
Abstract
Purpose:
This experimental study investigated the long head biceps tendon (LHBT) excursion that occurs at various positions of the upper limb during tendon stabilizing procedures. We hypothesized that shoulder abduction, elbow extension and forearm pronation would maximize the excursion of the LHBT and potential impacts on tendon stabilization.
Materials & Methods:
Forequarter specimens from 12 fresh frozen cadavers were used in this study. The study was performed at 0° and 30° of shoulder abduction. Elbow position was either 90° of flexion or full extension with the forearm either in full pronation or supination. A total of 14 combinations of positions were studied. A load of 55 N was applied to the distal biceps. The excursion of the proximal part of LHBT was measured for each of the different positions.
Results:
At a shoulder position of 30° of flexion, shoulder abduction of 30° created significantly greater excursion than 0° of shoulder abduction (p < 0.001). Both full extension of the elbow and full pronation of the forearm also showed significant excursion of the tendon when compared to supination (p < 0.001).
Conclusions:
The position of the shoulder, elbow and forearm has a significant effect on biceps excursion. Thirty degrees of shoulder abduction and 30° of forward flexion with the elbow in full extension and the forearm in full pronation maximizes excursion.
Clinical Relevance:
Information about the excursion of the LHBT affected by the position of the upper limb is useful for any biceps tendon stabilizing procedure. During an operation, the position of the upper limb should be monitored in order to maintain a proper anatomic length-tension relationship.
Introduction
Pathological conditions of the LHBT are a common cause of shoulder pain, 1,2 although some treatments of pathologies, e.g. repairing a rotator cuff without properly treating the LHBT lesion, may result in residual pain. Tenodesis is becoming more popular, especially for treating biceps pathologies in younger patients. 3 –6 Epidemiologic studies have shown that the number of procedures performed has risen between 2007 and 2011, with most performed in individuals between the age 30 and 59 years. 6 This procedures can prevent deformity and maintain a better strength of the elbow in the long term. 7 Even though the procedure has a high success rate, there are some reports of unsatisfactory results including biceps spasms/cramping (8%) and biceps pain (11%). 8,9 There is no clear explanation for these unpleasant symptoms after tenodesis. One possible cause is excessive tightness of the tendon after fixation.
The goal of tenodesis is pain relief while maintaining the function of the shoulder and elbow. Thus maintenance and restoration of LHBT length—tension relationship is very important for preserving muscle function with a proper tension. Hart et al. reported that the position of 30 degrees shoulder flexion, 40 degrees of shoulder abduction and 90 degrees of flexion of the elbow allows visualization of 56% of the LHBT from the bicipital groove. 10 This allows the LHBT to move freely and with high excursion. Anyway this study applied a load proximally while measuring the excursion, a situation which is different from the real world where the load usually comes from the distal part. 10 Lamplot et al. reported on the effect of various positions of the shoulder that could create excursion of the LHBT of up to 24.4 mm. 11 Unfortunately, the results of that study do not demonstrate how the change of the excursion relates to the position of the elbow. As the primary function of the biceps muscle has a direct effect on is the elbow and forearm functions, we believe a change in the position of the elbow and forearm would directly affect the length of the muscle-tendon unit. We further hypothesized that the position of the upper limb would affect the LHBT excursion, specifically that shoulder abduction, elbow full extension and forearm pronation would maximize the excursion of the LHBT.
Objectives
The primary objective of this study was to determine the amount of excursion of the LHBT under distal loading with different shoulder, elbow, and forearm positions.
Materials and methods
After the IRB was approved by the ethical board committee of the hospital, we conducted a study using upper limbs from fresh frozen donated cadavers. The whole-body specimens were thawed in a temperature-controlled room at 4 oC for 48 hours then left at room temperature until the specimens were soft and had regained full range of motion. We excluded specimens that had pathologies including restricted range of motion, previous surgery, rotator cuff tear, and biceps pathologies. Forequarter limb amputations were performed to free the limb from the torso. Then the skin was removed from the scapula to the proximal 1/3 of the forearm to allow identification of the biceps insertion on the radial tuberosity. The deltoid muscle was removed to reveal the rotator cuff and the proximal biceps tendon. The specimens were then inspected again to detect any pathologies of the rotator cuff and biceps tendon. A total of 12 healthy specimens (mean age 55.3 years; range, 38–72 years) were included in this study.
