, biceps tendon, rotator cuff, and acromioclavicular joint.
Results:
MRI evidence of tendinosis of the rotator cuff, subacromial bursitis, and long head of the biceps tendonitis was exceptionally common, at 80%, 79%, and 73%, respectively. Labral pathology was present in 69% of shoulders, with discrete labral tears identified in 56%. Articular cartilage changes were also common, with humeral pathology present in 57% of shoulders and glenoid pathology in 19% of shoulders. Climbers with labral tears identified in this study had significantly increased forward elevation compared with those without labral tears in both active (P = .026) and passive (P = .022) motion.
Conclusion:
The overall prevalence of intra-articular shoulder pathology detected by MRI in asymptomatic climbers was 80%, with 57% demonstrating varying degrees of glenohumeral articular cartilage damage. This high rate of arthritis differs significantly from prior published reports of other overhead sports athletes.
Keywords
Rock climbing is an increasingly popular sport worldwide, and its participation is expected to increase given the recent addition of sport climbing to the 2020 Olympic Games. 18,23 As of 2016, there were an estimated 6 million participants in the United States alone. 40 Furthermore, there are more than 430 climbing gyms in the United States, with an average of 8% growth in the number of gyms opening every year for the last 5 years. 11,15 As participation increases, sports medicine and upper extremity clinicians are beginning to see climbers more frequently, necessitating an increased awareness of sport-specific injuries and treatments.
Despite the perceived risk associated with climbing, acute injuries are relatively rare, with only a 0.2% to 0.4% incidence of accidents and approximately 0.02 acute injuries per 1000 hours of climbing. 32,35 However, given the sport’s combination of sustained isometric contractions (Figure 1) coupled with explosive maneuvers, as well as frequent overhead holds at the extremes of motion (Figure 2), overuse injuries are common. 