
Abstract
Background:
Football has one of the highest injury rates (IRs) in sports, ranging from 4.1 to 8.6 per 1000 athlete-exposures (AEs). Previous research has reported that athletes may be at an increased risk of suffering lower extremity (LE) injuries after a concussion.
Purpose/Hypothesis:
The purpose of this study was to evaluate the rate of LE injuries in collegiate football athletes after a concussion. We predicted that the overall LE IR would increase after a concussion and that each position group would also demonstrate a similar increase in LE injuries after a concussion.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Daily attendance and injury records were prospectively collected by licensed team medical providers for the 2012 through 2016 college football regular seasons. Each injury report included the date of injury, position group, body part injured, and type of injury. IRs per 1000 AEs with 95% CIs were calculated to evaluate LE injuries at different time points after a concussion (remainder of season, next season, any additional seasons) and by months (<6 months, 6-12 months, >12 months). Mid-P exact tests were utilized to establish injury rate ratios (IRRs) to compare the IR between variables.
Results:
There was no significant difference in LE IRRs between the athletes post- versus preconcussion (P = .20) or between the postconcussion and no concussion (control) athletes (P = .08). There was an increased LE IR beyond 12 months in the postconcussion group (IR, 9.08 [95% CI, 3.68-18.89]) compared with the no concussion group (IR, 2.88 [95% CI, 2.04-3.96]) (IRR, 3.16 [95% CI, 1.21-7.15]; P = .02). Line position players had an increase in LE injuries after a concussion (IRR, 6.22 [95% CI, 1.31-23.68]; P = .03) compared with linemen with no concussion.
Conclusion:
There was no initial increase in LE IRs immediately after a concussion; however, there was an increased LE IR more than 12 months after a concussion. There was no increase in LE IRs demonstrated by skill and other position groups. Line position players experienced an increased LE IR the next season after a concussion or greater than 12 months after the injury.
Football is one of the most popular sports in the United States, with more than 250,000 children aged 5 to 14 years, over 1 million high school students, and 60,000 collegiate athletes participating annually. 2 –4,9,19,26,33 However, it has experienced a recent decline in participation because of concerns of player safety. 3,35 Football has one of the highest injury rates (IRs) in competitive sports, ranging from 4.1 to 8.6 per 1000 athlete-exposures (AEs). 3,12,23,27,33,34 Zuckerman et al 37 examined the epidemiology of concussions in 25 collegiate sports over a 5-year span and found that football had the greatest incidence of concussions (n = 603) but only the fourth-highest concussion IR in collegiate athletics (6.71/1000 AEs). Because of high participation rates and IRs, football player safety is a heavily scrutinized topic. §§ Concussions are at the forefront of this scrutiny because of the potential short- and long-term effects on a player’s brain and body.
The incidence of concussions in National Football League games has increased from 0.41 in 1996 to 0.66 concussions per game in 2014. 8 USA Football integrated the “Heads Up Football” program into youth and high school football programs to educate coaches on how to teach proper, safe tackling techniques to improve safety at the grassroots level. 19 These techniques are associated with lower IRs and a decreased number of head impacts in practice. 15,19 In 2008, the National Collegiate Athletic Association (NCAA) implemented and emphasized “targeting” in further efforts to decrease the number of head injuries in collegiate football by penalizing players who initiate contact with another player’s head or neck region. 36 In addition, in 2013 the penalty applied was increased to further emphasize and discourage this dangerous playing technique. 17 Despite numerous efforts, concussions continue to be a focus of improvement in player safety. 12,18,20,35,37
Athletes may be at an increased risk of lower extremity (LE) injuries after a sustained concussion. 5 –7,16,24,28,29,31,32 Although an athlete may appear fully recovered, subtle brain and motor function deficits may linger and might not be easily identified. 5 –7,16,24,28,29,31 These underlying deficits may negatively affect gait and balance for an extended duration compared with the duration of common concussion symptoms. 6,7,30
The purpose of this study was to evaluate the rate of LE injuries in collegiate football athletes after a sustained concussion. Athletes were divided into similar position groups to evaluate if the demands of certain football positions predisposed them to LE injuries after a concussion. The hypothesis was that the overall LE IR would increase after a concussion and that each position group would demonstrate a similar increase in LE IRs after a concussion compared with a no concussion (control) group and with their collegiate performance before the concussion (preconcussion). In addition, the rate of LE injuries were evaluated at different time points after a concussion (remainder of season, next season, any additional seasons) and by months (<6 months, 6-12 months, >12 months). Understanding the specific time frame when athletes are more susceptible of sustaining LE injuries after a concussion may help future efforts to optimize player safety in football.