Specimen preparation
The specimens were mounted onto a stable pod by clamping the scapular body, setting the medial border perpendicular to the floor. A multiplanar external fixator was then applied to the limb. The first chance pin was placed on the humeral shaft at the level of the junction of the proximal and midshaft of the humeral bone and the second pin was placed at the level of the junction of the midshaft and the distal third. Both pins were carefully placed in the lateral plane to avoid penetration of the biceps muscle which might have affected the results of the study. Another chance pin was inserted into the glenoid neck of the scapula. An appropriate size fixator bar was attached to the pins through a single adjustable clamp. This created two sets of pins, a humerus set and scapular set, which were connected by a tube to tube clamp. The purpose of the fixator was to create a stable shoulder position during testing. Next, the distal biceps tendon was identified and weight was applied to the tendinous part just before insertion into the radial tuberosity. A load of 55 N on the distal biceps was created using a hanging sandbag. The force of the load was confirmed using a digital scaler (Figure 1).

1. Demonstration of specimen setup and measurement of the distance between the two needles representing the excursion of the LHBT.
Positioning of specimens
Different combinations of positions of the shoulder, elbow and forearm were tested. The positions were selected based on positions regularly used while performing surgery; the two main positions were the beach chair and the lateral decubitus positions. To simulate the beach chair position, we locked the external fixator at 0° shoulder glenohumeral (GH) abduction. With the beach chair position, we also studied the effect of glenohumeral rotation including 30o internal rotation, neutral rotation and 30o external rotation. In each case, the elbow was set at 90° flexion and full extension. Since the biceps tendon inserts into the radius and forearm rotation affects the movement of the tendon, we studied both full supination and full pronation. In the beach chair position, we investigated several combinations: 3 shoulder positions (30o internal rotation (IR), neutral (N), and 30o external rotation (ER), 2 elbow positions (90° flexion and full extension) and 2 forearm positions (pronation and supination) making a total of 12 combinations. To replicate the lateral decubitus position, we locked the external fixator at 30° GH abduction in neutral rotation and 30° forward flexion with full extension of the elbow. We then studied the effect of full supination and full pronation on the excursion of the tendon. The lateral decubitus position created another 2 combinations (supination and pronation), bringing the total number of position combinations to 14.
Measurement of excursion
To measure excursion, we started with the limb in a position with the shoulder in 0o of abduction, the elbow in 90° of flexion and the forearm in neutral rotation. We marked the tendon at a level one centimeter below the transverse humeral ligament using an 18-gauze needle. Then 55 N force was applied to the distal tendinous part of the biceps at the elbow level. The shoulder, elbow and forearm were set at each of the positions previously described, i.e. the 14 combinations. After each position was set, another 18-gauge needle was placed using same reference point, i.e. one centimeter below the transverse humeral ligament, and the distance between the two needles was measured using a digital Vernier caliper (Figure 1). That distance represents the excursion of the LHBT that occurred due to the load and the position of shoulder, elbow and forearm.
Statistical analysis
A sample size of 12 was calculated to be the required number of shoulders. Data were analyzed using the paired t-test to compare the data of 2 set which were the comparing the position of the elbow and the forearm. One-way analysis of variance (ANOVA) was used to compare the data among 3 or more sets. Statistical significance was defined as p values of 0.05 or lower.
Results
The data analysis found no statistically significant effect of glenohumeral rotation on the excursion of the LHBT (Table 1). However, having the elbow in full extension (EB 0°) significantly increased the excursion of the LHBT compared to the 90° elbow flexion position (EB 90o) (p < 0.05) (Figure 2). Additionally, full pronation of the forearm significantly increased the excursion of the LHBT compared to the full supination position (<0.05) (Figure 3). The position of the shoulder also significantly affected excursion. The position of 30° abduction and 30° forward flexion created significantly greater excursion compared to 0° abduction and 0° forward flexion with the same position of elbow and forearm (p < 0.05) (Figure 4).