4,6,33,37 Specifically, because of the frequent and extreme overhead positions and upper extremity workload experienced during climbing, shoulder injuries are especially common. Rotator cuff tendonitis, impingement, and biceps tendonitis are the most reported conditions. 2,4 –6,16,32

Climber demonstrating an example of a hold and a sustained isometric contraction of near 100% body weight.
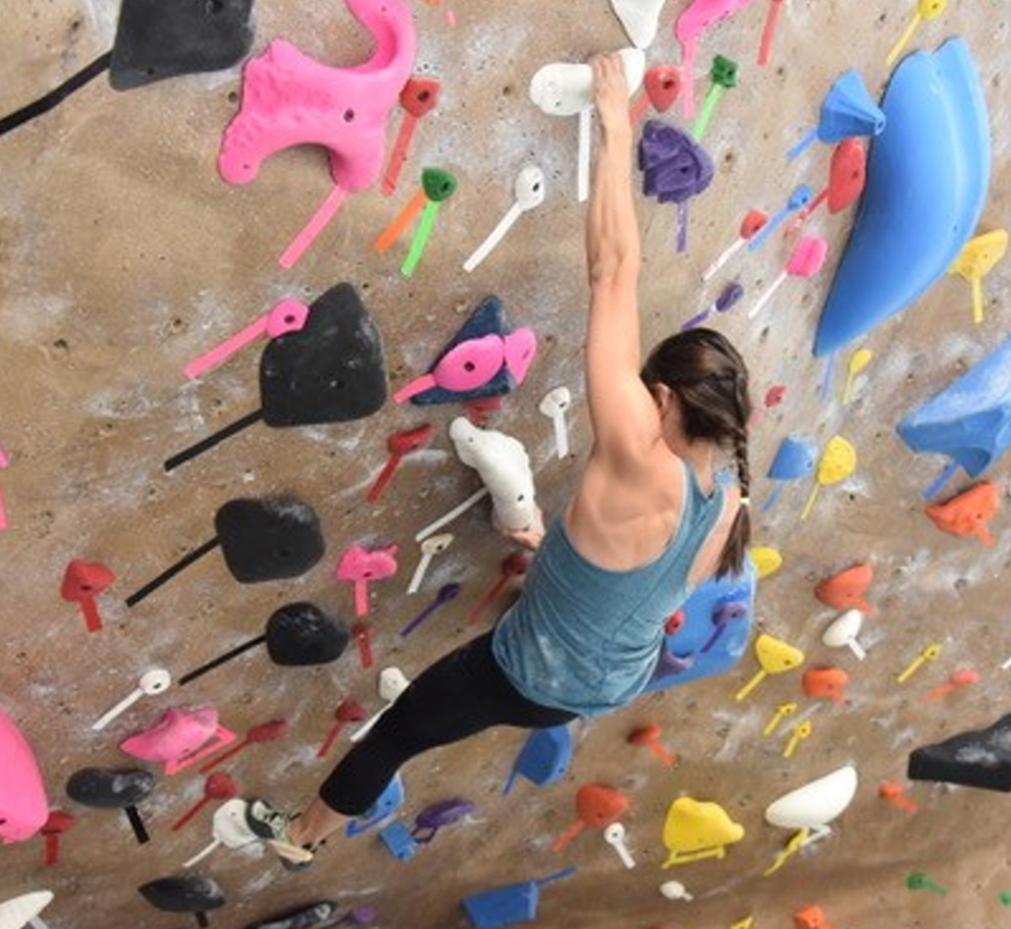
Climber demonstrating an example of a hold at the extremes of upper extremity motion.
Magnetic resonance imaging (MRI) is the most common tool for evaluating soft tissue injuries of the shoulder. 9 It is important to know the prevalence of asymptomatic findings to help with evaluation and clinical decision-making and to avoid exposing patients to unnecessary surgery. 31 Multiple studies have demonstrated that overhead athletes including pitchers or throwers frequently have asymptomatic shoulder findings on MRI. Miniaci et al 27 demonstrated a 79% prevalence of asymptomatic labral abnormalities in professional baseball pitchers, with similar findings demonstrated in volleyball and water polo players. 22,24 To date, there is a paucity of published literature focusing on shoulder MRI findings that exist in rock climbers.
The purpose of our study was to determine the prevalence of pathologic shoulder findings observed on MRI evaluation of asymptomatic, elite-level climbers and correlate such findings with the clinical examination results of these athletes. It was hypothesized that glenoid labrum, long head of the biceps tendon, and articular cartilage pathology would be present in >50% of asymptomatic athletes.
Methods
Participants
After receiving approval from a local institutional review board, we prospectively enrolled 50 volunteer elite rock climbers from January 2019 to October 2019. Recruitment was aided by advertisements in climbing gyms in Colorado, USA, and across various online platforms, such as climbing training and route forums, as well as through social media.