Methods
Daily attendance and injury records were prospectively collected during the fall regular season between the 2012 to 2016 seasons for a single Division I college football program. One regular season was defined as every game or practice from the first fall preseason practice to the last regular-season or conference championship game. All attendance and injury records were documented by a licensed team medical provider. This study was approved by an institutional review board.
The reportable injury definition from the NCAA Injury Surveillance System (ISS) was applied, which defined an injury as one that (1) occurred as a result of participation in an organized intercollegiate practice or contest, (2) required medical attention by a team certified athletic trainer or physician, and (3) resulted in restriction of the student-athlete’s participation or performance for ≥1 calendar days beyond the day of injury. 1 Injury reports were completed by a certified athletic trainer or team physician specializing in sports medicine. Each injury report included details of the injury, such as the date, position group, body part injured, and type of injury. The type of injury included contusion, strain, sprain, stinger/brachial plexopathy, dislocation, rupture, concussion, and other. The location of injury was divided into foot, ankle, lower leg and shin, knee, upper leg and thigh, hip, chest, shoulder, elbow, wrist and hand, and head and neck.
In addition, players were divided into 3 groups based on the physical demands and skills required for each position: line, skill, and other. The line position group consisted of offensive and defensive linemen. The skill position group consisted of wide receivers, running backs, and defensive backs. The other position group consisted of quarterbacks, tight ends, linebackers, and specialists, whose tasks fall between the speed and cutting of the skill group and the short powerful bursts of the line group.
Attendance sheets were utilized to document an athlete not participating because of an injury. One AE was defined as a single athlete who participated in either 1 organized game or practice. 11 The IR was calculated per 1000 AEs along with the 95% CI for all recorded variables. To evaluate the rate of LE injuries after a concussion, IRs were calculated by both postconcussion season (rest of season, next season, and additional seasons) and time period (<6 months, 6-12 months, >12 months). These were used to try to help pinpoint a specific time frame, as the season is only 4 to 5 months out of the year and the time of injury in the season may affect the results. The fall football regular season runs from August to the end of November or early December. To compare IRs between the concussion groups (preconcussion and postconcussion) and the no concussion (control) group, mid-P exact tests were utilized to calculate injury rate ratios (IRRs). Statistical significance was established at P ≤ .05.
Results
Over the 5-year course of the 2012 to 2016 college football seasons, written informed consent was received from 62 incoming collegiate athletes that resulted in 180 monitored athlete-seasons, for a total of 15,483 AEs. Concussions were sustained by 12 of the 62 (19.4%) players, and these athletes comprised the concussion group. There were 21 athletes in the line position group, but only 2 line players sustained a concussion (9.5%). The skill position group had 26 athletes, with 6 players suffering a concussion (23.1%). The other position group included 15 athletes, with 4 who sustained a concussion (26.7%). Overall, there were 49 LE injuries and 16 concussions in this group. Three athletes sustained multiple concussions, including 2 skill position players and 1 line position player. One line and 1 skill position player each sustained 2 concussions, and 1 skill position player sustained 3 concussions.
The skill position players had an overall concussion IR of 1.22 (95% CI, 0.56-2.31), the line position players had an IR of 0.73 (95% CI, 0.23-1.77), and an IR of 1.16 (95% CI, 0.37-2.81) was calculated for the other position players. There was no difference in the overall concussion IR between any of the position groups. Skill position players demonstrated an increased LE IR compared with line position players in both the concussion group (IRR, 2.58 [95% CI, 1.29-5.51]; P = .006) and the no concussion group (IRR, 3.30 [95% CI, 1.45-8.30]; P = .004). There were no other IR differences between the position groups.
The LE IR was 2.62 injuries per 1000 AEs for the preconcussion group and 5.59 injuries per 1000 AEs for the postconcussion group (Table 1). The no concussion group sustained 35 LE injuries in 12,166 AEs, for an IR of 2.88 per 1000 AEs.