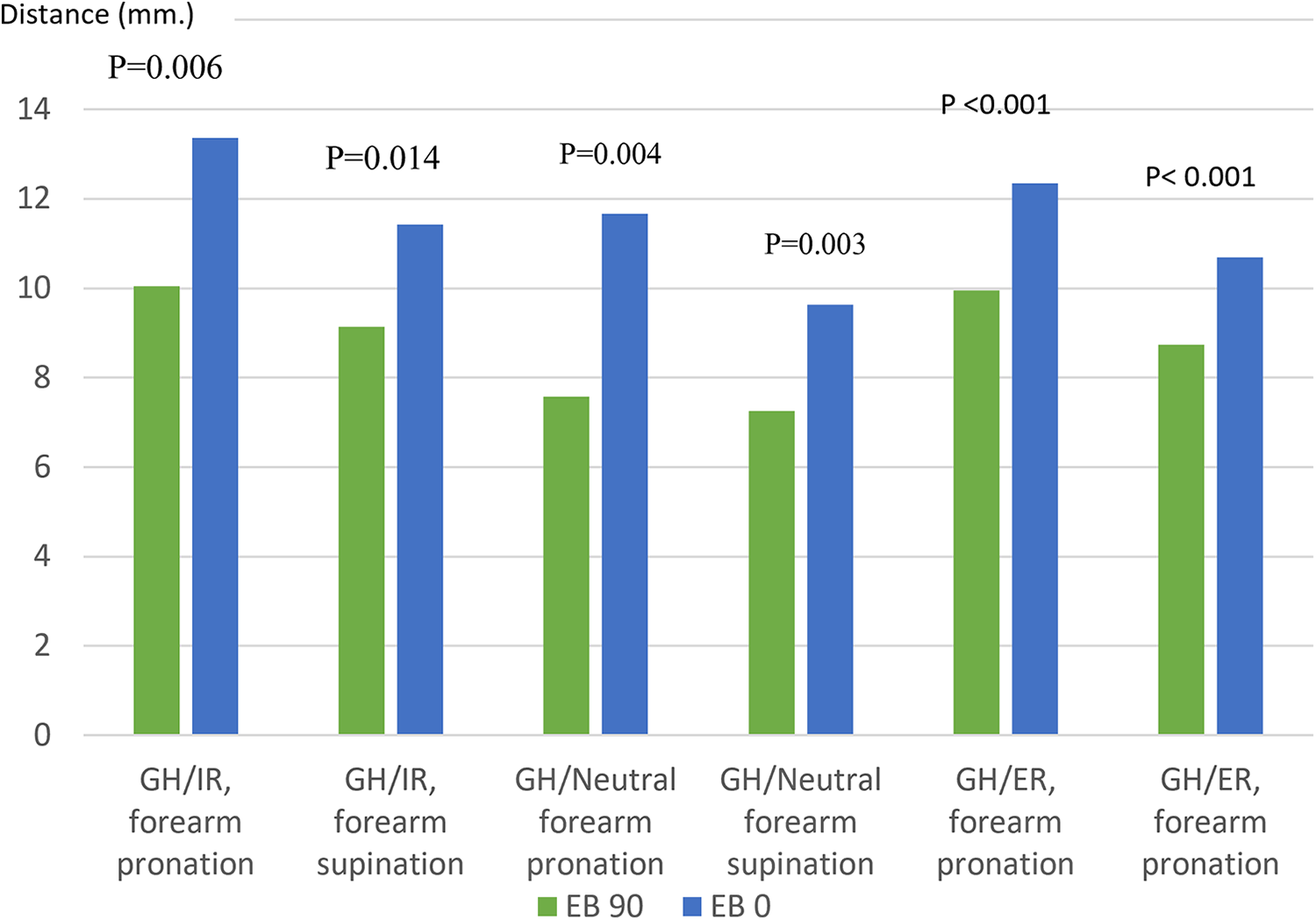
Effect of elbow position on LHBT excursion (GH/IR = Glenohumeral internal rotation, GH/Neutral = Glenohumeral neutral rotation, GH/ER = Glenohumeral external rotation, EB 90 = elbow at 90° flexion, EB 0 = elbow at full extension).

Effect of forearm position on LHBT excursion (GH0/0 = Glenohumeral 0° abduction and 0° forward flexion, GH30/30 = Glenohumeral 30° abduction and 30° forward flexion, IR = Glenohumeral internal rotation, N = Glenohumeral neutral rotation, ER = Glenohumeral external rotation, EB 90 = elbow 90° flexion, EB 0 = elbow full extension).