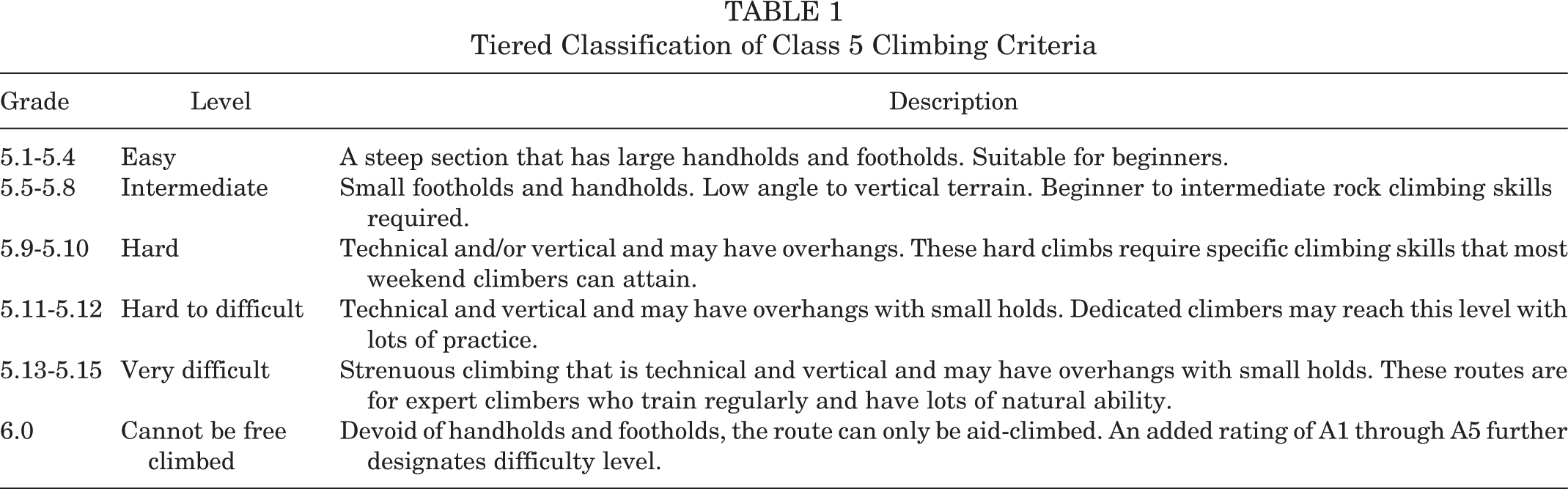
Climbers were eligible to participate in the study if they had been climbing at a grade of 5.11 or higher for at least 5 years; had no shoulder-related complaints; had no history of previous shoulder surgery or significant injury, including previous shoulder surgery or dislocation, rotator cuff or glenoid labrum tear, or fracture; and were willing and able to undergo MRI. Climbing route difficulty is rated on a graded scale based on the slope and technical complexity of the route. Grades 1 and 2 are hiking trails, grade 3 is hard hiking with possible scrambling and varying amounts of exposure, and grade 4 is bouldering or climbing that does not require a rope. Grade 5 is considered true rock climbing and is subdivided by a decimal system (Table 1). Grades 5.0 to 5.4 are considered easy rock climbing, 5.5 to 5.8 are considered intermediate, and 5.11 and greater are considered difficult. Interested candidates were screened for eligibility through email correspondence with members of the study team before an appointment for their MRI was scheduled.
Tiered Classification of Class 5 Climbing Criteria
Evaluation
Shoulder MRI scans with imaging in the sagittal, coronal, and axial planes were obtained using a Siemens Magnetom SkyraFit 3-T MRI scanner (Siemens Medical Solutions USA) with shoulder coil (16-channel, Siemens) through a shoulder-specific protocol (Table 2).
Shoulder MRI Protocols a

a FS, fat saturation; MRI, magnetic resonance imaging; PD, proton density; TR, repetition time; TE, echo time; TSE, turbo spin echo.
All climbers additionally underwent clinical evaluation of bilateral shoulders at the same appointment as their MRI scan, subjecting the participants to a battery of strength, stability, and range of motion tests using a goniometer for each shoulder, as well as provocative and special tests (Table 3). Of note, external rotation motion was measured with the arm adducted to the side. These examinations were performed by 3 sports medicine physicians (J.D.C., M.N.S., T.R.H.) on the research team.
Shoulder Special Tests by Examination Type a

a AC, acromioclavicular; BG, bicipital groove; SLAP, superior labrum anterior to posterior; TTP, tenderness to palpation.
After these appointments, all climbers completed and submitted an online questionnaire that collected data on the level of climbing participation (recreational, professional, etc), frequency of climbing, and level of pain during certain athletic and nonathletic movements involving the shoulder, as well as demographic information (age, sex, height, weight, etc) for each volunteer.