Overall Injuries and Exposures a
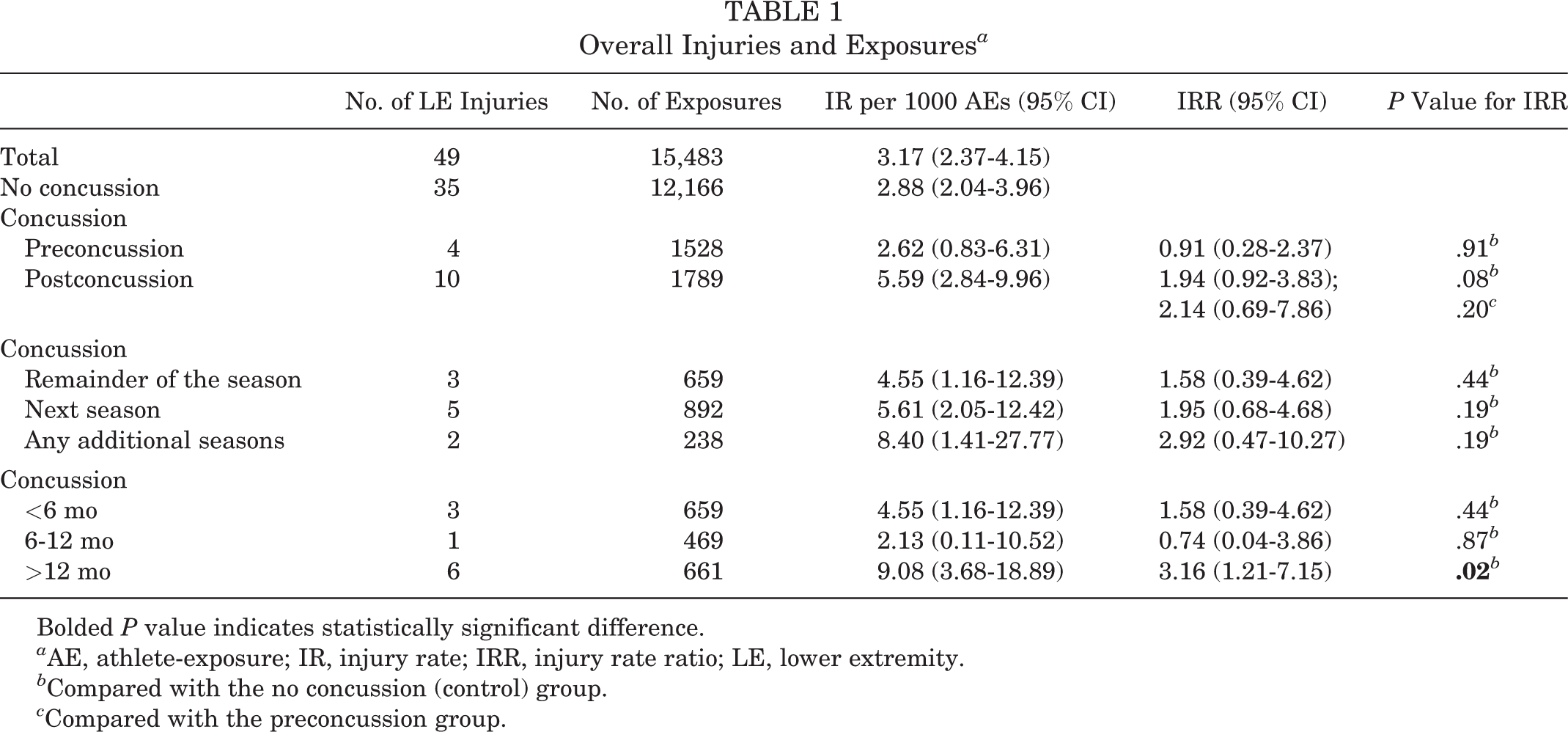
Bolded P value indicates statistically significant difference.
a AE, athlete-exposure; IR, injury rate; IRR, injury rate ratio; LE, lower extremity.
b Compared with the no concussion (control) group.
c Compared with the preconcussion group.
Overall, there was an increased LE IR beyond 12 months in the concussion group compared with the no concussion group (P = .02). There was no significant increase in IRRs in the postconcussion group compared with the no concussion group or the preconcussion group (P = .08 and .20, respectively). In addition, there were no differences in IRRs at any specific time period or point in the season for the postconcussion group compared with the no concussion group or preconcussion group (all P > .16). The athletes in the preconcussion group demonstrated no difference compared with those in the no concussion group (IRR, 0.91; P = .91).