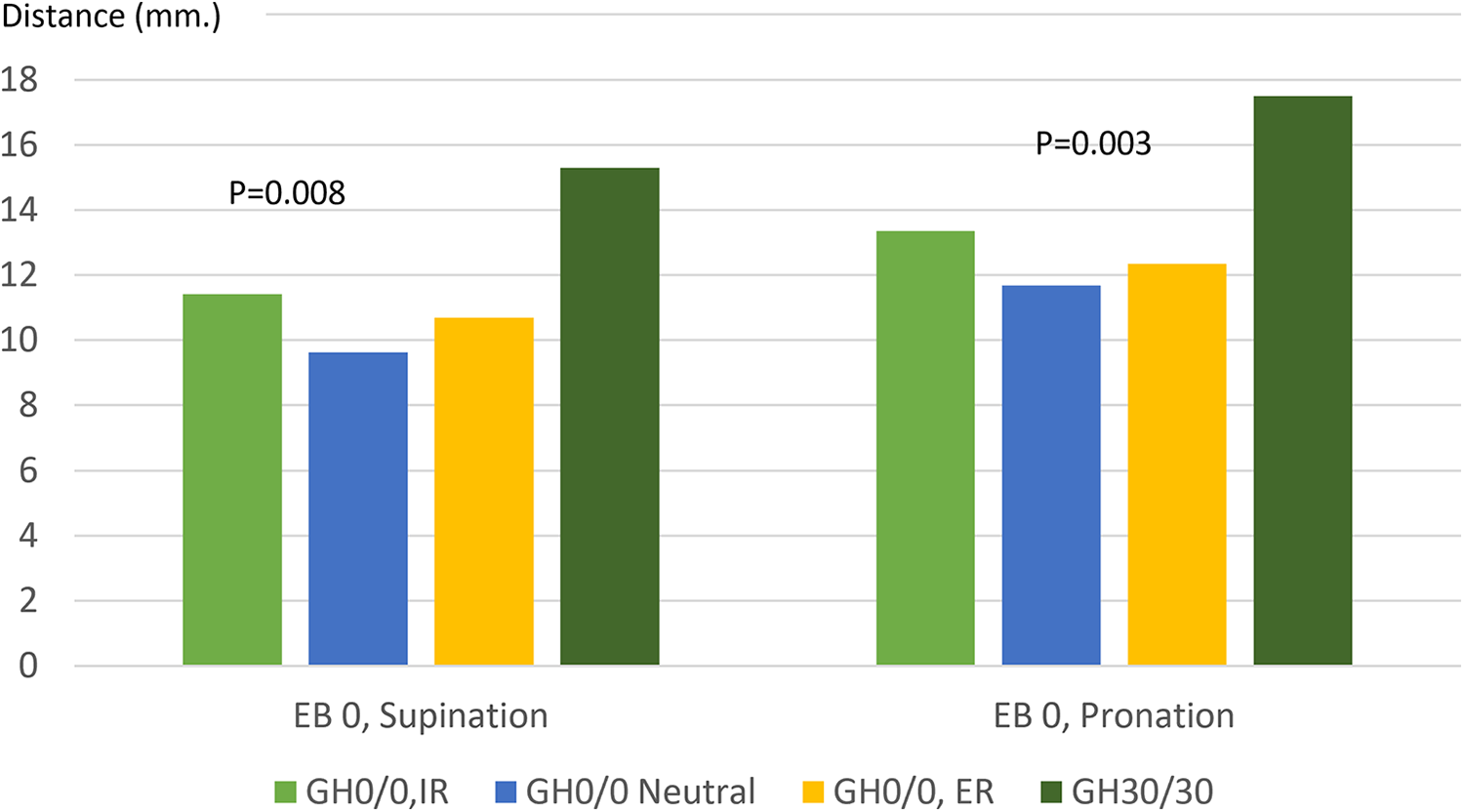
The effect of shoulder position on the excursion of the LHBT (EB 90 = elbow 90° flexion, EB 0 = elbow full extension, Supination = forearm supination, Pronation = forearm pronation).
Excursion value in various positions of shoulder, elbow and forearm under load.

GH = glenohumeral, IR = internal rotation, ER = external rotation, EB = elbow.