MRI scans were systematically evaluated by 2 experienced fellowship-trained musculoskeletal radiologists (C.P.H., E.K.F.). Both radiologists were blinded to climber activity levels and physical examination findings. Each radiologist, while reviewing the images, followed a checklist for systematic evaluation of each anatomic landmark. After initial review, any discrepancies were resurveyed by both reviewers, and consensus was obtained on all findings. MRI interpretation and classification criteria are listed in Tables 4 and 5. 19
MRI Interpretation and Classification Criteria a

a MRI, magnetic resonance imaging.
Modified Outerbridge Cartilage MRI Classification a

a MRI, magnetic resonance imaging.
Statistical Analysis
To address the primary aims of the study, the prevalence of types of examination and imaging findings was reported descriptively, and bivariate statistical hypothesis testing was performed to test associations between pathologic MRI findings and physical examination findings. The Welch 2-sample t test was used to compare means of continuous variables between binary MRI finding subgroups (with the exception of internal rotation of the shoulder, which was measured with respect to vertebral levels reached by the climber’s thumb, which in turn was analyzed as an ordinal variable using the Wilcoxon rank-sum test). P < .05 was considered statistically significant. All statistical analyses were performed using the statistical programming language R version 3.6.2 (R Core Team).
Results
Participant Characteristics
One hundred shoulders were evaluated from 50 elite climbers. Twenty-one climbers (42%) were women, 48 (96%) were right-hand dominant, and the average age was 34.1 years (range, 20-60 years). All climbers completed clinical evaluations, and all participants completed bilateral shoulder MRI.
Clinical Evaluation
Physical examination findings demonstrated active forward elevation to, on average, 175° ± 5°; external rotation to 67° ± 17°; and internal rotation to a median of T4 (range, C4-T11). All participants had full strength throughout the shoulder. No climber had Neer or Hawkins impingement on examination. One shoulder (1%) had tenderness to palpation (TTP) at the acromioclavicular (AC) joint, 4 shoulders (4%) had TTP at the bicipital groove, and 1 shoulder (1%) had positive results from a Speed test; no shoulder had TTP over the acromion, clavicle, or sternoclavicular joint. No climber had anterior or posterior apprehension on examination.
MRI Findings
A total of 100 MRI scans were available for radiology review. MRI review found tendinosis of the rotator cuff in 80% of shoulders. The supraspinatus had tendinosis in all 80%, the infraspinatus in 53%, and the subscapularis in 18%. No climbers had tendinosis of the teres minor. Intrasubstance rotator cuff tearing was identified in 16% of shoulders, including 11% of in the supraspinatus, 3% in the infraspinatus, and 4% in the subscapularis (Figure 3). Partial tearing, including either bursal or articular, was only present in 6% of participants.

Axial proton density fat-saturated magnetic resonance image demonstrating an intrasubstance subscapularis tendon tear (asterisk).
Biceps tendinosis and subacromial bursitis were exceedingly common at 73% and 79%, respectively. The AC joint showed degenerative changes in 28% of shoulders. Labral pathology was identified in 69% of shoulders. Increased signal with degenerative changes was seen in 23% of shoulders, most commonly in the superior labrum (18%), with anterior, posterior, and inferior tears seen less commonly at 6%, 5%, and 3%, respectively. Discrete labral tears were identified in 56% of shoulders. Tears varied in location; the most common was superior, identified in 36% of shoulders. Posterior, anterior, and inferior tears were present in 16%, 11%, and 7%, respectively.
Cartilage damage of the humerus was identified in 57% of shoulders, with 51% being modified Outerbridge classification 19 grade 3 or higher. Cartilage changes on the glenoid were noted in 19% of the shoulders, with 14% being grade 3 or higher.
Bivariate association analysis (Welch t test) showed that tearing of the anterior labrum (n = 11 shoulders) was significantly associated with higher mean (± SD) active (178 ± 4 vs 174 ± 5; P = .026) and passive (178 ± 4 vs 174 ± 5; P = .022) forward elevation. No other associations between MRI findings and physical examination findings were identified.