Skill Players
The 20 skill athletes with no concussion in the study had an LE IR of 4.62 per 1000 AEs (Table 2). There was no difference compared with the LE IR of the preconcussion group (P = .78). The IRR of the postconcussion group was not significantly different compared with that of the no concussion group or preconcussion group (P = .57 and .53, respectively). There was no significant difference in IRRs in any time period or season in the postconcussion group compared with the no concussion group (all P > .56) or preconcussion group (all P > .77).
Skill Position Group Injuries and Exposures a

a AE, athlete-exposure; IR, injury rate; IRR, injury rate ratio; LE, lower extremity.
b Compared with the no concussion (control) group.
c Compared with the preconcussion group.
Compared with the line group, the skill position group demonstrated a statistically significant increase in LE injuries overall (P = .006) as well as in the control group (P = .04); however, there was no difference in LE injury rates postconcussion between skill and line position groups (P = .59).
Line Players
The line position group included 21 athletes, and only 2 line athletes sustained a concussion during 5 years in the regular season (Table 3). The no concussion group suffered 7 LE injuries, with an IR of 1.40 per 1000 AEs. The line athletes who sustained a concussion had no reported preconcussion LE injuries but 3 LE injuries after their concussion.
Line Position Group Injuries and Exposures a

Bolded P value indicates statistically significant difference.
a AE, athlete-exposure; IR, injury rate; IRR, injury rate ratio; LE, lower extremity.
b Compared with the no concussion (control) group.
For the line position group, there was an increased LE IR in the postconcussion group when compared with the no concussion group (P = .03). There was also an increased LE IR for line position players in the first full season after a concussion compared with the no concussion group (P = .05). When analyzed by time frame after a concussion, there was an increased IR for line position players more than 12 months after a concussion compared with the control group (P = .02). However, there was no difference in LE IRs by line position players immediately after a concussion in any comparison (P = .23).
Other Players
The other position players with no concussion sustained a total of 6 LE injuries (IR, 2.49/1000 AEs [95% CI, 1.01-5.18]). The other position players who sustained a concussion only suffered a total of 2 LE injuries (Table 4). There was 1 LE injury sustained in the preconcussion group (IR, 1.68/1000 AEs [95% CI, 0.08-8.29]) and 1 LE injury sustained in the postconcussion group (IR, 2.29/1000 AEs [95% CI, 0.12-11.31]). There was no significant difference in IRs between athletes who sustained a concussion and athletes who had no concussion (all P > .80).
Other Position Group Injuries and Exposures a

a AE, athlete-exposure; IR, injury rate; IRR, injury rate ratio; LE, lower extremity.
b Compared with the no concussion (control) group.
c Compared with the preconcussion group.
Discussion
Previous research has demonstrated that skill position players experienced the greatest proportion of injuries to the LE compared with line and other position players. 21 There was no significant overall increase in LE IRs between the preconcussion and postconcussion groups. There was also no difference in LE IRs between the concussion and no concussion groups. The only overall increase was observed in the postconcussion group’s LE IR for the time period beyond 12 months after a concussion when compared with the control group. These findings did not support our overall hypothesis regarding a clear increase in LE IRs after an athlete sustains a concussion.
Our findings did not support our hypothesis that each position group would demonstrate a similar increase in LE IRs after a concussion. To our knowledge, this is one of the first studies to analyze LE IRs after a concussion and analyze the role of the position group.
Lynall et al 24 compared the LE IRs of 44 collegiate athletes after a concussion with a matched control group for 90, 180, and 365 days and determined that a significant increase in LE injuries occurred in the 180- and 365-day comparisons but not in the initial 90 days after a concussion. Unfortunately, only 25% (11/44) of the concussion population competed in football, also making the sample size extremely small. Herman et al 16 reported a similar significant increase in LE injuries in the first 90 days after a concussion during the remainder of the season to a matched control group of 56 players.