Discussion
Results from this study indicate a significant change of excursion of LHBT occurs under distal load and that the amount of that excursion is determined by the position of the shoulder, the elbow and the forearm. These findings differ from the results of a previous study which reported that the position of the elbow does not affect the excursion of the tendon. 11 This difference between the two studies can be explained by variations in the extension position of the elbow and the pronation of the forearm which oppose functions of the tendon, i.e. elbow flexion and supination, which lengthen the tendon and produce a significant change in the extent of excursion. These findings of the present study may explain the over-tension condition that sometimes occurs during a biceps stabilizing procedure such as biceps tenodesis, when the procedure is performed in the least excursion stage. There have been no specific force recommendations for testing the excursion of the biceps, with most studies recommending using a force between 5–67 N. 10,12 –14 Some studies reported loading the tendon proximally; we think, however, that it is more appropriate to load the biceps distally. 10 Loading the biceps tendon distally is very important as it simulates the usual activity of the patient in which the load is applied to hand, e.g. lifting an object. A peak force of 55 N was used in this study because this is the approximate force generated in the biceps throughout the range of motion of the elbow with no distal resistance other than the weight of the arm. 15,16
Arthroscopic rotator cuff repair has become a standard procedure for treating a torn rotator cuff. Pathology of the LHBT is one of the common concomitant pathologies which need to be treated in the same occasion. Commonly used patient positions for performing shoulder arthroscopy include the beach chair position and the lateral decubitus position. These two positions are associated with different shoulder, elbow and forearm positions during surgery. For example, while performing shoulder arthroscopy in the beach chair position, the shoulder should be in a position of 0° abduction and 0° forward flexion. Often while the surgeon is performing biceps tenodesis, an assistant holds the elbow and the forearm in various positions without being aware of the effect of the specific position on the excursion of the LHBT. Increased awareness of the effect of position of the upper extremity could potentially improve the success of biceps tenodesis operations. Stabilizing the position of the shoulder at 30° of abduction and 30° of forward flexion with the elbow in full extension and the forearm in pronation prior to setting the tension of LBHT can minimize the risk of over-tension. Rather than starting surgery by performing a tenotomy, we recommend first releasing the transverse humeral ligament and then setting the position of shoulder, elbow and forearm to obtain a maximal excursion, then marking the tendon where the bone tunnel for the tenodesis will be created. After that, the routine tenotomy and tenodesis procedure can be performed. While pulling the LHBT into the tenodesis hole, the reference points should be checked to make sure they remain at the original spot to avoid over-tension.
Data from North America show that the number of tenodesis procedures almost doubled in the 4 years between 2008 and 2011. 17 Even though tenodesis is performed both to improve the strength of the elbow as well as for cosmetic reasons, it is not without sequelae: the reported failure rate of the procedure ranges from 0% to 19%. 18,19 Failure can result from both controllable and uncontrollable factors. Uncontrollable factors include bone density and the quality of the tendon. Low bone density and the type of implant fixation together can be the cause of failure due to poor fixation strength. Also, fixation in a condition of high tension results in a high pull-out force. Advanced pathology of the tendon can be a cause of residual pain and retearing. Differences in surgical technique represent another potentially important contributing factor to failure. Too much tension while fixing the LHBT may create a high pull-out tension on the tendon. High tension on the LHBT can affect the biceps tone which may explain residual clamping pain. Surgical technique is one of the important controllable factors: surgeons need to be aware of the proper length and tension of the LHBT while performing a biceps stabilizing procedure.
Our study has some limitations. First, our model studied the LHBT excursion in fresh cadavers using methods which are difficult to replicate in a living person. For example, there was no muscle tone in other muscles of the cadavers that could produce force on the shoulder and elbow joints which might have affected the excursion values. Second, we could not determine if the observed excursion might be related to the cramping pain that occurs in some patients after surgery. Additionally, it was not possible to determine the strength of the LBHT after performing the tenodesis based solely on the observed excursion. Further clinical studies should be conducted to demonstrate that the value of excursion does not affect the strength of the biceps muscle and that this method results in good clinical outcomes. Lastly, our experiment was done only with forequarter specimens; motion of the shoulder in real patients could be potentially affect LBHT excursion. Abduction of the shoulder is always combined with motion of the scapulothoracic and glenohumeral joint, but in this study, we set a position of 30° abduction by measuring the glenohumeral joint; there could be a higher degree of shoulder abduction in a real patient.
Conclusions
The positioning of the shoulder, elbow and forearm during surgery affects the excursion of the LHBT. Thirty degrees of shoulder glenohumeral abduction and 30° of forward flexion with the elbow in full extension and the forearm in the full pronation position is recommended to provide maximal excursion during biceps tenodesis.
Footnotes
Acknowledgments
The authors would like to express their sincere thanks to Dr.Lamar Robert, PhD, and Assoc. Prof. Chongchit Sripun, PhD, for editing the English manuscript and also Mrs.Areerak Phanphaisarn for helping to confirm statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. Specimens were donated to Chiangmai University hospital.