Discussion
The most important findings of this study were that in a sample of elite-level climbers, MRI evidence of tendinosis of the rotator cuff, subacromial bursitis, and long head of the biceps tendonitis was exceptionally common, at 80%, 79%, and 73%, respectively. Labral pathology was present in 69% of shoulders, and discrete labral tears were identified in 56%. Articular cartilage changes were also common, with humeral pathology present in 57% of shoulders and glenoid pathology in 19% of shoulders.
Comparison to Other Studies on Shoulder Pathology Prevalence
Labral abnormalities are commonly identified in asymptomatic overhead athletes. 12,17,22,27 Asymptomatic baseball pitchers have labral signal on MRI 79% of the time, 27 with discrete labral tears reported between 36% and 48% of the time. 25,27 Klein et al 22 evaluated MRI findings in water polo players and reported an increased labral signal of between 21% and 53%; however, the discrete tear rate was not reported, and up to 29% of shoulders in that study were in fact symptomatic. Labral pathology in climbers is most similar to that of professional baseball pitchers, with a reported signal rate in our study of 69% and discrete tearing reported in 56%. The extreme arm positions of rock climbing, often holding body weight–equivalent loads at the extremes of shoulder motion, are possible explanations for the prevalent labral pathology.
In the present study, rotator cuff tendinosis was identified in 80% of shoulders, with the majority in the supraspinatus and infraspinatus (in 80% and 53%, respectively, of patients with rotator cuff tendinosis). While it is possible to correlate this with shoulder position, these values are similar to those observed in the asymptomatic shoulders of the general population. 14,26,28,29 In other upper extremity athletes, rotator cuff tendinosis was identified in 79% of the asymptomatic shoulders of professional pitchers. 27 Intrasubstance tears were identified in 16% of climbers’ shoulders, with partial-thickness tears seen in only 6%. Given that surgical treatment of rotator cuff tears is only recommended in large or near-full-thickness rotator cuff tears, 20 the prevalence of severe rotator cuff pathology is relatively rare.
Tendinosis/tendinopathy in the biceps tendon, along with subacromial bursitis, was also an exceedingly common MRI finding in this study, at 73% and 79%, respectively. These rates are higher than those reported in other overhead sports. Water polo reports biceps tendinopathy at a rate of 60.7%, 22 while baseball and hockey demonstrated much lower rates: 0% in baseball pitchers 25,27 and 3% in hockey players. 17 While it is understandable that hockey players may have lower rates of biceps and anterior shoulder tendinopathy because their stick is below their waist and the sport rarely requires overhead motion, the difference between climbers and pitchers is more surprising. It is possible that part of the variation is related to differences in MRI technology. The study imaging of the baseball shoulder was performed in 2002 on a 1.5-T magnet, 27 and it is possible that modern 3-T scanners are more sensitive for detecting intrasubstance signal changes, partial tearing, and edema.
Degenerative changes in the AC joint were present in only 28% of climber’s shoulders. This is similar to the 25% reported in water polo players 22 ; however, it differs from higher rates (29%-43%) reported in baseball pitchers 27 and the lower rate (6%) reported in hockey players. 17 AC joint pathology is prevalent in the asymptomatic middle-aged population, with up to 90% reported to have mild-to-moderate arthritic changes. 14,26 It is also well documented that changes identified in the AC joint on MRI poorly correlate with clinical symptoms. 21,38,42 It is possible that the rate of AC arthrosis is relatively low owing to distractive loads seen while hanging, as opposed to compressive and torsional loads seen in blocking and weightlifting activities.