Numerous non-football–specific studies have evaluated this topic. Brooks et al 5 reported an increase in acute LE musculoskeletal injuries the first 90 days after returning to play in 87 cases from 7 sports at a single institution. Lynall et al 25 reported that high school athletes from 27 different sports demonstrated increased odds of sustaining a time-loss, acute LE musculoskeletal injury after a concussion. This increase was not observed in non–time-loss LE musculoskeletal injuries. 25 Even professional rugby players demonstrated a 60% increased risk of time-loss injuries after a concussion the remainder of the season. 10 These non-football–specific studies indicate increased LE IRs immediately after a concussion. The differences in results may be caused by small sample sizes, or they may demonstrate the importance of this topic specifically to each individual sport and/or level of competition. These studies were performed on high school to professional athletes across numerous different sports and may indicate a significant challenge in our ability to find a universal rule regarding the musculoskeletal injury risk after a concussion.
Our analysis demonstrated several similar findings to the Lynall et al 24 study. There was no increase in LE IRs immediately after a concussion (<6 months or rest of season) in the postconcussion group compared with the no concussion group, however there was a significant increase in LE injuries greater than 12 months after a concussion. This increase was not demonstrated when analyzed by position groups. We hesitate to make any major interpretation from the position group data, as these data are underpowered, but from the preliminary data, only the line position group demonstrated a difference in LE IRs after a concussion. This increase was noted in the first full regular season after a concussion or more than 12 months after a concussion (P = .05 and .02, respectively), depending on the time interval variable analyzed. The exact reason could be from a number of confounding or incidental variables. This topic is important as the exact mechanism of this proposed increased injury risk is not clearly known and is likely multifactorial. One would expect that if there were persistent neuromuscular deficits after a concussion that contributed to future LE injuries, this association would be greatest in the earlier periods after a concussion. Over time, these neuromuscular deficits may improve, and the risk of LE injuries, unless participation were limited, would decrease over time.
However, there are many unique challenges to accurately evaluating LE injuries after a concussion. Football has one of the highest IRs of all competitive sports and a documented high LE IR. 15,23,35 Just over half of all football injuries (50.4%) from 2004 to 2009 in the NCAA ISS involved the LE. 14 In addition, the rate of reinjuries for NCAA football over that time period was roughly 13%. 14 The described risk of LE injuries after a concussion may be related to other effects of concussions, such as physical deconditioning. These confounding factors stress the importance of large-scale collaborative efforts to power postconcussion LE studies and evaluate other injury characteristics (ie, mechanism of injury, type of exposure).
These collaborations can introduce additional bias through differences in medical and coaching staff members that result in different practice styles, drills, and treatment protocols. Several studies 5,16,24 have combined multiple sports that confound the results as the injury risks and physical requirements of each sport are unique, as demonstrated by significant differences in IR patterns. In addition, collegiate off-seasons are limited in the number of coach-guided training sessions and practices and instead mainly rely on individual or small-group sport-focused sessions, player-led practices, and strength and conditioning workouts. These exposures are challenging to monitor and do not follow a clear schedule compared with the regular season, although the general consensus is that off-season exposures have a lower IR compared with in-season injuries.
Limitations
This small-scale study observed a single collegiate football program and included 64 athletes over the course of 5 seasons. There was no prestudy power analysis. This resulted in an extremely small sample size in which athletes were broken up into position groups (ie, skill, line, and other) and underpowered our position group analyses. Because of the small sample size, we did not factor when during the season the concussion was sustained, length of symptoms, or time lost from a concussion. Instead, this study focused on the relationship of concussions and LE injuries.
A significant challenge is to obtain accurate records of all LE injuries and concussions in the off-season, as coach-directed practice and training sessions are limited. In addition, players’ medical injury history before competition at this institution were not accurately known, and athletes may have sustained previous concussions. Our study lacked matched controls and may have introduced participation bias as it is possible that the relationship between a concussion and LE injury is a function of rates of exposure (ie, starter vs reserve player).
Conclusion
There was no initial increase in LE IRs immediately after a concussion; however, there was an increased LE IR more than 12 months after a concussion. There was no increase in LE IRs demonstrated by skill and other position groups. Line position players experienced an increased LE IR the next season after a concussion or greater than 12 months after an injury.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by The Ohio State University’s Department of Athletics. The authors acknowledge funding support from National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases grants R01AR55563 and R01AR056259 to T.E.H.
Ethical approval for this study was obtained from The Ohio State University Biomedical Sciences Institutional Review Board.