The cartilage pathology identified in our study was unexpectedly severe. Climbers in this study had an average age of 34.1 years, yet 57% had cartilage changes on the humeral head, with a significant proportion having moderate to severe changes: 48% with modified Outerbridge grade 3 and 3% with grade 4. Interestingly, the glenoid cartilage was less severely affected than the humeral head; 19% of glenoids demonstrated cartilage changes, with 11% rated as grade 3 and 4% rated grade 4. This level of cartilage pathology was not identified in pitchers, hockey players, polo players, or volleyball players. 12,17,22,27 In an investigation of a population of amateur athletes with shoulder pain that evaluated the contralateral, asymptomatic shoulders of patients with an average age of 39.4 years, a more similar comparison group to our own, the prevalence of glenohumeral cartilage changes was only 0.8% to 3.3%. 3 One hypothesis for the observed high prevalence of labral tears and associated cartilage pathology is that these pathologies were secondary to acute instability events. However, given that no patient was noted to have a Hill-Sachs or Bankart lesion, and no patient recalled a history of instability events or had symptomatic instability on clinical evaluation, an instability origin is unlikely. It is possible that a sustained isometric upper extremity contraction, such as a hanging position coupled with an explosive climbing move (eg, reaching and swinging to a new hold), can lead to shearing events in the glenohumeral joint, which can cumulatively lead to labral and articular cartilage damage. These hypothesized pathomechanics will have to be investigated further to develop preventative strategies for symptomatic shoulder osteoarthritis at a young age.
Correlation of Physical Examination With MRI Findings
Climbers with labral tears identified in this study had significantly increased forward elevation compared with those without labral tears in both active (P = .026) and passive (P = .022) motion. While patients with labral tears had higher motion, all shoulders had, on average, range of motion at the highest end of normative values. 7 In baseball pitchers, posterior capsular tightness and internal impingement can lead to glenohumeral internal rotation deficit in which pitchers lose internal rotation but maintain a full arc of motion, compensating with increased external rotation. 1,10,36,41 In contrast, climbers maintain full external and internal rotation arc, in addition to increased forward elevation in shoulders with labral tears. It is possible that increased time spent at the extremes of motion can stress the labra, leading to increased rates of tearing.
Limitations
There are some limitations to the current study. Physical examinations were performed by multiple examiners. While all were in fellowship training in sports medicine, there is still variation in range of motion reporting and examination technique, which may have affected the clinical examination reporting. Radiology evaluation of MRI scans was performed by consensus review. This has the advantage of 2 expert musculoskeletal radiologist opinions; however, this approach precluded the possibility of calculating interrater reliability statistics. Furthermore, MRI interpretation has previously been reported to have a large amount of variability, specifically in rotator cuff 30,34 and labral pathology. 8,13,39 MRI scans in this study were reviewed by experts in the field of musculoskeletal radiology; however, the inherent variability in MRI interpretation may limit diagnostic accuracy and comparison to other MRI studies. Also, differences in MRI technique between this study, which used a 3.0-T field strength scanner, and many other studies that used 1.5-T field strength are difficult to quantify and define. A 3.0-T MRI study with greater resolution and signal contrast may be more sensitive and might be more likely to demonstrate changes compared with a 1.5-T examination. Also, techniques, understanding, and appreciation of imaging findings, as well as physical examination findings and their significance/meaning in the clinical patient, continue to evolve. There may be inherent uncertainty in comparing earlier with later studies. Finally, given that this study lacks a control group, it is impossible to report on the rates of MRI findings of the shoulders of climbers versus nonclimbers.
Conclusion
Study results indicated that positive findings on MRI are exceedingly common in the asymptomatic climber’s shoulder, especially in the glenoid labrum, articular cartilage, and biceps tendon. As always, correlation of imaging findings with clinical and physical examination is essential. Imaging, in particular MRI, is one part of the complete evaluation of the clinical patient for diagnosis and treatment planning.
Footnotes
Final revision submitted September 17, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.N.S. has received education payments from Southern Edge Orthopaedics. C.P.H. has received consulting fees from Smith & Nephew. T.R.H. has received hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vail Health Hospital (protocol No. 2018-33 v4).